
Duchene Muscular Dystrophy (DMD)
What is a Duchenne Muscular Dystrophy (DMD)?
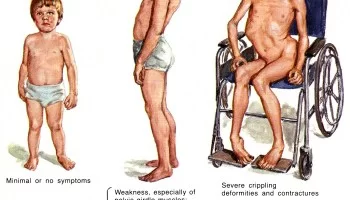
→ Duchenne muscular dystrophy (DMD) is a genetic disorder characterized by progressive muscle degeneration and weakness. This can result in trouble standing up. Most are unable to walk by the age of 12.
→ Females with a single copy of the defective gene may show mild symptoms. Scoliosis is also common.
→ The cause is a genetic change that affects the muscles. Muscles contain a chemical (protein) called dystrophin, which is necessary for muscles to function properly. People with DMD have a shortage of dystrophin in their muscles. The lack of dystrophin leads to muscle fiber damage and a gradual weakening of the muscles. The shortage of dystrophin is caused by a faulty gene.
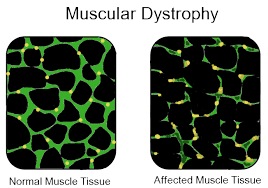
→ The body is made of cells and each cell has a ‘control center’ which contains genes. The genes are made of DNA. The genes control how the cells make proteins. Every cell contains many different genes and makes many different proteins. One of these proteins is the dystrophin protein which is involved in DMD.
→ In DMD there is a fault in the gene which makes dystrophin. So the muscle cells cannot make dystrophin (or make only a little of it). This leads to muscle damage, as explained above.
Symptoms of Duchenne Muscular Dystrophy
→ The symptoms usually start around age 1-3 years. Parents may notice – In a child, parents may notice enlarged calf muscles This enlargement is known as pseudohypertrophy, or “false enlargement,” because the muscle tissue is abnormal and may contain scar tissue.
→ A preschooler with DMD may seem clumsy and fall often. Parents also may note that children have trouble climbing stairs, getting up from the floor, or running.
→ The calf muscles may look bulky, although they are not strong.
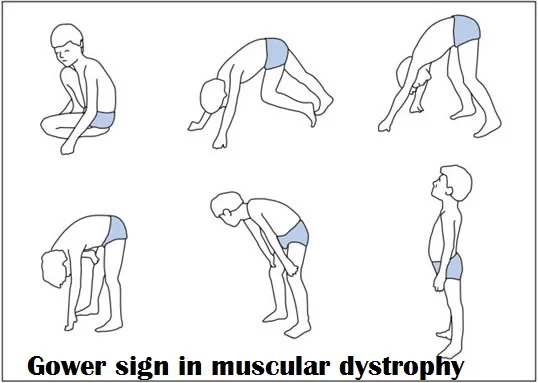
As he gets older, the child may use his hands to help him get up, looking as if he is ‘climbing up his legs’. This is called ‘Gower’s sign‘.
→ Sometimes, a delay in development may be the first sign of DMD. The child’s speech development may also be delayed. Therefore, if you have a boy whose development is delayed, you may be offered a screening test for DMD. However, DMD is only one of the possible causes of developmental delay – there are many other causes not related to DMD.
Diagnosis Procedure in Duchenne Muscular Dystrophy
→ The diagnosis may be suspected because of the child’s symptoms (above). When looking for signs of DMD, it is important to watch the child running and getting up from the floor – muscle weakness is more noticeable during these activities.
→ The first step in making the diagnosis is a blood test. This tests for creatine kinase. Children with DMD always have a very high level of creatine kinase (about 10-100 times normal). Therefore, if a child’s creatine kinase level is normal then DMD is ruled out. If the creatine kinase level is high, further tests are needed to see whether this is due to DMD or some other condition.
→ The next step in diagnosing DMD involves either a muscle biopsy and/or genetic tests:
(1) A muscle biopsy involves taking a small sample of a muscle, under local anaesthetic. The sample is examined under a microscope using special techniques to look at the muscle fibres and the dystrophin protein.
(2) Genetic tests are done using a blood sample. The DNA in the blood is tested to look at the dystrophin gene. This test can diagnose most cases of DMD.
Treatment in Duchenne Muscular Dystrophy
There is no proper cure for Duchenne muscular dystrophy (DMD) but research is ongoing. The goal of treatment is to control the symptoms of DMD and related complications caused by severe progressive muscle weakness and loss of movement may cause difficulty in day-to-day activity. Muscle Strengthening Exercises are best and try to maximize strength as much as possible.
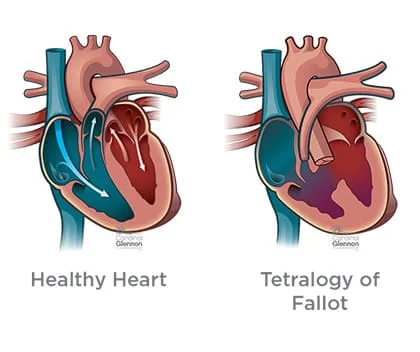
An enlarged, weakened heart (dilated cardiomyopathy) may be treated with medications, but in severe cases, a heart transplant may be necessary. Assistive devices for breathing difficulties may be needed, especially at night and as the disease progresses.
Gentle exercise is encouraged for people with DMD. Physical inactivity (such as bed rest) can worsen muscle disease, but so can overexertion. Physiotherapy may be helpful to maintain muscle strength and function.
Orthotic support (such as braces and wheelchairs) may improve the ability to move and take care of oneself.
Steroids (corticosteroids) may improve the strength and function of muscles in people with DMD, including lung function.
Few Known Steroids :
Prednisone is a steroid that has been shown to extend the ability to walk by 2 to 5 years. However, the possible side effects of prednisone include weight gain, high blood pressure, behavior changes, and delayed growth.
Deflazacort (another form of prednisone), is used in Europe and is believed to have fewer side effects and was recently approved in the United States by the FDA.
Oxandrolone, a medication used in a research study, also has similar benefits to prednisone, but with fewer side effects.
Preschool age –
→ Information about DMD. You may wish to be in touch with patient support groups or other families with DMD.
→ Referral to a specialist team so that your child’s health can be monitored. The specialist team may include a doctor who specializes in the medical care of children (a pediatrician), a specialist in muscle and nerve conditions (a neurologist), and a physiotherapist and specialist nurse.
→ Advice about the right level of exercise for your child.
→ Genetic advice for the family. You may wish to have tests to see whether anyone else in the family has the DMD gene. This may be important to families who are thinking of having more children.

Age 5-8 Years –
→ At this age, some support may be needed for the legs and ankles. For example, using night-time ankle splints, or with a longer brace called a knee-ankle-foot orthosis (KAFO).
→ Treatment with a medication called corticosteroids (or steroids) can help to maintain the child’s muscle strength.

Age 8 Years and Later –
→ At some time after the age of 8 years, the child’s leg muscles become significantly weaker. Walking gradually becomes more difficult and a wheelchair is needed. The age at which this happens varies from person to person. Often it is around age 9-11 years, although with corticosteroid treatment, some boys can walk for longer.


Author: Nitesh Patel - Physiotherapist
Physiotherapist in Samarpan Physiotherapy Clinic Ahmedabad Bapunagar Amaraiwadi Vastral Mobile Physiotherapy Clinic Dr. Nitesh Patel ( Physiotherapist ) : Mo No : 09898607803


5 Comments