
Bronchitis
Definition of Bronchitis
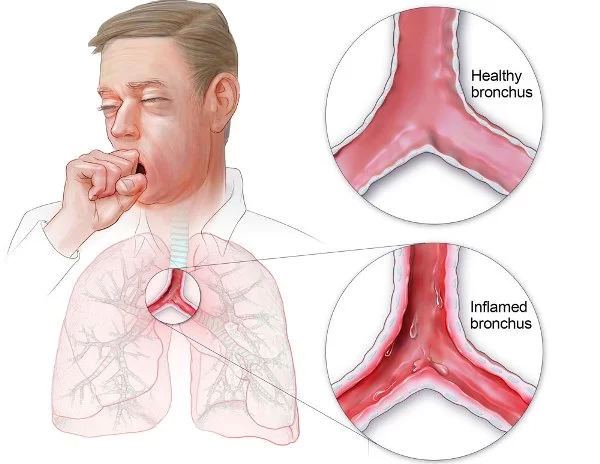
Bronchitis is inflammation of the bronchi (large and medium-sized airways) in the lungs. Symptoms include coughing up mucus, wheezing, shortness of breath, and chest discomfort. Bronchitis is divided into two types: acute and chronic. Acute bronchitis is also known as a chest cold.
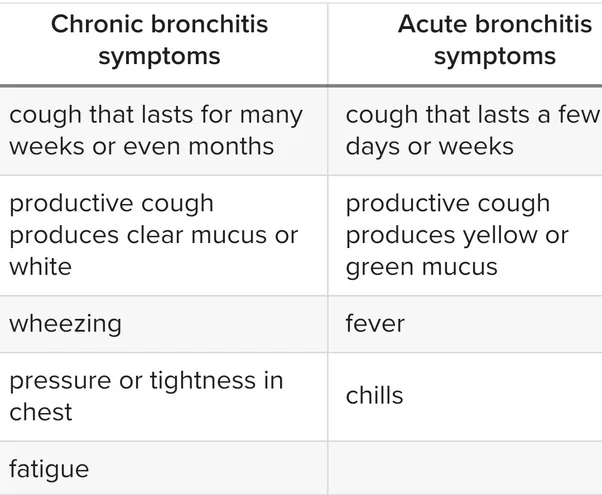
Acute bronchitis usually has a cough that lasts around three weeks. In more than 90% of cases, the cause is a viral infection. These viruses may be spread through the air when people cough or by direct contact. Risk factors include exposure to tobacco smoke, dust, and other air pollution. A small number of cases are due to high levels of air pollution or bacteria such as Mycoplasma pneumonia or Bordetella pertussis. Treatment of acute bronchitis typically involves rest, paracetamol (acetaminophen), and NSAIDs to help with the fever.
Chronic bronchitis is defined as a productive cough that lasts for three months or more per year for at least two years. Most people with chronic bronchitis have chronic obstructive pulmonary disease (COPD). Tobacco smoking is the most common cause, with a number of other factors such as air pollution and genetics playing a smaller role. Treatments include quitting smoking, vaccinations, rehabilitation, and often inhaled bronchodilators and steroids. Some people may benefit from long-term oxygen therapy or lung transplantation.
Epidemiology of Bronchitis
COPD kills around 30,000 people per year in the UK alone and it is estimated that around 3 million people in the UK have COPD, 2 million of which are undiagnosed.CB occurs in 3.4 to 22% of the US adult population and rates are even higher in patients with COPD. The prevalence of the disease has a great impact on society and on the healthcare system around the world. The primary risk factor for CB is smoking, and up to 25% of long-term smokers will go on to develop COPD. Other factors are long-term exposure to air pollution, fumes, and dust from the environment or workplace.
Causes of Bronchitis
CB is caused by overproduction and hypersecretion of mucus by goblet cells, increasing airflow obstruction. This can be due to smoke inhalation, a viral or bacterial infection, or inflammatory cell activation of mucin gene transcription
As mentioned, smoking is the primary risk factor, this can be from those who inhale second-hand smoke as well as smokers. This is caused by inflammation and permanent damage to the airways due to toxins in cigarette smoke. Other factors include fumes and dust and air pollution which can all affect your lung tissue when inhaled.
