
Sub Acromial Bursitis: Physiotherapy Treatment
What is a Subacromial bursitis?
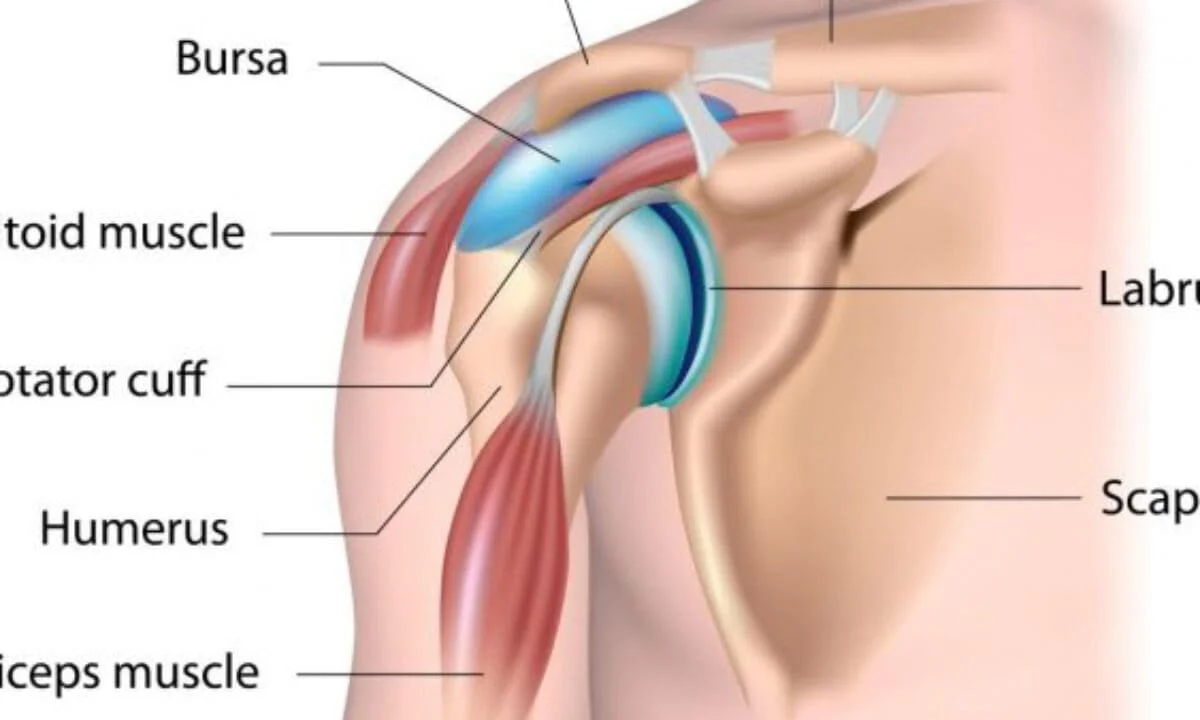
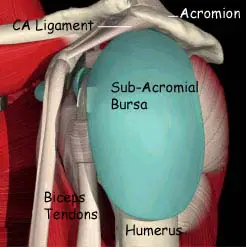
Subacromial bursitis is a condition caused by inflammation of the bursa that separates the superior surface of the supraspinatus tendon (one of the four tendons of the rotator cuff muscle) from the overlying coracoacromial ligament, acromion, and coracoid (the acromial arch) and from the deep surface of the deltoid muscle.
The subacromial bursa helps the motion of the supraspinatus tendon of the rotator cuff in activities such as overhead abduction work of the shoulder joint.
Subacromial bursitis has similar symptoms to Supraspinatus tendinitis with shoulder pain over a 60-degree arc when the arm is lifted sideways.
Anatomy Of Subacromial Bursa:
The Supraspinatus muscle runs along the top of the shoulder blade and inserts via the tendon at the top of the arm or humerus bone. This muscle is used to lift the arm up sideways and is also important in throwing sports as it is the muscle that holds the arm in the shoulder when you release what you are throwing.
There are massive forces involved in slowing the arm down after you have thrown something but few people bother to train these muscles preferring to concentrate more on the muscles that accelerate the arm rather than decelerate it.. A heavy fall onto the shoulder can also result in injuring the supraspinatus muscle.
Over the tendon is a bursa or small sack of fluid the purpose of which is to help lubricate the moving tendon. This bursa can become trapped in the shoulder causing pain and inflammation. The athlete is more prone to this injury if they overuse the shoulder, particularly in sports where the arm is at or above shoulder level. Or if the athlete has previously had a rupture of the supraspinatus tendon.
