

Blood Pressure (BP)
What is Blood pressure (BP)?
Blood pressure (BP) is the pressure of circulating blood on the walls of blood vessels. Used without further specification, “blood pressure” usually refers to the pressure in large arteries of the systemic circulation. Blood pressure is usually expressed in terms of the systolic pressure (maximum during one heart beat) over diastolic pressure (minimum in between two heart beats) and is measured in millimeters of mercury (mmHg), above the surrounding atmospheric pressure.
Blood pressure is one of the vital signs, along with respiratory rate, heart rate, oxygen saturation, and body temperature. Normal resting blood pressure in an adult is approximately 120 millimetres of mercury (16 kPa) systolic, and 80 millimetres of mercury (11 kPa) diastolic, abbreviated “120/80 mmHg”.
Traditionally, blood pressure was measured non-invasively using a mercury-tube sphygmomanometer, or an aneroid gauge, which is still generally considered to be the gold standard of accuracy for auscultatory readings. More recently other semi-automated methods have become common, largely due to concerns about potential mercury toxicity, although cost and ease of use have also influenced this trend. Early automated alternatives to mercury- tube sphygmomanometers were often seriously inaccurate, but validated devices have better accuracy to mercury devices, if you allow an error of equal to or less than 5 mm Hg and a standard deviation of equal to or less than 8 mm Hg.
Blood pressure is influenced by cardiac output, total peripheral resistance and arterial stiffness and varies depending on situation, emotional state, activity, and relative health/disease states. In the short term, blood pressure is regulated by baroreceptors which act via the brain to influence nervous and endocrine systems.
Blood pressure that is low is called hypotension, and pressure that is consistently high is hypertension. Both have many causes. and may be of sudden onset or of long duration. Long-term hypertension is a risk factor for many diseases, including heart disease, stroke and kidney failure. Long-term hypertension is more common than long-term hypotension, which often goes undetected because of infrequent monitoring and the absence ofsymptoms.
The risk of cardiovascular disease increases progressively above 115/75 mmHg. In practice blood pressure is considered too low only if noticeable symptoms are present.
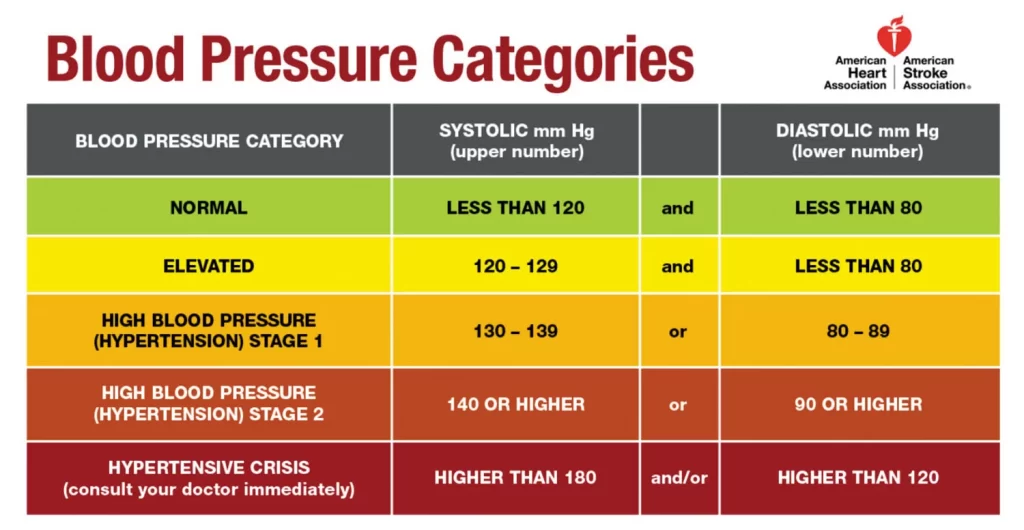
Observational studies demonstrate that people who maintain arterial pressures at the low end of these pressure ranges have much better long term cardiovascular health. There is an ongoing medical debate over what is the optimal level of blood pressure to target when using drugs to lower blood pressure with hypertension, particularly in older people. The table shows the classification of blood pressure adopted by the American Heart Association for adults who are 18 years and older. It assumes the values are a result of averaging resting blood pressure readings measured at two or more visits to the doctor.
