
Iliopsoas Muscle Anatomy: Know Your Muscles
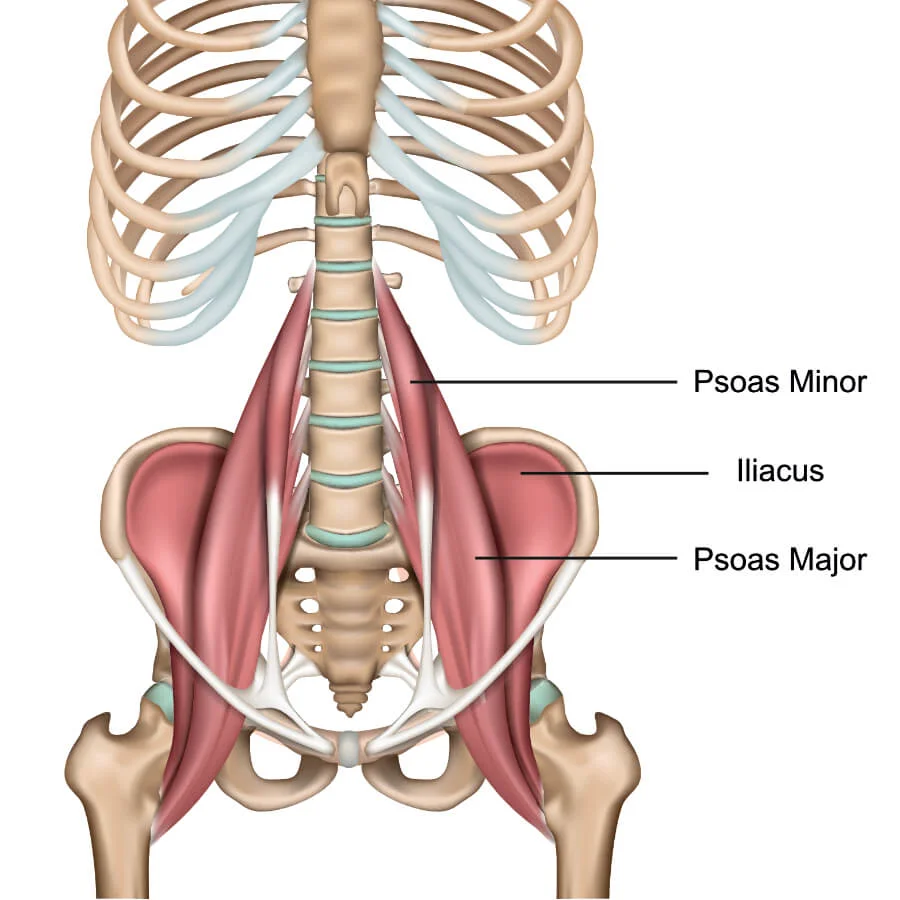
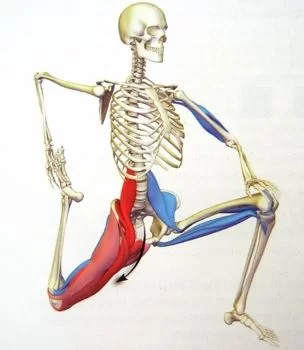
The term Iliopsoas means the combination of the psoas major muscle & the iliacus muscle Joining at their inferior ends. These muscles are distinct in the abdomen, but usually indistinguishable in the thigh.
As such, they are usually given the common name “iliopsoas” and are referred to as the “dorsal hip muscles”.The psoas minor Also contributes to the iliopsoas muscle.
Anatomy of Iliopsoas Muscle
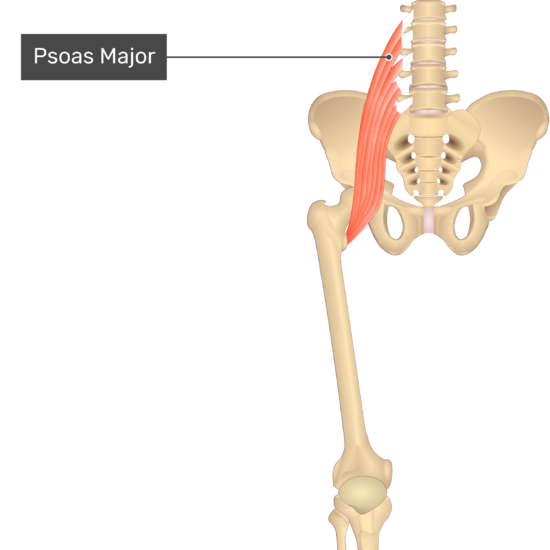
Psoas Major Muscle:
This muscle is deep into the abdominal Parts.
- Origin: Bodies and transverse processes of the lumbar vertebrae
- Insertion Site : Lesser trochanter Femur.
- Nerve Supply: Lumbar plexus
- Action : coxal joint- it flexion, laterally rotation, & adduction of The hip Joint.
Iliacus Muscle:
Deep to the abdomen in the iliac fossa
- Origin : Iliac fossa
- Insertion : Lesser trochanter Femur.
- Nerve Supply: Femoral Nerve.
- Action : coxal joint- it flexion, laterally rotation & adduction of The hip Joint.
Psoas Minor Muscle:
Roughly 40% of the population has a psoas minor. In a human, it is a relatively insignificant muscle.
- Origin: Body and transverse processes of the first lumbar vertebrae
- Insertion: Superior ramus of the pubis
- Nerve Supply: Ventral rami of the lumbar
- Action: Assist to create a lordotic curve in the lumbar spine & tilt the pelvis posteriorly
Iliopsoas Weakness:
Iliopsoas weakness may result in a “sway back” posture or “flat back” posture. As the line of gravity falls slightly posterior to the hip axis, it creates an extension movement at the hip. EMG studies show that in normal conditions the iliopsoas muscle is activated to create an internal flexion movement to counteract this external force.
Prolonged hyperextension resulting from this sway-back posture increases the stress placed on the anterior hip joint ligaments & anterior joint capsule, resulting in instability in the hip joint. This can also cause muscle imbalances due to overcompensation of surrounding muscle tissue.
Weakness in the iliopsoas causes decreased ability to flex the hip joint, as well as difficulty bringing the trunk forward when preparing to rise up from a seated position or walk up an incline. If you are a runner, it decreases your stride pattern.
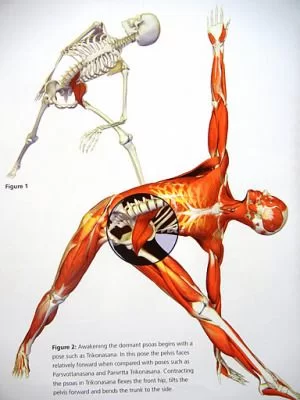
Power Triangle:

This Can Be Explained Via a Power Triangle. Many have heard of the “power triangle” in weightlifting – in this position, the hips are flexed & the trunk is forward.
With weak iliopsoas muscles, you will have difficulty getting into this position, which means you lose out on the potential power you can create in this area. So, you may not make the gains you would like in the lift. Iliopsoas weakness also causes instability at the squat portion of these lifts, which can cause discomfort to the athlete.
Strengthening the Iliopsoas Muscle:
Strengthening the iliopsoas can improve speed, agility, & strength in Olympic lifting movements. You can do any of these basic exercises before your workout or even after:
Leg Lifts:

Lie on your back, legs extended in front of you. Place your hands either underneath your bottom or above your head. If your hands are above your head, be conscious about leaving your lower back on the ground rather than curved.
The best way to do this is to think about bringing your belly button towards the spine. Lift one leg several inches above the ground. Do ten to fifteen reps on each leg. You can do these with weight As Exercise To Progress.
Hanging Leg Lifts (Knee to Elbows):
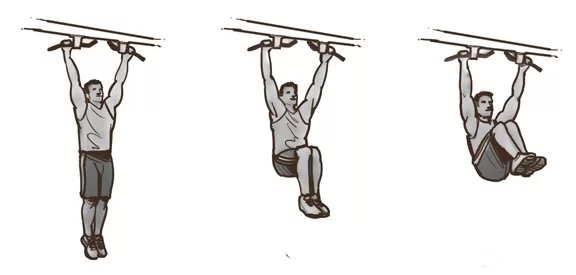
Hang from a pull-up bar. Lift both knees in towards the chest. It’s important to reach the knees to the chest area, or you can aim for your elbows like the knee-to-elbow movement.
V-Sit:

Start lying down. Lift the lower legs, knees bent at ninety degrees. Place the hands on the shins and begin to lift the upper body. Try to release the hands forward on the sides of each leg. If the strength is there, lift both legs upwards rather than forward. Hold for ten to twelve seconds, and do 10 to 12 repetitions.
Stretching Exercise Of Iliopsoas Muscle:

Tight iliopsoas can lead to lower back discomfort & dysfunction because the muscles pull on the pelvis & affect the range of motion in the lower back and hips.
Use the following movements to help bring the Full length Of The Muscle :
Low Lunge:

We all know what a lunge position is. Remember to keep the bent knee at ninety degrees and lower the back leg towards the group. Lift the upper body. You want to shift your energy forward rather than backward. If you would like you can lift your hands up towards the ceiling & add a little backbend to this movement to increase More stretch to Illeopsoas Muscle.
Bridging:

After lying down, Bend your knees so your feet are close to your gluteus Muscle. Start to lift the pelvis by squeezing the gluteus & hamstrings. Your hands should be by your side.
Inclined Plane or Reverse Plank
Begin in a seated position. Arms are behind the body and fingers are forward towards your feet. Activate the gluteus & hamstrings and start to lift the pelvis. Keep your arms Straight. The lower legs should be bent at a ninety-degree angle at the knees. If you feel comfortable in this position, extend the knees so both legs are extended forward if you can hold this position for 10 seconds to up to one minute.

A healthy and strong Iliopsoas Muscle is important for all the movements that you do in day-to-day life. So, it’s vital you take the time to strengthen & stretch these muscles to get the most out of your workouts & to prevent injuries. If you run into serious problems such as pain in the iliopsoas (which can lead to low back pain or hip pain), then consult a physiotherapist who can help alleviate those problems and treat any resulting gait problems you may have developed, as well.
Anatomical Variations
The scientific literature describes numerous anatomical variations of the iliopsoas muscle.
The iliacus muscle and the psoas major muscle join to create the iliopsoas tendon. A recent research found that a large percentage of people will find a bilateral bifid tendon (two tendons) at the level of the femur’s lower trochanter (approximately 26%).
A very tiny proportion of cases have bilateral bifid tendons, and there are also very few cases with three tendons present. The tendon may be the source of pain and hip joint dysfunction, as will be demonstrated later.
There may be additional muscle or auxiliary bodies in the psoas major muscle, which is primarily on the left and innervated by lumbar branches.
The psoas major muscle can have several fascicles, but it is always a part of a single muscle; it can have a tendon that is connected to the quadratus lumborum muscle or that is independent of the iliacus muscle.
About 40% of people have a bilateral absence of the psoas minor muscle.
The iliacus muscle has anatomical variations. It is possible that there is a supernumerary iliacus, namely on the left side. It originates from the middle third of the iliac crest, is consistently innervated by the femoral nerve, and combines with the tendon of the iliopsoas complex at its insertion.
The iliacus minimus muscle, also referred to as the iliocapsularis, is an accessory muscle that receives its innervation from the femoral nerve. It can originate at the iliolumbar ligament, go anteriorly to the iliacus muscle, lateral to the psoas major muscle, and finally unite with the iliopsoas complex muscle fibers.
Its insertion may occur in the iliofemoral ligament or in the proximal third of the femur.
There may be differences in the innervation that impact the iliopsoas complex. The lumbar plexus and femoral nerve typically pass behind the psoas major muscle. Sometimes the lumbar plexus penetrates the psoas major muscle, causing the typical clinical indications of nerve entrapment.
The femoral nerve may pass via the iliacus muscle. A psoas major auxiliary muscle may cross the femoral nerve, separating its course and allowing the nerve to pass normally under the inguinal ligament.
Clinical Importance
A disease of the internal organs can mimic symptoms of the iliopsoas muscle, which is located close to several viscera. When there is a right muscle lesion, the lower right quadrant experiences pain that resembles appendicitis. The colon’s fecal material may not move through properly if there is muscle hypertrophy.
This could be the cause of compression of the genitofemoral nerve at the level of the vessel’s lacuna gap (lacuna vasculorum), below the inguinal ligament, as well as the femoral nerve and the lateral cutaneous nerve.
The complicated iliopsoas make it challenging to detect a single issue, however, the following will provide some evaluation techniques for identifying repeated dysfunctions.
Iliopsoas Hematoma
Hematomas in the iliopsoas muscle can occur either spontaneously or as a direct consequence of trauma. The latter may result from mistakes made in blood coagulation control (prior cardiac valve operations), hemophilia, or liver disease (cirrhosis).