There is also a genetic factor associated with COPD, it is a deficiency in alpha-1-antitrypsin. This genetic marker is indicative of Emphysema, but many patients on the COPD spectrum have characteristics of both Emphysema and CHRONIC BRONCHITIS and should be taken into account.
Pathophysiology of Bronchitis
”MUCUS METAPLASIA”
causes airflow obstruction by several mechanisms: it causes luminal occlusion; the thickening of the epithelial layer intrudes on the airway lumen, and the mucus alters the airway surface tension. These all leave the airway at a greater risk of collapsing and decrease the capacity for airflow and gas exchange.
It was also found that smokers with moderate COPD and CHRONIC BRONCHITIS had a greater number of goblet cells in their peripheral airways, which increases the potential of mucus in the lungs. It was found that as a greater number of small airways were blocked with mucus the greater the severity of the disease.
Mucus hypersecretion is one of the risks associated with cigarette smoke exposure, viral infections, bacterial infections, or inflammatory cell activation. When combined with poor ciliary function, distal airway occlusion, ineffective cough, respiratory muscle weakness and reduced peak expiratory flow clearing secretions is extremely difficult and requires high energy consumption.
CLINICAL MANIFESTATION IN BRONCHITIS
The clinical presentation can be an increased exacerbation rate, accelerated decline in lung function, worse health-related quality of life, and increase in mortality.
Common symptoms outlined by the British Lung Foundation include:
- Wheezing, particularly breathing out
- Breathlessness when resting or active
- Tight chest
- Cough
- Producing more mucus or phlegm than usual
- These symptoms would be persistent for at least 3 months a year for 2 consecutive years to be considered Chronic Bronchitis.
Diagnosis
If a patient presents with some or all of the symptoms your doctor will follow up with more investigations such as:
- Spirometry Test: This is a breathing test to assess how well your lungs work. You breathe into a machine and two measurements are taken; forced expiratory volume (FEV1) and forced vital capacity (FVC). The readings are then compared to normal ranges for your age, to determine if your airways are compromised.
2. Chest X-ray: This will show whether there are other lung conditions that may be causing the symptoms, or in what area the obstruction is in. This can give an indication of what areas to focus on during treatment and the severity and progression of the obstruction.
3. Blood test: This is to see if your symptoms could be due to anemia, or to see if the symptoms are due to the genetic marker alpha-1-antitrypsin deficiency.
4. Phlegm sample: This is to check to see if there is an infection that is causing the symptoms, this is to primarily rule out other possibilities to ensure proper treatment.
The treatment of CB may include a variety of interventions including management through medications, education, physical exercise, and respiratory exercises. The goal of the physiotherapist should involve education, improving exercise tolerance, reducing exacerbations and hospitalization, assisting in sputum clearance, and increasing thoracic mobility and lung volume.
Medical Treatment
There are various kinds of short-term and long-term medications individuals with CHRONIC BRONCHITIS might take to reduce flare-ups, decrease obstruction, improve activity, and decrease shortness of breath. These medications may include bronchodilators, corticosteroids, and antibiotics.
Physiotherapy Treatment in BRONCHITIS
EXERCISE-
Regular exercise can have positive effects on the management, treatment, and prevention of CB and COPD. Aerobic exercise and upper & lower limb resistance training have shown positive changes in the reduction of airflow obstruction, clearing of airways, improved functional capabilities increased energy levels, and sputum expectoration. Exercise programs should be under the supervision of the treating clinical team and a discussion with the general practitioner should be had before taking part in any exercise program.
POSTURAL DRAINAGE–
The use of various positions to assist in the expectoration of sputum by using gravity to move sputum towards the throat and mouth. It can be used with other treatment techniques. These positions can be modified for each client’s condition and preferences. Ideally, the client is placed in a position where the affected area is higher than the unaffected area.
ACTIVE CYCLE OF BREATHING TECHNIQUE-
The Active Cycle of Breathing Techniques(ACBT) is one way to help you to clear sputum from your chest. ACBT is a set of breathing exercises that loosens and moves the sputum from your airways. It is best to be taught ACBT by a physiotherapist.
The ACBT exercises are breathing control, deep breathing, and huffing which are performed in a cycle until your chest feels clear.