Blood pressure fluctuates from minute to minute and normally shows a circadian rhythm over a 24-hour period, with highest readings in the early morning and evenings and lowest readings at night. Loss of the normal fall in blood pressure at night is associated with a greater future risk of cardiovascular disease and there is evidence that night-time blood pressure is a stronger predictor of cardiovascular events than day-time blood pressure.Also, an individual’s blood pressure varies with exercise, emotional reactions, sleep, digestion and time of day (circadian rhythm).
Various other factors, such as age and sex, also influence a person’s blood pressure. In children, the normal ranges are lower than for adults and depend on height. Reference blood pressure values have been developed for children in different countries, based on the distribution of blood pressure in children of these countries.As adults age, systolic pressure tends to rise and diastolic pressure tends to fall.Consequently, in the elderly, systolic blood pressure often exceeds the normal adult range, this is thought to be due to increased stiffness of the arteries.
Differences between left and right arm blood pressure measurements tend to be small. However, occasionally there is a consistent difference greater than 10 mmHg which may need further investigation, e.g. for obstructive arterial disease.
Reference ranges for blood pressure in children
Stage Approximate age Systolic Diastolic
Infants 1 to 12 months 75–100 50–70
Toddlers and preschoolers 1 to 5 years 80–110 50–80
School age 6 to 12 years 85–120 50-80
Adolescents 13 to 18 years 95–140 60–90
MEAN ARTERIAL PRESSURE
The mean arterial pressure (MAP) is the average over a cardiac cycle and is determined by the cardiac output (CO, systemic vascular resistance (SVR), and central venous pressure (CVP)
MAP =(CO.SVR) +CVP
In practice the contribution of CVP (which is small) is generally ignored and so
MAP=CO.SVR
MAP can be estimated from measurements of the systolic pressure P(systolic) and the diastolic pressure P(diastolic).
so,
MAP = P (diasolic) +1/3 P (P sys – p dias)
PULSE PRESSURE
P pulse = ( P systolic – P diastolic )
Curve of the arterial pressure during one cardiac cycle. The closing of the aortic valve causes the notch in the curve.
The pulse pressure is the difference between the measured systolic and diastolic pressures.
The up-and-down fluctuation of the arterial pressure results from the pulsatile nature of the cardiac output, i.e. the heartbeat. Pulse pressure is determined by the interaction of the stroke volume of the heart, the compliance (ability to expand) of the arterial system—largely attributable to the aorta and large elastic arteries—and the resistance to flow in the arterial tree. By expanding under pressure, the aorta absorbs some of the force of the blood surge from the heart during a heartbeat. In this way, the pulse pressure is reduced from what it would be if the aorta were not compliant. The loss of arterial compliance that occurs with aging explains the elevated pulse pressures found in elderly patients.
SYSTEMIC VENOUS PRESSURE
Blood pressure generally refers to the arterial pressure in the systemic circulation. However, measurement of pressures in the venous system and the pulmonary vessels plays an important role in intensive care medicine but requires invasive measurement of pressure using a catheter.
Venous pressure is the vascular pressure in a vein or in the atria of the heart. It is much less than arterial pressure, with common values of 5 mmHg in the right atrium and 8 mmHg in the left atrium. Blood pressure (BP) is the pressure of circulating blood on the walls of blood vessels. Used without further specification, “blood pressure” usually refers to the pressure in large arteries of the systemic circulation. Blood pressure is usually expressed in terms of the systolic pressure (maximum during one heartbeat) over diastolic pressure (minimum in between two heart beats) and is measured in millimeters of mercury (mmHg), above the surrounding atmospheric pressure.
Blood pressure is one of the vital signs, along with respiratory rate, heart rate, oxygen saturation, and body temperature. Normal resting blood pressure in an adult is approximately 120 millimetres of mercury (16 kPa) systolic, and 80 millimetres of mercury (11 kPa) diastolic, abbreviated “120/80 mmHg”.
