

Ankle Impingement Sign (Hyperdorsi Flexion Test)
What is an Ankle Impingement Sign?
The Ankle Impingement Sign is a physical examination test used to assess for anterior ankle impingement syndrome (AAIS). AAIS is a condition in which the front of the ankle joint becomes impinged, or compressed, during dorsiflexion (bending the foot upwards).
The anterior and posterior ankle impingement tests are part of the ankle impingement test, which is used to assess ankle impingement syndrome. A variety of anterior and posterior joint pathologies involving both osseous and soft tissue anomalies are included in the syndrome known as ankle impingement. The causes, pathophysiology, diagnostic procedures, and available treatments for anterior and posterior ankle impingement syndromes are covered in this study.
Purpose
Impingement is the unnatural trapping or contact of structures that cause pain or limit movement. This examination is performed to check for anterior impingement of the ankle’s talocrural joint. Compression of tissues during dorsiflexion at the anterior border of the tibiotalar joint causes anterior ankle impingement syndrome.
Anterior impingement
In general, anterior ankle impingement refers to structures that become trapped in terminal dorsiflexion along the anterior edge of the tibiotalar joint. A number of anatomic anomalies related to the osseous and soft tissues have been identified as causal variables.
Ankle pain and limited motion in athletes have long been associated with distinctive spurs, or “exostoses,” at the anterior distal tibia and dorsal talar neck. Additional reports exist of solitary talofibular lesions. According to cadaveric dissections, the anatomy of anterior tibiotalar exostoses has been thoroughly examined. These lesions are intra-articular, lying well within the dorsal talar capsular attachment and the distal tibial attachment.
These tibial and talar spurs are sometimes called “kissing osteophytes,” but in reality, they rarely abut and overlap. According to an analysis of preoperative CT images, tibial spurs are typically seen laterally, while talar spurs typically lie medial to the talar dome’s midline. During dorsiflexion, the tibial osteophyte is frequently “accepted” by a prominent dip in the articular talar dome. Raikin et al. called this a “divot sign,” but Kim et al. called it a “tram-track lesion.” Further research has verified that patients with distal tibial lesions had a high incidence of loose bodies and concomitant talar cartilage lesions (80.7%).
Soft tissues located inside the articulation on the anterior surface may cause impingement on their own or in combination with skeletal abnormalities. There’s a triangular soft tissue mass in the anterior joint space, mostly made up of synovial and adipose tissues. In those who are asymptomatic, these tissues are squeezed after 15° of dorsiflexion. This soft tissue may have less room due to anterior osteophytes, which would worsen its entrapment and cause chronic inflammation, synovitis, and capsuloligamentous hypertrophy. Additional factors that have been identified as causal include enlarged anterior tibiofibular ligaments, synovial plica, and post-traumatic fibrous bands.
Although the impinging anatomic lesions have been thoroughly understood, the precise cause of these lesions remains unclear. According to the beginning, spurs are thought to be enthesophytes brought on by recurrent plantar flexion that causes traction on the anterior capsule. The traction theory has been refuted by anatomic studies, which show that the chondral edges and lesions are deep into the joint capsule rather than at its attachment, causing traction. Recent observations of athletic populations frequently affected with anterior impingement have given rise to theories suggesting that hyper-dorsiflexion-induced recurrent impaction injury to the anterior chondral edge or direct impact from an external object, like a soccer ball, causes disease.
It has also been suggested that abnormal repetitive micromotion resulting from chronic lateral ankle instability may play a role in the development of bone and soft tissue diseases linked to anterior impingement. Numerous research works have investigated the frequency of concurrent anterior impingement lesions during arthroscopy in patients having lateral ankle instability stabilization treatments. Soft tissue lesions, including anterior compartment synovitis or anterior lateral gutter synovitis, have been reported often (63–100%), whereas anterior tibial osteophytes have been routinely reported (12–26.4%). In one study, compared to matched asymptomatic controls, patients undergoing a Brostrom operation had a 3.37-fold higher incidence of bone spurs.
The patient performs the Anterior Ankle Impingement Test, also known as the Hyperdorsi Flexion Test, by sitting on the edge of the examination table with their legs hanging loosely and their knee bent 90 degrees. The examiner stabilizes the patient’s heel with one hand by wrapping it around it and then uses the other to pull the patient’s foot into its maximum dorsiflexion by grasping the midfoot and forefoot on the plantar side from below.
The test should be repeated using just internally and externally rotated positions of the foot.
The area around the anterior ankle joint may become painful with strong hyperdorsi flexion. The most common locations of local pain reported while palpating the anterior joint line are medial to the tibialis anterior muscle tendon or laterally to the tendons of the tibialis anterior and extensor digitorum longus muscles.
Posterior Ankle Impingement Test
Compression of the tissues posterior to the tibiotalar and talocalcaneal articulations during terminal plantar flexion causes posterior ankle impingement. Similar to that, any one or more osseous and soft tissue etiologies alone or in combination may be the cause of this.
The most frequent cause of posterior impingement is pathology related to the lateral (trigonal) process of the posterior talus. This structure’s anatomical variations have been thoroughly documented. Extended tubercles are referred to as Stieda processes. The os trigonum has been the subject of much discussion in the orthopedic and radiologic literature; nonetheless, it may indicate the failure of fusion of a secondary ossification center to the talar body. Trigonal process impingement may be the consequence of an acute fracture, a long-term injury from repeated microtrauma, or mechanical irritation of the soft tissues nearby. Less frequently, reactive hypertrophic capsule and synovium in conjunction with osteophyte impingement or tibiotalar or subtalar degenerative joint disease can cause posterior symptoms. There may also be post-traumatic consequences from fracture malunion of the talus, calcaneus, or posterior malleolus. There has also been an instance of posterior impingement brought on by talar osteonecrosis.