- Breathing control exercise-
Breathing control is breathing gently, using as little effort as possible (also see leaflet GL- 02) Breathe in and out gently through your nose if you can. If you cannot, breathe through your mouth instead If you breathe out through your mouth you can use breathing control with ‘pursed lips breathing. Try to let go of any tension in your body with each breath out Gradually try to make the breaths slower Try closing your eyes to help you to focus on your breathing and to relax It is very important to do Breathing Control in between the more active exercises of ACBT as it allows your airways to relax. Breathing control can also help you when you are short of breath or feeling fearful, anxious, or in a panic.
2- Deep breathing exercise-
Take a long, slow, deep breath in, through your nose if you can. Try to keep your chest and shoulders relaxed. Breathe out gently and relaxed, like a sigh. You should do 3-5 deep breaths. Ask your physiotherapist to help you choose the right number of deep breaths for you. Some people find it helpful to hold their breath for about 2-3 seconds at the end of the breath in, before breathing out. Try the deep breathing exercises both with and without holding your breath and see which works best for you.
3. Huffing
A huff is exhaled through an open mouth and throat instead of coughing. It helps move sputum up your airways so that you can clear it in a controlled way. To ‘huff’ you squeeze air quickly from your lungs, out through your open mouth and throat, as if you were trying to mist up a mirror or your glasses. Use your tummy muscles to help you squeeze the air out, but do not force it so much that you cause wheezing or tightness in your chest. Huffing should always be followed by breathing control. There are 2 types of huff, which help to move sputum from different parts of the lungs.
The Small-long huff
This will move sputum from low down in your chest. Take a small to medium breath in and then huff (squeeze) the air out until your lungs feel quite empty, as detailed above.
The Big-short huff
This moves sputum from higher up in your chest, so use this huff when it feels ready to come out, but not before. Take a deep breath in and then huff the air out quickly. This should clear your sputum without coughing.
AUTOGENIC DRAINAGE-
Autogenic Drainage (AD), is an airway clearance technique that uses controlled breathing and minimal coughing to clear secretions from your chest. It involves hearing and feeling your secretions as you breathe out and controlling the desire to cough until secretions are high up and easily reached with minimal effort.
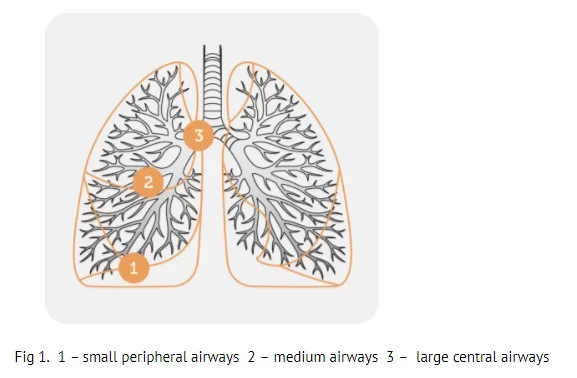
It uses breathing at different lung volumes to loosen, mobilize and move secretions in three stages toward the larger central airways. (fig.1)
Stages of AD
It consists of three stages:
Stage 1: Unstick secretions – breathe as much air out of your chest as you can then take a small breath in, using your tummy, feeling your breath at the bottom of your chest. You may hear secretions start to crackle. Resist any desire to cough.
Loosening peripheral secretions by breathing at low lung volumes (slow, deep air movement)
Repeat for at least 3 breaths.
Stage 2: Collect secretions – as the crackle of secretions starts to get louder change to medium-sized breaths. Feel the breaths more in the middle of your chest.
Repeat for at least 3 breaths.
Collecting secretions from central airways by breathing at low to middle lung volumes (slow, mid-range air movement)
Stage 3: Evacuate secretions – when the crackles are louder still, take long, slow, full breaths to your absolute maximum.
Repeat for at least 3 breaths.
Expelling secretions from the central airways by breathing at mid to high lung volumes (shallow air movements)
The velocity or force of the expiratory airflow must be adjusted at each level of inspiration so that the highest possible airflow is reached in that generation of bronchi, without being high enough to cause the airways to collapse during coughing. Autogenic drainage does not utilize Postural Drainage positions but is performed while sitting upright.