Causes of Sub Acromial Bursitis
Bursitis can result from any procedure that inflames the subacromial bursa. Typical causes include:
- Subacromial impingement
- Overuse or repetitive overhead tasks
- Direct injury
- Deposition of crystals
- Subacromial hemorrhage
- Infection
- Autoimmune conditions, such as rheumatoid arthritis
Which Symptoms are seen in Subacromial bursitis?
Symptoms of subacromial bursitis can be similar to those of supraspinatus inflammation or injury in the shoulder.
There will be pain and weakness in the arm, particularly when it is lifted sideways through a 60-degree arc.
Pain may also be felt when you press in at the inside front of the upper arm.
If it is the tendon that is injured rather than the bursa there is likely to be more pain when the arm is lifted up sideways against resistance.
Related Other symptoms:
Gradual onset shoulder pain with overhead movement
Epidemiology
About 0.4% of primary care visits are related to bursitis. There is an equal gender balance. People who engage in repetitive overhead tasks, such as athletes, manufacturing workers, and manual laborers, are more likely to experience it. Due to years of wear and tear that promote subacromial impingement, older people are more susceptible to developing subacromial bursitis.
Pathophysiology
The subacromial bursa may become inflamed due to several causes, resulting in an increase in fluid and collagen production by the bursa’s synovial cells. The fluid might become hemorrhagic and is frequently rich in fibrin. There are three stages of bursitis: acute, chronic, and recurring.
Thickened synovial fluid and localized inflammation are indicative of the acute phase. Because of the bursa’s friction between the acromion/deltoid superiorly and the humeral head/supraspinatus inferiorly, this disease causes discomfort during overhead exercises.
Because of a persistent inflammatory process inside the bursa, chronic bursitis causes persistent pain. It can also cause weakening and eventually rupture of the surrounding ligaments and tendons. Tendinitis should be taken into consideration in situations of chronic bursitis since both conditions might coexist.
Patients who have undergone repetitive trauma or normal overhead tasks may get recurrent bursitis. Patients with inflammatory diseases like rheumatoid arthritis may also show it.
Differential Diagnosis
- Impingement syndrome
- Rotator cuff tendinitis/tear
- Biceps tendinitis
- Frozen Shoulder
- Acromioclavicular joint osteoarthritis
How Diagnosis is done in Subacromial bursitis?
Bursitis can often be diagnosed by physical examination of the patient. By (visual) inspection it is possible to notice some redness and warmth, local tenderness, or stiffness in the joint with some swelling when the inflammation is worse.
By x-ray, it is possible to confirm the presence of gout crystals and calcification (which means that the bursitis is chronic or recurrent).
With bursa fluid puncture is it possible to rule out infections?
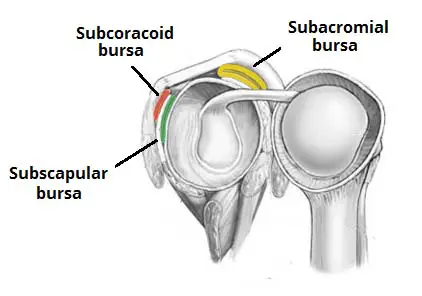
The subacromial deltoid bursa comes into conflict with the acromion. By executing the painful arc, the pain will be felt between 70 and 120 degrees of abduction. When the test is positive, we speak of a bursitis subacromiodeltoid. The movement restriction is not in accordance with the capsular pattern. This means that the abduction is more restricted than the exorotation.
The subcoracoid bursa stands in relation to the anterior joint capsule. We speak of a subcoracoid bursa when the passive exorotation in 90 degrees of abduction is negative and the passive exorotation in 0 degrees is positive.
A test for the scapulothoracic bursa focuses on the strength of the scapular muscles—including the trapezius (upper, middle, and lower), levator scapula, serratus anterior, latissimus dorsi, deltoids, and rotator cuff muscles. A loss of muscle tone or an alteration of scapulothoracic rhythm may lead to increased friction between the medial border of the scapula and the rib cage, resulting in crepitus or snapping.
A snapping scapula is a painful crepitus of the scapulothoracic articulation. This crepitus is a grinding or snapping noise with scapulothoracic motion that may or may not accompany the pain. This condition is commonly seen in overhead-throwing athletes. Treatment of patients with this syndrome begins with nonoperative methods; when nonoperative treatment fails, several surgical options exist.
Previous to bursitis, there’s always any other pathology that causes bursitis.