Traditionally, blood pressure was measured non-invasively using a mercury-tube sphygmomanometer, or an aneroid gauge, which is still generally considered to be the gold standard of accuracy for auscultatory readings. More recently other semi-automated methods have become common, largely due to concerns about potential mercury toxicity, although cost and ease of use have also influenced this trend. Early automated alternatives to mercury-tube sphygmomanometers were often seriously inaccurate, but validated devices have better accuracy to mercury devices, if you allow an error of equal to or less than 5 mm Hg and a standard deviation of equal to or less than 8 mm Hg.
Blood pressure is influenced by cardiac output, total peripheral resistance and arterial stiffness and varies depending on situation, emotional state, activity, and relative health/disease states. In the short term, blood pressure is regulated by baroreceptors which act via the brain to influence nervous and endocrine systems.
Blood pressure that is low is called hypotension, and pressure that is consistently high is hypertension. Both have many causes. and may be of sudden onset or of long duration. Long-term hypertension is a risk factor for many diseases, including heart disease, stroke and kidney failure. Long-term hypertension is more common than long-term hypotension, which often goes undetected because of infrequent monitoring and the absence of symptoms.
The risk of cardiovascular disease increases progressively above 115/75 mmHg. In practice blood pressure is considered too low only if noticeable symptoms are present.
Observational studies demonstrate that people who maintain arterial pressures at the low end of these pressure ranges have much better long term cardiovascular health. There is an ongoing medical debate over what is the optimal level of blood pressure to target when using drugs to lower blood pressure with hypertension, particularly in older people.
The table shows the classification of blood pressure adopted by the American Heart Association for adults who are 18 years and older. It assumes the values are a result of averaging resting blood pressure readings measured at two or more visits to the doctor.
Blood pressure fluctuates from minute to minute and normally shows a circadian rhythm over a 24-hour period, with highest readings in the early morning and evenings and lowest readings at night. Loss of the normal fall in blood pressure at night is associated with a greater future risk of cardiovascular disease and there is evidence that night-time blood pressure is a stronger predictor of cardiovascular events than day-time blood pressure. Also, an individual’s blood pressure varies with exercise, emotional reactions, sleep, digestion and time of day (circadian rhythm).
Various other factors, such as age and sex, also influence a person’s blood pressure. In children, the normal ranges are lower than for adults and depend on height. Reference blood pressure values have been developed for children in different countries, based on the distribution of blood pressure in children of these countries.As adults age, systolic pressure tends to rise and diastolic pressure tends to fall. Consequently, in the elderly, systolic blood pressure often exceeds the normal adult range, this is thought to be due to increased stiffness of the arteries.
Differences between left and right arm blood pressure measurements tend to be small. However, occasionally there is a consistent difference greater than 10 mmHg which may need further investigation, e.g. for obstructive arterial disease.
MEAN ARTERIAL PRESSURE
The mean arterial pressure (MAP) is the average over a cardiac cycle and is determined by the cardiac output (CO, systemic vascular resistance (SVR), and
central venous pressure (CVP)
MAP =(CO.SVR) +CVP
In practice the contribution of CVP (which is small) is generally ignored and so
MAP=CO.SAR
MAP can be estimated from measurements of the systolic pressure P(systolic) and the diastolic pressure P(diastolic).
so, MAP = P (diasolic) +1/3 P (P sys – p dias)
PULSE PRESSURE
P pulse = ( P systolic – P diastolic )
Curve of the arterial pressure during one cardiac cycle. The closing of the aortic valve causes the notch in the curve.
The pulse pressure is the difference between the measured systolic and diastolic pressures.
The up and down fluctuation of the arterial pressure results from the pulsatile nature of the cardiac output, i.e. the heartbeat. Pulse pressure is determined by the interaction of the stroke volume of the heart, the compliance (ability to expand) of the arterial system—largely attributable to the aorta and large elastic arteries—and the resistance to flow in the arterial tree. By expanding under pressure, the aorta absorbs some of the force of the blood surge from the heart during a heartbeat. In this way, the pulse pressure is reduced from what it would be if the aorta were not compliant. The loss of arterial compliance that occurs with aging explains the elevated pulse pressures found in elderly patients.
SYSTEMIC VENOUS PRESSURE
Blood pressure generally refers to the arterial pressure in the systemic circulation. However, measurement of pressures in the venous system and the pulmonary vessels plays an important role in intensive care medicine but requires invasive measurement of pressure using a catheter.