The rationale behind the Autogenic Drainage Technique
The rationale for the technique is the generation of shearing forces induced by airflow. The speed of the expiratory flow may mobilize secretions by shearing them from the bronchial walls and transporting them from the peripheral to the central airways.
TECHNIQUE OF AUTOGENIC DRAINAGE-
Posture

Clear your nose and throat by blowing your nose and huffing.
- BREATHING IN-
Slowly breathe in through the nose to keep the upper airways open. Use the diaphragm and/or the abdomen if possible.
First, take a large breath in, and hold it for a moment. Breathe all the way out for as long as you can. Now you are at low lung volume. The size of your breath and the level at which you breathe depends on where the mucus is located.
Take a small to normal breath in, and pause. Hold your breath for about 3 seconds. All the upper airways should be kept open. This improves the even filling of all lung parts. The pause allows time for the air to get behind the mucus. - BREATHING OUT-
Breathe out through the mouth. Keep the upper airways open. This is your glottis, throat, and mouth. Breathing out is done in a sighing manner. When you force your breath out the airways can collapse. You will hear a wheeze.
At low lung level breathing use your abdominal muscles. Squeeze all the air out until you can breathe out no more.
You hear the mucus rattling in the airways when breathing the right way. Put a hand on your upper chest, and feel the mucus vibrating. High frequencies mean that the mucus is in the small airways. Low frequencies mean that the mucus is in the large airways. Using this feedback lets you easily adjust the technique.
Repeat the cycle. Inhale slowly to avoid sending the mucus back down. Keep breathing at a low level until the mucus collects and moves upward.
SIGNS OF THIS ARE:
The crackling of the mucus can be heard as you exhale.
You feel the mucus moving up.
You feel a strong urge to cough.
The level of breathing is raised when any of the above occurs. Moving the breathing from the lower to the higher lung area takes the mucus with it. Finally, the collected mucus reaches the large airways where it can be cleared by a high lung volume huff. Don’t cough until the mucus is in the larger airways. Cough only if a huff did not move the mucus to the mouth.
You have now finished one cycle. Take a break of one to two minutes. Relax and perform breathing control before you start on the next cycle. The cycles are repeated during the session. A session lasts between twenty to forty-five minutes or until you feel all the mucus has been cleared. Do sessions of AD more often if you still have mucus present at the end of a session.
BENEFITS OF AD-
- No equipment is required
- Patients can perform their airway clearance independently.
- Less effort is required to expectorate which reduces stress on the pelvic floor.
- DISADVANTAGE OF AD-
- Patients generally need to be over 8 years old.
- The technique can be difficult to teach
- Patients need the cognitive ability to understand the basic physiology behind the technique
- To benefit from the auditory feedback, patients need to have a moderate or large amount of sputum
Greater expectoration was achieved with AD compared to PEP therapy.
PERCUSSION AND VIBRATION-
Usually used in conjunction with postural drainage. The theory behind the use of percussions and vibrations is that it will assist with clearing of sputum stuck in the airways. There is little evidence of this effect however, some clients do believe it helps with sputum expectoration. Percussion is the rhythmic clapping on the chest or back of the client with a loose wrist and cupped hands. The clapping should be soothing and relaxing to the client, each client may have their own personal preference. Vibrations consist of while the therapist’s hands are against the client’s chest or back performing fine movements of the hands down and inwards while the client is exhaling after a large breath.
PERCUSSION-
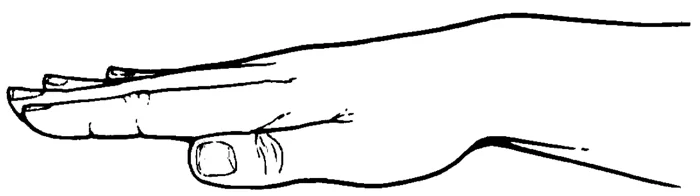
Clapping (percussion) by the caregiver on the chest wall over the part of the lung to be drained helps move the mucus into the larger airways. The hand is cupped as if to hold water but with the palm facing down (as shown in the figure below). The cupped hand curves to the chest wall and traps a cushion of air to soften the claout this type of breathing.