It is not rare that people suffering from bursitis also have other pathologies. Shoulder bursitis commonly co-exists with different shoulder pathologies (see differential diagnosis), which can make it hard to diagnose. Torn tendons or ligaments can cause as well the irritated bursa.
Shoulder bursitis can be caused due to repeated minor trauma. This can be an overuse of the shoulder joint and muscles according to a more single significant trauma such as a fall for example.
The subacromial bursa lies between the coracoacromial ligament and the supraspinatus muscle. His function is to reduce friction in the space under the acromion. Tests which can include subacromial bursitis are given at the outcome measures.
Bursitis is typically determined by pain or swelling which is localized, tenderness, and pain with motion of the affected area tissues. Procedures can include bursitis or X-ray testing and MRI scanning.
Bursitis is typically identified by localized pain or swelling, tenderness, and pain with the motion of the tissues in the affected area.
X-ray testing can sometimes detect calcifications in the bursa when bursitis has been chronic or recurrent. While MRI scanning can be used to identify bursitis, it is not always necessary.
Test for Subacromial bursitis:
Hawkins Test:
The examinator has to hold the arm in 90° anteflexion. Next, he has to do passive endoration of the arm by use of his other arm. During this manoeuvre the tuberculum majus appears under the coracoacromial ligament which causes pain within subacromial bursitis.
The same test is conducted for bankart lesion, which causes pain in the region of the m. deltoid.
The patient stands up, arm alongside the body.
Test: active abduction from 0° to 180°
The test is positive when the patient complains of pain between 60°-120° abduction.
The arm is lifted above 120° and the pressure on the bursa decreases.
Background: the subacromial space, becomes smaller during abduction and causes compression of the supraspinatus tendon and the subacromial bursa.
Medical Management in Subacromial bursitis:
A common treatment for bursitis is the use of injections with or without the use of ultrasound guidance or palpation. These injections could contain steroids or other analgesic substances.
One study examined the use and effectiveness of botulinum toxin type B in the treatment of subacromial bursitis or shoulder impingement syndrome. The conclusion was that botulinum type B can be a useful strategy and that it has great potential for replacing steroids as a treatment for subacromial bursitis or shoulder impingement syndrome.
Inflammation can also be treated with anti-inflammatory medications such as Motrin, Advil, Aleve, Celebrex, or one of many others. These all fall within the category of ‘non-steroidal anti-inflammatory medications.’ Taken by mouth, these medications help with the inflammation of the tendons and bursa and also help reduce discomfort.
Since the appearance of bursitis is due to another medical condition, treating the cause of this bursitis should be the first step. However since the bursa is still painful, injection is often used to cure this pain. This injection can be in the bursa, or in the muscle itself. A recent study has shown that both methods reduce pain, but there’s no significant difference between the two methods.
Physiotherapy Treatment in Subacromial bursitis
- Stretching regularly to increase mobility and range of motion.
- Strength training regularly to condition the surrounding muscle of the shoulder joint.
- Avoid prolonged repetitive movements, especially ones where you are lifting up over your head.
- Avoiding any other movements that you know irritate the area.
The aim of the therapy:
1) Reduce the pain and related symptoms
2) Minimize damage
3) Maintain rotator cuff motion and strength
The first step in treating bursitis is applying cold to the bursa. It will help decrease the swelling and redness around the bursa.
Apply ice every day for 12-20 minutes.
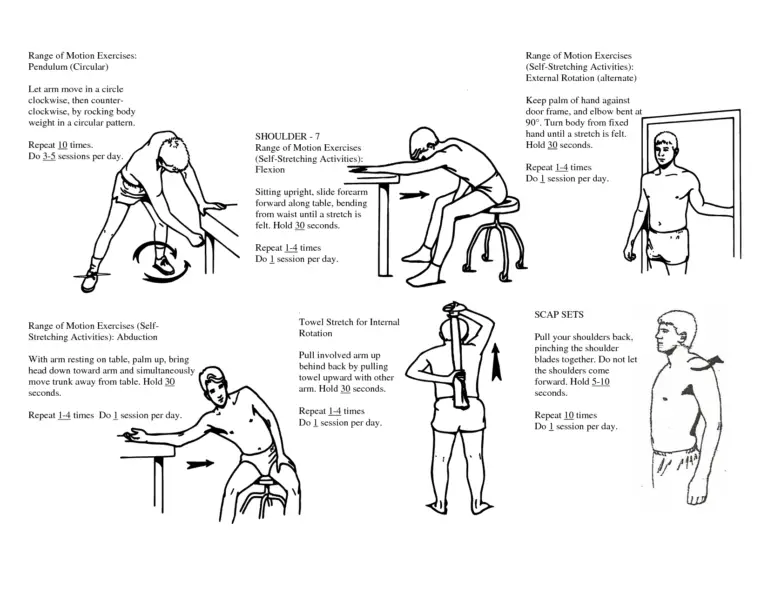
In the acute stage, also use Codman’s pendulum exercises and ROM exercises.