Venous pressure is the vascular pressure in a vein or in the atria of the heart. It is much less than arterial pressure, with common values of 5 mmHg in the right atrium and 8 mmHg in the left atrium.
VARIANTS OF THE VENOUS PRESSURE INCLUDE:
Central venous pressure, which is a good approximation of right atrial pressure, which is a major determinant of right ventricular end diastolic volume. (However, there can be exceptions in some cases.)
The jugular venous pressure (JVP) is the indirectly observed pressure over the venous system. It can be useful in the differentiation of different forms of heart and lung disease.
The portal venous pressure is the blood pressure in the portal vein. It is normally 5–10 mmHg
PULMONARY PRESSURE
Normally, the pressure in the pulmonary artery is about 15 mmHg at rest. Increased blood pressure in the capillaries of the lung causes pulmonary hypertension, leading to interstitial edema if the pressure increases to above 20 mmHg, and to pulmonary edema at pressures above 25 mmHg.
DISORDERS
Disorders of blood pressure control include high blood pressure, low blood pressure, and blood pressure that shows excessive or maladaptive fluctuation.
HIGH HYPERTENSION
SYMPTOMS
Hypertension is generally a silent condition. Many people won’t experience any symptoms. It may take years or even decades for the condition to reach
levels severe enough that symptoms become obvious. Even then, these symptoms may be attributed to other issues.
SYMPTOMS OF THE SEVERE HYPERTENSION INCLUDE:
Headaches
Shortness of breath
Nosebleeds
Flushing
Dizziness
Chest pain
Visual changes
Blood in the urine
These symptoms require immediate medical attention. They don’t occur in everyone with hypertension, but waiting for a symptom of this condition to appear could be fatal.
The best way to know if you have hypertension is to get regular blood pressure readings. Most doctors’ offices take a blood pressure reading at every appointment.
MAIN COMPLICATIONS OF THE PERSISTENT HYPERTENSION
Arterial hypertension can be an indicator of other problems and may have long-term adverse effects. Sometimes it can be an acute problem, for example hypertensive emergency.Levels of arterial pressure put mechanical stress on the arterial walls. Higher pressures increase heart workload and progression of unhealthy tissue growth (atheroma) that develops within the walls of arteries. The higher the pressure, the more stress that is present and the more atheroma tend to progress and the heart muscle tends to thicken, enlarge and become weaker over time.
Persistent hypertension is one of the risk factors for strokes, heart attacks, heart failure and arterial aneurysms, and is the leading cause of chronic kidney failure. Even moderate elevation of arterial pressure leads to shortened life expectancy. At severely high pressures, mean arterial pressures 50% or more above average, a person can expect to live no more than a few years unless appropriately treated.
In the past, most attention was paid to diastolic pressure; but nowadays it is recognised that both high systolic pressure and high pulse pressure (the numerical difference between systolic and diastolic pressures) are also risk factors. In some cases, it appears that a decrease in excessive diastolic pressure can actually increase risk, due probably to the increased difference between systolic and diastolic pressures. If systolic blood pressure is elevated (>140 mmHg) with normal diastolic blood pressure (<90 mmHg), it is called “ISOLATED SYSTOLIC HYPERTENSION” and may present a health concern.
For those with heart valve regurgitation, a change in its severity may be associated with a change in diastolic pressure. In a study of people with heart valve regurgitation that compared measurements 2 weeks apart for each person, there was an increased severity of aortic and mitral regurgitation when diastolic blood pressure increased, whereas when diastolic blood pressure decreased, there was a decreased severity.
LOW HYPOTENSION
SYMPTOMS OF LOW BLOOD PRESSURE
Most doctors will only consider chronically low blood pressure as dangerous if it causes noticeable signs and symptoms, such as:
- Dizziness or lightheadedness
- Nausea
- Fainting (syncope)
- Dehydration and unusual thirst
Dehydration can sometimes cause blood pressure to drop. However, dehydration does not always cause low blood pressure. Fever, vomiting, severe diarrhea, overuse of diuretics and strenuous exercise can all lead to dehydration, a potentially serious condition in which your body loses more water than you take in. Even mild dehydration (a loss of as little as 1 percent to 2 percent of body weight) can cause weakness, dizziness and fatigue.