cupped-hand-illustration
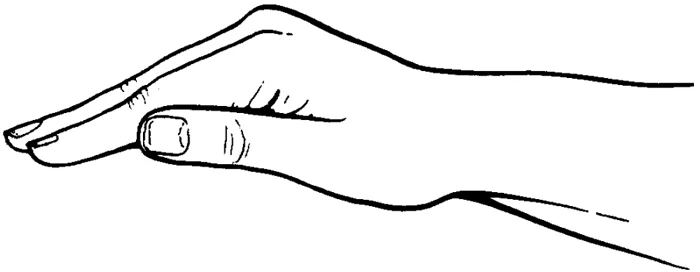
A strong beat and aggressive percussion are used. Every rhythm ought to sound hollow. Because the arm is relaxed and most of the action is in the wrist, percussion is less demanding to perform. When the hand is appropriately cupped, percussion shouldn’t hurt or sting.
Special attention must be taken to not clap over the:
- Spine.
- Breastbone.
- Stomach.
- Lower ribs or back (to prevent injury to the spleen on the left, the liver on the right, and the kidneys in the lower back).
VIBRATION-
Vibration is a technique that gently shakes the mucus so it can move into the larger airways. The caregiver places a firm hand on the chest wall over the part of the lung being drained and tenses the muscles of the arm and shoulder to create a fine shaking motion. Then, the caregiver applies a light pressure over the area being vibrated. (The caregiver may also place one hand over the other, then press the top and bottom hand into each other to vibrate.)
Vibration is done with the flattened hand, not the cupped hand (see the figure below).
Exhalation should be as slow and as complete as possible. each treatment session can last between 20 to 40 minutes. CPT is best done before meals or one-and-a-half to two hours after eating, to decrease the chance of vomiting. Early morning and bedtimes are usually recommended.
flat-hand-illustration
Deep breathing moves the loosened mucus and may lead to coughing. Breathing with the diaphragm (belly breathing or lower chest breathing) is used to help the person take deeper breaths and get the air into the lower lungs. The belly moves outward when the person breathes in and sinks in when he or she breathes out. Your CF respiratory or physical therapist can help you learn more about this type of breathing.
EDUCATION
Education of the individual with CHRONIC BRONCHITIS by the treating clinical staff in terms of the presenting condition, medication use, treatment options, and self-management may help with the psychological effects associated with having a chronic condition and promote a proactive approach to management.
How to Prevent Bronchitis?
There is presently no cure for CHRONIC BRONCHITIS. However, with lifestyle changes, education, and proper management it is possible to prevent exacerbations of the condition.
- Stopping Smoking
Smoking can irritate the lungs leading to irritation, inflammation, and scarring. The longer an individual smokes the more damage occurs to the lungs which can lead to increased amounts of exacerbations of the condition. By quitting smoking this can decrease the amount of exacerbations, hospital visits and lead to a better quality of life. - Physical Fitness
Aerobic exercise and upper & lower limb resistance training have the ability to increase physical fitness, functional tolerance, and energy levels and decrease concern over shortness of breath, exacerbations, and hospital visits. Specific guidelines are put in place in concern to exercise for individuals with chronic bronchitis and COPD. The Discussion should be held with the treating clinical team before participation in any exercise program begins. - Avoiding Irritants
Being aware of possible irritants within the household, workplace, and places of recreation can help reduce risk factors associated with chronic bronchitis and reduce exacerbations. Irritants to be aware of can include dust, chemicals, vapors, air pollution, and smoke. Proper respiratory protective equipment should be made readily available if contact with irritants in the workplace commonly occurs. - Practice Proper Hygiene
Practicing good hygiene can reduce the spread of germs, bacteria, and infections. This can help reduce the risk factors associated with bronchitis and help reduce exacerbations of chronic bronchitis. - Education
Education can play a vital aspect in the prevention and management of CHRONIC BRONCHITIS. Education about the presenting condition, risk factors associated with it, and treatment can help reduce anxiety associated with the development of any chronic condition, and a proper understanding of the condition and how to manage it can encourage the individual to take a proactive approach to their management program.
Author: Nitesh Patel - Physiotherapist
Physiotherapist in Samarpan Physiotherapy Clinic Ahmedabad Bapunagar Amaraiwadi Vastral Mobile Physiotherapy Clinic Dr. Nitesh Patel ( Physiotherapist ) : Mo No : 09898607803

My father had a problem of bronchits . And nose congestion and coughing whole day