Once the inflammation has been reduced, you can begin using ultrasound therapy to continue the healing process.
For the best of the recovery, it is designated to keep the joint in motion. This will prevent the joint becomes stiff and the recovery process is slowed down.
Rehabilitation program
The following guidelines are for information purposes only. We recommend seeking professional advice before attempting any rehabilitation.
Aims of rehabilitation
The aims of subacromial bursitis rehab are to reduce pain and inflammation, improve or maintain mobility, strengthen the shoulder with exercises, and finally gradually return the athlete to full function and fitness.
Before beginning a subacromial bursitis rehabilitation program it is important to be aware that the athletes chance of the injury recurring are increased by any of the following:
If they have an unstable shoulder joint where there is a lot of movement and weakness in the joint for example from a previous injury or a shoulder dislocation. If you are not sure, see a sports injury professional. Failure to recognize this may mean the injury is likely to recur.
Poor technique or bad training habits. Overuse or training too hard is just as likely to cause injury as poor technique. If not sure, find a good coach.
Weakness in the rotator cuff muscles. Strengthening exercises should not be neglected just because the pain has gone.
Stage 1: To reduce the pain and inflammation.
Apply cold therapy or ice to the shoulder. This will help reduce pain and inflammation. Apply ice for up to 15 minutes every hour, gradually reducing the frequency of applications as the shoulder improves.
Rest the shoulder. Do not do anything that causes pain. Every time the athlete causes pain, they may be making the injury worse. If necessary, use a sling to restrict movement then do so but only for a few days.
NSAID or anti-inflammatory medication (e.g. ibuprofen) may help in the early stages. Always check with your Doctor before taking medication if you are not sure.
Stage 2: To re-establish range of motion and strength
(usually 5 to 7 days after injury)
Range of motion is done through shoulder mobility exercises, gradually increasing the range of motion the joint will go through pain-free and specific stretching exercises to stretch all muscles around the shoulder joint.
Sports massage techniques can help to improve greatly the condition of the rotator cuff muscles, so allowing more joint flexibility and better response to strengthening exercises.
Strengthening exercises concentrate more specifically on the external rotator muscles (the ones that rotate the arm out) and the scapular stabilizers (muscles that support the shoulder blade). It is also important to strengthen the whole joint.
Strengthening exercises must be done pain-free and in conjunction with stretching exercises.
Stage 3: To return the athlete to competition or specific training
These exercises need to be specifically tailored to the athlete’s sport. For example, throwers would start throwing a tennis ball against a wall. Five sets of 20 throws gradually increase the number of sets and number of repetitions assuming no pain during, after, or the next day.
How long will it take to heal?
Obviously, every injury is different, however, the athlete is usually able to resume sports-specific training after between 1 and 3 weeks.
If the injury is neglected it can become chronic and be very difficult to treat resulting a cycle of rotator cuff injury and impingement of the shoulder joint.
Stretches & Exercises to Relieve Shoulder Bursitis Symptoms
Before performing any of these stretches or exercises, please remember:
- Always consult with your physician before engaging in any new exercise program to ensure it is safe and appropriate for your particular condition.
- Flexible tissue is more tolerant of the stresses placed on it during activities. Warm up the area before stretching or exercising by either doing 5-10 minutes of moderate aerobic activity (e.g. brisk walking) or applying a heat pad to the affected area.
- Each stretch should be held for 20 to 30 seconds.
- A gentle stretching sensation should be felt, but never pain
Shoulder Pendulum Stretch
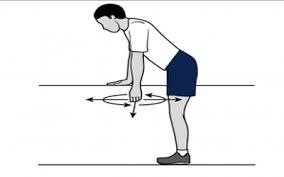
You’ll need a 3-5 lb. weight or any 3-5 lb. household object that you can comfortably grasp. Bend at the waist so your afflicted arm is dangling straight down. You may want to hold onto a table or chair with the opposite arm for support. Keeping your dangling arm loose, gently rotate your arm in a circular motion while keeping your arm and shoulder relaxed. Rotate clockwise for 2-3 minutes and then counterclockwise for 2-3 minutes and repeat until your shoulder feels loosened.