- Lack of concentration
- Blurred vision
- Cold, clammy, pale skin
- Rapid, shallow breathing
- Fatigue
- Depression
- Underlying causes of low blood pressure
- Low blood pressure can occur with:
PROLONGED BED REST
PREGNANCY: During the first 24 weeks of pregnancy, it’s common for blood pressure to drop.
DECREASE IN BLOOD VOLUME: A decrease in blood volume can also cause blood pressure to drop. A significant loss of blood from major trauma, dehydration or severe internal bleeding reduces blood volume, leading to a severe drop in blood pressure.
CERTAIN MEDICATIONS: A number of drugs can cause low blood pressure, including diuretics and other drugs that treat hypertension; heart medications such as beta blockers; drugs for Parkinson’s disease; tricyclic antidepressants; erectile dysfunction drugs, particularly in combination with nitroglycerine; narcotics and alcohol. Other prescription and over-the-counter drugs may cause low blood pressure when taken in combination with high blood pressure medications.
HEART PROBLEMS: Among the heart conditions that can lead to low blood pressure are an abnormally low heart rate (bradycardia), problems with heart valves, heart attack and heart failure. Your heart may not be able to circulate enough blood to meet your body’s needs.
ENDOCRINE PROBLEMS: Such problems include complications with hormone-producing glands in the body’s endocrine systems; specifically, an underactive thyroid (hypothyroidism), parathyroid disease, adrenal insufficiency (Addison’s disease), low blood sugar and, in some cases, diabetes. Severe infection (septic shock): Septic shock can occur when bacteria leave the original site of an infection (most often in the lungs, abdomen or urinary tract) and enter the bloodstream. The bacteria then produce toxins that affect blood vessels, leading to a profound and life-threatening decline in blood pressure.
ALLERGIC REACTIONS (anaphylaxis): Anaphylactic shock is a sometimes-fatal allergic reaction that can occur in people who are highly sensitive to drugs such as penicillin, to certain foods such as peanuts or to bee or wasp stings. This type of shock is characterized by breathing problems, hives, itching, a swollen throat and a sudden, dramatic fall in blood pressure.
NEURALLY MEDIATED HYPOTENSION: Unlike orthostatic hypotension, this disorder causes blood pressure to drop after standing for long periods, leading to symptoms such as dizziness, nausea and fainting. This condition primarily affects young people and occurs because of a miscommunication between the heart and the brain.
NUTRITIONAL DEFICIENCIES: A lack of the essential vitamins B-12 and folic acid can cause anemia, which in turn can lead to low blood pressure.
OTHER CAUSES OF LOW ARTERIAL BLOOD PRESSURE INCLUDES:
Sepsis
Hemorrhage – blood loss
Toxins including toxic doses of blood pressure medicine
Hormonal abnormalities, such as Addison’s disease
Eating disorders, particularly anorexia nervosa and bulimia
Shock is a complex condition that leads to critically decreased perfusion. The usual mechanisms are loss of blood volume, pooling of blood within the veins reducing adequate return to the heart and/or low effective heart pumping. Low arterial pressure, especially low pulse pressure, is a sign of shock and contributes to and reflects decreased perfusion. If there is a significant difference in the pressure from one arm to the other, that may indicate a narrowing (for example, due to aortic coarctation, aortic dissection, thrombosis or embolism) of an artery.
FLUCTUATING BLOOD PRESSURE
Normal fluctuation in blood pressure is adaptive and necessary. Fluctuations in pressure that are significantly greater than the norm are associated with greater white matter hyperintensity, a finding consistent with reduced local cerebral blood flow and a heightened risk of cerebrovascular disease. Within both high and low blood pressure groups, a greater degree of fluctuation was found to correlate with an increase in cerebrovascular disease compared to those with less variability, suggesting the consideration of the clinical management of blood pressure fluctuations, even among normotensive older adults. Older individuals and those who had received blood pressure medications were more likely to exhibit larger fluctuations in pressure
PHYSIOLOGY
SYSTOLE ON THE LEFT ANT DIASTOLE AND RIGHT
During each heartbeat, blood pressure varies between a maximum (systolic) and a minimum (diastolic) pressure. The blood pressure in circulation is principally due to the pumping action of the heart. Differences in mean blood pressure are responsible for blood flow from one location to another in the circulation. The rate of mean blood flow depends on both blood pressure and the resistance to flow presented by the blood vessels. Mean blood pressure decreases as the circulating blood moves away from the heart through arteries and capillaries due to viscous losses of energy. Mean blood pressure drops over the whole circulation, although most of the fall occurs along the small arteries and arteriole Gravity affects blood pressure via hydrostatic forces (e.g., during standing), and valves in veins, breathing, and pumping from contraction of skeletal muscles also influence blood pressure in veins.
