
Upper Motor Neurone Lesion
What is an Upper Motor Neurone Lesion?
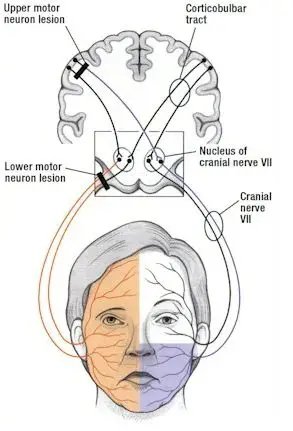
An upper motor neuron lesion is an injury or disease that occurs in the Brain to the neural pathway above the anterior horn cell of the spinal cord or motor nuclei of the cranial nerves, sign is an increase in muscle tone (spasticity), hyperreflexia, and the persistence or reappearance of primitive reflexes, such as the extensor plantar response (Babinski sign).
As compared to the opposite where lower motor neuron lesion affects nerve fibers starting from the anterior horn of the spinal cord or the cranial nerve motor nuclei to the related muscles.
Upper motor neuron lesions are mainly seen in the brain or spinal cord-related diseases such as stroke, multiple sclerosis, traumatic brain injury, cerebral palsy, atypical parkinsonism, multiple system atrophy, and amyotrophic lateral sclerosis.
UPPER MOTOR NEURON LESION DEFINITION
“An Upper motor neuron lesion (pyramidal insufficiency) is a lesion of the neural pathway above the anterior horn cell of the spinal cord or motor nuclei of the cranial nerves.”
Symptoms of upper motor neuron lesion:
The symptoms vary depending on the site and the extent of the lesion, and these are as follows:
- Muscle weakness. known as ‘pyramidal weakness’ (Partial or complete paralysis is associated with normal or increased extensor tone)
- Loss or decreased movement control mainly slowness
- Spasticity- an increase in muscle tone
- Exaggerated Tendon reflexes
- Rigidity with Clasp-knife response where initial higher resistance to movement is followed by a lesser resistance
- Babinski sign is positive means, that proper stimulation of the sole of the foot is done, and the big toe is raised (extended) rather than curled downwards (flexed). The presence of the Babinski sign is an abnormal response in adulthood. In a normal person, during the plantar reflex, it causes plantar flexion and the adduction of the toes. In Babinski’s sign, there is dorsiflexion of the big toe and abduction of the other toes. However, it is only present in infants from birth to 12 months. The positive Babinski sign after 12 months is the sign of a non-specific upper motor neuron lesion.
- Increased deep tendon reflex (DTR)
- Pronator drift
- Loss of Balance
- Loss of Co-ordination
Location of lesion and structure involved:
- Central nervous system-cortex, brainstem, corticospinal tracts, and spinal cord.
Diagnosis or pathology:
- Stroke, traumatic brain injury, spinal cord injury.
Tone:
- Increased: Hypertonia, velocity dependent.
Reflexes:
- Increased: hyperreflexia, clonus, exaggerated cutaneous and autonomic reflexes, +ve Babinski.
Involuntary movements:
- Muscle spasms: flexor or extensor.
Strength:
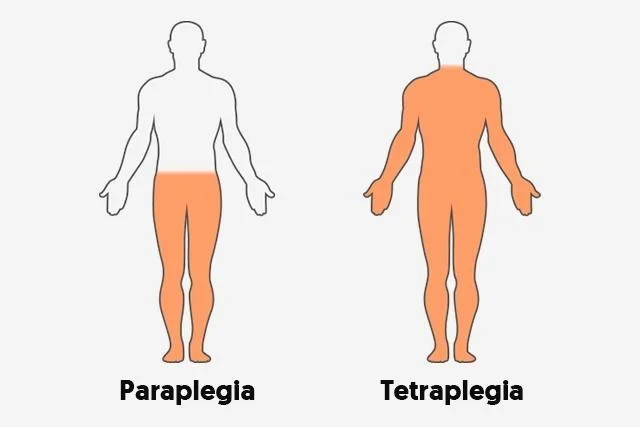
- Weakness or Paralysis: ipsilateral(stroke) or bilateral(SCI) Corticospinal: contralateral if above decussation in the medulla; ipsilateral if below distribution: never focal.
Muscle bulk:
- Disuse atrophy: variable, widespread distribution, especially of antigravity muscles.
Voluntary movements:
- Impaired or absent: dyssenergic patterns, obligatory mass synergies.
Synergies pattern in Upper motor neuron lesion:
- Primitive abd stereotyped movement associated with spasticity.
- They may be elicited reflexively, as associated reactions, or voluntary movement patterns.
- There are two basic synergies of each extremity.
(1) FLEXION SYNERGY:
(a) Upper extremity:

- Scapular elevation and retraction.
- Shoulder abduction and external rotation.
- Elbow flexion is generally the strongest component.
- Forearm supination and wrist/finger flexion.
(b) Lower extremity:

- Hip flexion is generally the strongest component of abduction and external rotation.
- Knee flexion.
- Ankle dorsiflexion and inversion.
- Toe dorsiflexion.
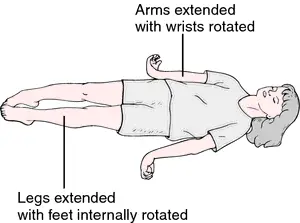
(2) EXTENSOR SYNERGY:
(a) Upper extremity:
- Scapular protraction.
- Shoulder adduction and internal rotation.
- Elbow extension.
- Forearm pronation and wrist/finger flexion.
(b) Lower extremity:
- Hip extension, adduction, and internal rotation.
- Knee extension.
- Ankle plantar flexion and inversion.
- Toe flexion.
Diagnosis
During an examination, your doctor will look for signs of a neurology problem by checking your:
- Balance and coordination
- Body Movement control
- Higher functions are your Hearing, speech, and vision
- Memory and concentration
- Muscle tone
- Babinski sign
- Knee Jerk / Ankle Jerk
Images / Tests for diagnosis
- CT Scan
- MRI
- Nerve conduction study
- Spinal tap or lumbar puncture
- Nerve biopsy
Treatment
Treatment mainly depends upon the diagnosis of the UMN Lesion diagnosis, if the stroke is diagnosed treatment is accordingly, if other diseases are diagnosed by a doctor treatment may be highly variable.
Physiotherapy Treatment :
Physiotherapy treatment also depends on an assessment of your symptoms, Diagnosis, and cause of disease.
The following are the most common goals of UMN Lesion treatment options in Physiotherapy.
- To regain movement control by repeated active/active assisted movement exercise
- Reduce spasticity/rigidity by regular stretching exercise
- Improve Balance with the help of Balancing exercise
- Improve coordination with Frankle’s coordination exercise
- Rehabilitation exercise program
- Gait training
- Functional electrical stimulation
- Neuromuscular developmental training (NDT)
Author: Nitesh Patel - Physiotherapist
Physiotherapist in Samarpan Physiotherapy Clinic Ahmedabad Bapunagar Amaraiwadi Vastral Mobile Physiotherapy Clinic Dr. Nitesh Patel ( Physiotherapist ) : Mo No : 09898607803



3 Comments