Internal Shoulder Rotation Stretch
You’ll need a rolled-up standard bath towel to perform this stretch. Hold the towel at both ends with your better hand behind your neck and the hand of the arm afflicted by bursitis behind your lower back. Pull your lower arm up the back by pulling up with your higher arm. Hold the stretch for five seconds and then return to the starting position by pulling down with your lower arm. Repeat 10 times and then make sure to switch arms (lower arm up and upper arm down).
Shoulder Flexion Stretch
You’ll need a non-weighted bar or a household item such as a broom handle to perform this stretch. Standing with good posture (core is tight, chest is up, and shoulder blades are back and down) grasp the handle shoulder width apart with your palms down. Then keeping your arms perfectly straight, raise the bar up directly over your head, hold for 5 seconds, and then slowly bring it all the way back down to the starting position and repeat 10-20 times in 3-4 sets.
Strengthening Exercises for Shoulder Bursitis
Standing Scapular Elevation
You’ll need a pair of 5-10 lbs. dumbbells or any household objects that you can comfortably grasp. Standing with good posture (core is tight, the chest is up, and shoulder blades are back and down), shrug your shoulders and traps straight up keeping your arms perfectly straight. Hold for five seconds and then slowly lower your shoulders back down to the starting position. Repeat 10-20 times in 3-4 sets.
Standing Shoulder Scaption
You’ll need a pair of 3-5 lbs. dumbbells or any household objects that you can comfortably grasp. Stand with your feet shoulder-width apart with optimal posture and hold a dumbbell in each hand with your palms facing each other in a neutral grip position. Next, bring both dumbbells up into a “Y” formation on a 45-degree angle from your body and hold for 2-3 seconds. Be sure not to raise the dumbbells above shoulder height. Slowly return back down to the starting position and repeat 10-20 times in 3-4 sets.
Upright External Shoulder Rotation
You’ll need a 3-5 lbs. dumbbell or any household object that you can comfortably grasp. Stand with the dumbbell positioned out to the side of the head, elbow bent, and shoulder height with the dumbbell directly above the elbow. Slowly lower the dumbbell forward by rotating at the shoulder until the dumbbell is in line with your shoulder. Return the dumbbell the same way back to the starting position and repeat 10-20 times in 3-4 sets for each shoulder.
Complications
Subacromial bursitis is not a shoulder pathology that is commonly linked with numerous problems. Mostly, there is always a risk that repeated steroid injections may lead to infecting the shoulder joint. Recurring injections raise the possibility of rotator cuff muscle damage.
Bhatia et al. could not discover any statistically significant variation in the frequency of rotator cuff tears between individuals who underwent three subacromial corticosteroid injections and those who underwent more than three.
Prognosis
For subacromial bursitis, the prognosis is favorable. The majority of cases get to recover with medical treatment and Physiotherapy, however, some people don’t recover even after surgery. Another factor is age, with older patients typically experiencing worse results. Generally speaking, the illness resolves on its own and has no long-term effects on the patient’s daily activities.
FAQs
What are the 3 symptoms of bursitis?
The most typical symptoms of bursitis include pain, swelling, and soreness in nearby areas of a joint. Rest and anti-inflammatory medications can be used to treat bursitis.
Will bursitis heal on its own?
Bursitis symptoms can mimic those of other health issues, so it’s important to consult a Doctor as soon as possible for a comprehensive diagnosis, guidance, and customized treatment plan. Without therapy, bursitis can take weeks to heal. It may or may not go away on its own.
How do you treat subacromial bursitis?
The treatment for subacromial bursitis typically includes rest, ice, anti-inflammatory medications, and physical therapy. Severe cases may require corticosteroid injections or, in rare instances, surgical intervention. Always consult with a healthcare professional for personalized advice.
Can shoulder bursitis be cured?
It’s quite likely that shoulder bursitis will fully heal. In most cases, the symptoms go away with Proper treatment. Shoulder bursitis often reacts favorably to rest and anti-inflammatory drugs. Longer-term physical treatment may be required if there is another shoulder issue, such as tendonitis or bone issues.
How long does subacromial bursitis take to heal?
The healing time for subacromial bursitis varies, but with proper treatment, many people experience improvement within a few weeks to a few months.
Author: Nitesh Patel - Physiotherapist
Physiotherapist in Samarpan Physiotherapy Clinic Ahmedabad Bapunagar Amaraiwadi Vastral Mobile Physiotherapy Clinic Dr. Nitesh Patel ( Physiotherapist ) : Mo No : 09898607803



7 Comments