HEMODYNAMICS
Most influences on blood pressure can be understood in terms of their effect on cardiac output and resistance (the determinants of mean arterial pressure).
SOME FACTORS ARE ;
BLOOD VOLUME: The greater the blood volume, the higher the cardiac output. There is some relationship between dietary salt intake and increased blood volume, potentially resulting in higher arterial pressure, though this varies with the individual and is highly dependent on autonomic nervous system response and the renin–angiotensin system.
CARDIAC OUTPUT: The pumping action of the heart is ultimately responsible for blood pressure. Increases or decreases in cardiac output can result in increases or decreases respectively in blood pressure.
SYSTEMIC VASCULAR RESISTANCE: The higher the resistance to blood flow, the higher the arterial pressure upstream needs to be to maintain flow. In simple terms, resistance is related to vessel radius by Hagen-Poiseuille’s equation (resistance 1/radius4, so the smaller the radius, the very much higher the resistance). Other physical factors that affect resistance include: vessel length (the longer the vessel, the higher the resistance), blood viscosity (the higher the viscosity, the higher the resistance) and the presence of arterial stenosis (a narrow stenosis increases resistance to flow, however this increase in resistance rarely if ever increases systemic blood pressure, it decreases downstream flow). Substances called vasoconstrictors can reduce the calibre of blood vessels, thereby increasing blood pressure. Vasodilators (such as nitroglycerin) increase the calibre of blood vessels, thereby decreasing arterial pressure.
In practice, each individual’s autonomic nervous system and other systems regulating blood pressure respond to and regulate all these factors so that, although the above issues are important, they rarely act in isolation and the actual arterial pressure response of a given individual can vary widely in the short and long term.
REGULATION
HOMEOSTASIS
The endogenous regulation of arterial pressure is not completely understood, but the following mechanisms of regulating arterial pressure have been well-characterized:
BARORECEPETOR REFLEX :
Baroreceptors in the high-pressure receptor zones detect changes in arterial pressure. These baroreceptors send signals ultimately to the medulla of the brain stem, specifically to the rostral ventrolateral medulla (RVLM). The medulla, by way of the autonomic nervous system, adjusts the mean arterial pressure by altering both the force and speed of the heart’s contractions, as well as the systemic vascular resistance. The most important arterial baroreceptors are located in the left and right carotid sinuses and in the aortic arch.
RENIN-ANGIOTENSION SYSTEM (RAS): This system is generally known for its long-term adjustment of arterial pressure. This system allows the kidney to compensate for loss in blood volume or drops in arterial pressure by activating an endogenous vasoconstrictor known as angiotensin II.
ALDOSTERON RELEASE:
This steroid hormone is released from the adrenal cortex in response to angiotensin II or high serum potassium levels. Aldosterone stimulates sodium retention and potassium excretion by the kidneys. Since sodium is the main ion that determines the amount of fluid in the blood vessels by osmosis, aldosterone will increase fluid retention, and indirectly, arterial pressure. Baroreceptors in low-pressure receptor zones (mainly in the venae cavae and the pulmonary veins, and in the atria) result in feedback by regulating the secretion of antidiuretic hormone (ADH/Vasopressin), renin and aldosterone.
The resultant increase in blood volume results in an increased cardiac output by the Frank–Starling law of the heart, in turn increasing arterial blood pressure.
These different mechanisms are not necessarily independent of each other, as indicated by the link between the RAS and aldosterone release. When blood pressure falls many physiological cascades commence in order to return the blood pressure to a more appropriate level.
The blood pressure fall is detected by a decrease in blood flow and thus a decrease in Glomerular filtration rate (GFR) Decrease in GFR is sensed as a decrease in Na+ levels by the macula densa.