Various soft tissue systems may generate posterior impingement symptoms as well. Posterior capsuloligamentous damage due to repetitious or acute hyperflexion can show to inflammation, scarring, and thickening of the capsule, posterior inferior tibiofibular ligament, and posterior fibers of the deltoid ligament. Tenosynovitis and tendinosis are common conditions that affect the flexor hallucis longus (FHL) tendon, which is located between the medial and lateral posterior processes of the talus. The tendinopathy may result from overuse or secondary to disturbance from surrounding abnormal bony anatomy. Other sources of impingement have been identified as anatomic soft tissue variations, including the posterior intermalleolar ligament and various anomalous muscles.
Posterior Ankle Impingement Test or Hyperplantar Flexion Test is accomplished with the patient is sitting on the edge of the study table with the legs hanging down loosely and the knees flexed 90°. With one hand the examiner holds the patient’s heel and stabilizes it and with the other holds the mid and forefoot over the dorsum of the foot. The examiner then forces the foot into the highest plantar flexion and repeats this action many times.
Repeating the test with slightly externally and internally rotated positions is recommended.
If the patient has pain during maximal plantar flexion, particularly in the posterolateral region of the hindfoot, the posterior ankle impingement test is deemed positive. An impingement, which happens when soft tissue or a bony protuberance gets impacted between the tibia and the posterior edge of the calcaneus, is the source of the pain. It is recommended to repeat the test with different foot rotation angles.
An injection of anesthetic should be given following a positive test result and pain felt during posterolateral palpation. Under sterile conditions, the posterolateral aspect of the foot—between the posterior border of the tibia and the posterior process of the talus—is where the joint capsule is infiltrated. The test is repeated after the injection, and if the outcome is still negative (no discomfort when pressed to flex the plantar arch), the diagnosis is verified.
Ankle Impingement Sign
The examiner places the patient in a seated position, takes hold of the calcaneus with one hand, and then brings the forefoot into plantarflexion with the other. The examiner applies pressure on the ankle’s anterolateral region using his thumb. The next step involves moving the foot from plantarflexion to dorsiflexion while applying thumb pressure.
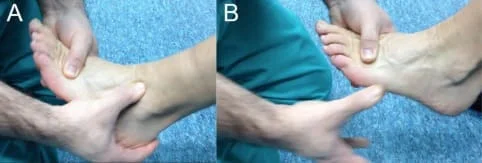
The test is positive if there is more dorsiflexion pain than plantarflexion when the examiner applies pressure.
Sensitivity/Specificity
In a study involving 73 patients who complained of ankle pain, the reference standard for determining the sensitivity and specificity of the ankle impingement sign was arthroscopic visualization.
- 95% Sensitivity
- 88% of specificity
Ankle Impingement Sign Video
FAQs
How do you diagnose anterior ankle impingement?
An impairment in the total range of motion of the ankle, primarily affecting dorsiflexion, is the typical presentation of symptoms. This may also be connected to inflammation and pain. An extensive physical examination and ankle X-rays are used to make the diagnosis.
How do you diagnose posterior ankle impingement?
The diagnosis of PAIS depends heavily on a thorough medical history and physical examination. A comprehensive neurovascular evaluation should be part of a physical examination, in addition to testing the range of motion and strength. A positive plantar flexion test result is indicated by hindfoot pain that is made worse by ankle plantar flexion.
What are the risk factors for ankle impingement?
Risk factors for Ankle impingement are:
Football players and ballet dancers are two examples of sportsmen who frequently experience pain from anterior ankle impingement. These athletes undertake recurrent dorsiflexion movements. Past occurrences of ankle sprains could be additional risk factors.
What sports often involve anterior ankle impingement?
Athletes like football players, soccer players, ballet dancers, gymnasts, and runners who experience recurrent ankle dorsiflexion frequently have anterior ankle impingement.
How much time does it take for posterior ankle impingement to heal?
Whether you choose non-surgical or surgical therapy for posterior ankle impingement, it may take up to 12 weeks to fully heal.
What are the symptoms of posterior ankle impingement?
Common symptoms include harming and swelling after an activity, as well as searing pain in the back of the ankle when engaging in activities where the foot is turned outward.
Reference
- Impingement sign ankle. (n.d.). Physiopedia. https://www.physio-pedia.com/index.php/Impingement_sign_ankle
- O. (2022, March 20). Ankle Impingement Test | OrthoFixar 2023. OrthoFixar. https://orthofixar.com/special-test/ankle-impingement-test/
- Impingement Sign. (n.d.). The Student? Physical Therapist. https://www.thestudentphysicaltherapist.com/impingement-sign.html
- image- Diniz, P., Sousa, D., Batista, J., Abdelatif, N. M. N., & Pereira, H. (2020, September 1). Diagnosis and treatment of anterior ankle impingement: state of the art. Journal of ISAKOS; Elsevier BV. https://doi.org/10.1136/jisakos-2019-000282
- Diniz, P., Sousa, D. A., Batista, J. P., Abdelatif, N., & Pereira, H. (2020).The latest methods for diagnosing and treating anterior ankle impingement. ISAKOS Journal, 5(5), 295-303. 10.1136/jisakos-2019-000282 can be found at this link.
- Lavery, K. P., McHale, K. J., Rossy, W. H., & Theodore, G. (2016). Ankle impingement. Journal of Orthopaedic Surgery and Research, 11(1). https://doi.org/10.1186/s13018-016-0430-x