Other potential reasons include little, underappreciated injuries, improper muscle fiber repair following physical activity, and broken small blood vessels. One of the signs is an unexpected backache that isn’t caused by effort or pain in the flank (the side of the affected muscle).
Grey Turner sign, a visible ecchymosis on the flank due to a big retroperitoneal hematoma, compression of the femoral nerve with involvement of the thigh, and leg muscle hypoesthesia can all happen.
The patient lies down with their leg in a flexion position to reduce pain. Surgery is only required if the bleeding causes life-threatening consequences for the patient, such as hypovolemia, abdominal compartment syndrome, or femoral nerve pain.
Iliopsoas Snapping Syndrome
A malfunction of the iliopsoas complex known as iliopsoas snapping (IS) or coxa saltans produces audible and palpable noise during active hip motions, either with or without pain. IS comes in three kinds: intra-articular, internal, and external.
The external type is caused by the iliotibial band, whereas the noise and pain are caused by the gluteal maximus muscle tendon, which involves tendons moving over the great trochanter. The internal variety is characterized by exostoses of the small trochanter or movement of the iliopsoas complex tendon over the anterior capsule of the femoral head, involving the iliopectineal eminence (muscle pulley).
Moving internal bodies, labral tears, synovial chondromatosis, and the existence of chronic subluxation (in dancers or children) are the causes of the intra-articular type.
Soft tissue anomalies, the existence of an auxiliary strip of the psoas major muscle, a paralabral cyst, tendon inflammation, or bursitis are other dysfunctions that may contribute to this phenomena (IS). The iliacus muscle/tendon’s action against the pubic branch is another factor.
Following a precise medical history (about 50% of IS cases result from hip trauma) and a general palpatory examination to identify any abnormalities, the active iliopsoas snapping test is carried out.
The healthcare professional places his palm on the inguinal region while the patient is supine in the Fabere test position. The lower limb is brought back to neutral (abduction, external rotation, extension, and rest) by the patient.
When palpating, you should typically feel or hear a characteristic noise (though this may not occur) and experience pain, especially when flexion is between 30 and 45 degrees.
You can utilize the cycling test as a differential diagnostic to determine if the noise or irregular sliding action on the great trochanter is caused by an IS of the external kind. The patient is actively extending the leg on the non-supporting side while flexing it in lateral decubitus.
The FADIR test, in which the patient is recumbent and actively performs leg flexion, internal rotation, and adduction, is used to assess an intra-articular typology. This is used to recognize an intra-articular lesion, like a lesion in the labrum. Diagnostic tests with instruments can validate the diagnosis.
A radiographic evaluation is done to check for changes in the bone structure, an MRI is used to evaluate intra-articular lesions, and an analysis using ultrasound and hip mobility is done to determine the degree of inflammation. Treatment is conservative.
FAQs
What is the iliopsoas muscle?
The primary flexor of the hip joint is the iliopsoas muscle. The hip is flexed by the psoas major and iliacus working together, but because of its proximal attachments, the psoas major can also move the lumbar spinal column.
What is the iliopsoas muscle used for?
The iliopsoas muscle is used for hip flexion, which is the action of lifting your thigh toward your torso. It also plays a role in stabilizing the spine and pelvis during various movements.
Where is the iliopsoas muscle located?
The iliopsoas muscle is located in the front of the hip and consists of two muscles: the psoas major and the iliacus. The psoas major originates from the lumbar vertebrae of the spine, and the iliacus originates from the iliac crest of the pelvis. These muscles converge and attach to the femur (thigh bone), making them collectively known as the iliopsoas muscle.
What is the iliopsoas muscle problem?
In general, it has been found that tendinopathy, bursitis, snapping, and impingement of the iliopsoas, which cause persistent groin discomfort in 12–36% of athletes and 25–30% of athletes with acute groin injuries.
Is walking good for iliopsoas?
Since walking involves both hip flexion and trunk rotation, it is a more natural kind of exercise to strengthen the psoas. Jogging is preferable. Try trail running or chasing a dog around on the grass if you’re already in excellent shape.
Author: Nitesh Patel - Physiotherapist
Physiotherapist in Samarpan Physiotherapy Clinic Ahmedabad Bapunagar Amaraiwadi Vastral Mobile Physiotherapy Clinic Dr. Nitesh Patel ( Physiotherapist ) : Mo No : 09898607803




very Good Detail, We Follow Your Exercise