The macula densa causes an increase in Na+ reabsorption, which causes water to follow in via osmosis and leads to an ultimate increase in plasma volume. Further, the macula densa releases adenosine which causes constriction of the afferent arterioles. At the same time, the juxtaglomerular cells sense the decrease in blood pressure and release renin. Renin converts angiotensinogen (inactive form) to angiotensin I (active form).
Angiotensin I flows in the bloodstream until it reaches the capillaries of the lungs where angiotensin converting enzyme (ACE) acts on it to convert it into angiotensin II.
Angiotensin II is a vasoconstrictor that will increase bloodflow to the heart and subsequently the preload, ultimately increasing the cardiac output.
Angiotensin II also causes an increase in the release of aldosterone from the adrenal glands.
Aldosterone further increases the Na+ and H2O reabsorption in the distal convoluted tubule of the nephron.
Currently, the RAS is targeted pharmacologically by ACE inhibitors and angiotensin II receptor antagonists, also known as angiotensin receptor blockers (ARBs). The aldosterone system is directly targeted by spironolactone, an aldosterone antagonist. The fluid retention may be targeted by diuretics; the antihypertensive effect of diuretics is due to its effect on blood volume. Generally, the baroreceptor reflex is not targeted in hypertension because if blocked, individuals may suffer from orthostatic hypotension and fainting.
MEASUREMENT
Taking blood pressure with a sphygmomanometer
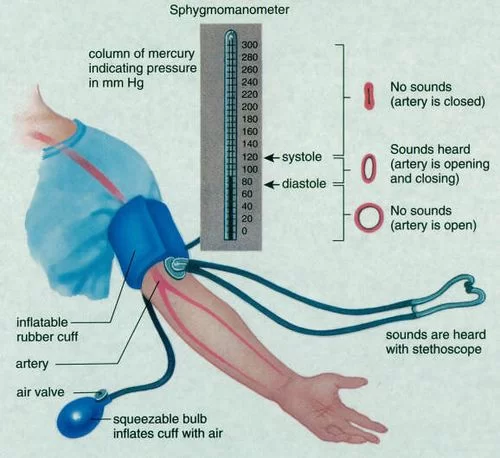
Arterial pressure is most commonly measured via a sphygmomanometer,and a stethoscope, which uses the height of a column of mercury, or an aneroid gauge, to reflect the blood pressure by auscultation. The most common automated blood pressure measurement technique is based on the so-called “oscillometric” method. Blood pressure values are generally reported in millimetres of mercury (mmHg), though aneroid and electronic devices do not contain mercury.
For each heartbeat, blood pressure varies between systolic and diastolic pressures. Systolic pressure is peak pressure in the arteries, which occurs near the end of the cardiac cycle when the ventricles are contracting. Diastolic pressure is minimum pressure in the arteries, which occurs near the beginning of the cardiac cycle when the ventricles are filled with blood. An example of normal measured values for a resting, healthy adult human is 120 mmHg systolic and 80 mmHg diastolic (written as 120/80 mmHg, and spoken as “one-twenty over eighty”).
Systolic and diastolic arterial blood pressures are not static but undergo natural variations from one heartbeat to another and throughout the day (in a circadian rhythm). They also change in response to stress, nutritional factors, drugs, disease, exercise, and momentarily from standing up. Sometimes the variations are large. Hypertension refers to arterial pressure being abnormally high, as opposed to hypotension, when it is abnormally low. Along with body temperature, respiratory rate, and pulse rate, blood pressure is one of the four main vital signs routinely monitored by medical professionals and healthcare providers.
Measuring pressure invasively, by penetrating the arterial wall to take the measurement, is much less common and usually restricted to a hospital setting.
Fetal blood pressure
Further information: Fetal circulation § Blood pressure
In pregnancy, it is the fetal heart and not the mother’s heart that builds up fetal blood pressure to drive blood through the fetal circulation. The blood pressure in the fetal aorta is approximately 30 mmHg at 20 weeks of gestation, and increases to approximately 45 mmHg at 40 weeks of gestation.
The average blood pressure for full-term infants:
Systolic 65–95 mmHg
Diastolic 30–60 mmHg
In other animals
In cats
Hypertension in cats is indicated with a systolic blood pressure greater than 150 mm Hg.
PHYSIOTHERAPY MANAGEMENT
Physical Therapy for Hypertension
A multi-faceted, holistic approach to hypertension helps patients in Red Bank to lower blood pressure without the use of medications.
Hypertension is the medical term used to describe high blood pressure. It is a common but very serious condition; one-third of American adults and two- thirds of American seniors (those over the age of 65) are affected by hypertension. The human body requires a certain level of blood pressure in order to pump blood throughout the arteries. When the arteries become narrowed, the heart must pump faster in order to carry out the necessary functions of the body.
Hypertension is typically asymptomatic and always dangerous. It increases the risk of some of the leading causes of mortality in this country, including stroke and heart disease. Because hypertension can be treated with lifestyle changes and holistic practices, it is inadvisable to rely on anti-hypertensive medications. In fact, studies show that there is no correlation between anti-hypertensive medications and longer lifespan.
Some common anti-hypertensive medications include diuretics, beta blockers, and calcium channel blockers. Diuretics deprive the body of potassium and can increase blood glucose levels. Beta blockers decrease the body’s response to impulses from the nervous system, which can lead to insomnia, depression, and cold extremities. Beta blockers may also affect blood glucose levels. Calcium channel blockers can cause heart palpitations, swollen ankles, and headaches.
For patients with hypertension, treating the underlying cause of hypertension (rather than masking the problem with drugs) is often the best option. This can be accomplished with changes in diet and lifestyle (quitting smoking, for example), as well as with healthy, drug-free techniques such as chiropractic care and physical therapy.
Physical Therapy for Hypertension
There are a number of physical therapy techniques that can help to lower blood pressure in conjunction with healthy, positive lifestyle changes. Many hypertension patients struggle with weight-related issues or injuries such as neck pain or back pain. Physical therapy can help patients with a wide range of medical conditions to begin an exercise regimen that is safe and effective. Stress relief is another major factor in reducing hypertension. For hypertensive patients who are suffering from anxiety, massage can be a powerful weapon in lowering blood pressure readings. One reason massage is so helpful is that is works to reduce steroid hormones, a good indicator of stress levels.
Go for a walk every day. Start with short distances and build up gradually. Try to walk at a pace that makes you mildly out of breath.
Walking with a friend can make it more enjoyable and help you to keep up the routine
Get advice from your physiotherapist or GP before you start doing more energetic and structured exercise
Stop smoking – see your GP if you need help with this
Lose weight if you need to
Eat a balanced diet with plenty of fresh fruit and vegetables and oily fish
Reduce the amount of alcohol, salt and animal fat in your diet
Take your medication as prescribed.
Reduce the amount of alcohol, salt and animal fat in your diet
Take your medication as prescribed.
- Do heart-pumping exercises
There are many types of exercises, but aerobic (cardio) activities are best at lowering blood pressure. Aerobic exercises include basketball, tennis, jogging, swimming, and even household chores like mopping the floor. You have to maintain moderate intensity to achieve benefits. Do at least 150 minutes of moderate intensity exercises per week, as recommended by Health Promotion Board. Do not be alarmed if your blood pressure rises during aerobic exercises.
2. Train with weights
Another type of exercise that may help lower high blood pressure is weight training. Please note that weight training, like aerobic exercises, can cause a temporary spike in blood pressure, especially when you hold your breath or lift very heavy weights. Over the long-term, weight training lowers your blood pressure and benefits your overall health.
3. Don’t be a “weekend warrior”
If you don’t have enough time to do a 30-minute exercise session during the work week, consider breaking up your workout into 10-minute blocks. This would be better than squeezing all your physical activities into a weekend, as sudden bursts of activity could be risky to your health. It can also put you at risk of certain musculoskeletal injuries.
4. Listen to your body
If you experience any chest pain or tightness, dizziness, excessive fatigue, or severe shortness of breath, stop exercising at once and seek medical help immediately. Before starting any exercise program, you should consult your doctor too.
Author: Nitesh Patel - Physiotherapist
Physiotherapist in Samarpan Physiotherapy Clinic Ahmedabad Bapunagar Amaraiwadi Vastral Mobile Physiotherapy Clinic Dr. Nitesh Patel ( Physiotherapist ) : Mo No : 09898607803


33 Comments