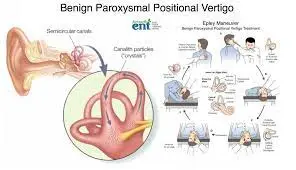
Benign Paroxysmal Positional Vertigo (BPPV) Medical Treatment
Benign paroxysmal positional vertigo is an inner-ear illness. A person with BPPV feels a sudden spinning feeling when they move their head. BPPV is not indicative of a significant condition. If it does not go away on its own after six weeks, a simple in-office surgery can help alleviate your discomfort.
Overview
What is the definition of benign paroxysmal positional vertigo (BPPV)?
Benign paroxysmal positional vertigo (BPPV) is a prevalent inner ear condition. With BPPV, changes in head position, such as tipping your head backward or sitting up in bed, cause sudden vertigo.
BPPV is not a dangerous condition, and it normally resolves on its own within a few days following the initial episode. (It may take many weeks for some folks.) However, the symptoms of BPPV can be scary and sometimes deadly, particularly in persons over the age of 65. BPPV’s unsteadiness can result in falls, which are a primary cause of fractures.
Symptoms & Causes
What is the symptoms of BPPV?
Vertigo is the primary symptom of BPPV. This vertigo experience might be minor or severe, lasting seconds or up to a minute. Other symptoms of benign paroxysmal positional vertigo may include:
- Dizziness.
- Lightheadedness.
- Balance problems.
- Nausea and vomiting.
- Blurred vision.
- Nystagmus (rapid, involuntary eye movements).
- BPPV normally affects only one ear at a time, although it has the potential to affect both.
What causes BPPV?
BPPV is nearly typically caused by a change in your head posture. Some people may have symptoms whether lying down or sitting up in bed. Others may experience sensations when they tilt their head back or to the side. These symptoms frequently intensify with age, owing to normal wear and tear on the inner ear components.
In some cases, BPPV can be a symptom of another inner ear problem, such as:
- Labyrinthitis.
- Vestibular neuritis.
- Acoustic neuroma.
- Additionally, BPPV can accompany migraines, or it can develop after a traumatic event — such as a fall, accident, or sports injury.
Diagnosis of BPPV
A doctor can confirm BPPV by analyzing a patient’s symptoms and medical history. They may do a physical examination and evaluate the ear for evidence of a separate underlying problem.
A doctor can utilize the following tests to help diagnose BPPV:
Dix-Hallpike test-
The Dix-Hallpike test involves a person lying on their back while a doctor turns their head. These movements should cause vertigo if the person has BPPV. A doctor will also check for rapid eye movements, which suggest nystagmus.
Electronystagmography (ENG)-
A doctor will use this test to record a person’s eye movements in various situations, such as staring at a light or moving the head.
Electroencephalogram (EEG) –
A clinician can use an EEG to assess brain activity and rule out any underlying neurological issues.
MRI scan-
If a doctor is unable to confirm a diagnosis, he or she may perform an MRI scan on the head and inner ears.
Treatment of BPPV
Treatments for BPPV primarily aim to improve visual stability and reduce vertigo and dizziness.
Medical Management
Unless the patient experiences severe nausea or vomiting, no medication is typically required for BPPV. If severe nausea is present, the doctor may prescribe or give anti-nausea drugs, particularly if the patient is unable to tolerate repositioning maneuvers otherwise.
Surgery:
Singular Nerve Neurectomy
A singular neurectomy is a surgical surgery that divides a single nerve. It is occasionally used to treat benign paroxysmal positional vertigo.
Posterior Canal Occlusion
- Surgery is typically reserved for instances that fail routine canalith repositioning methods. There are numerous surgical possibilities.
- Labyrinthectomy of the affected ear can effectively treat benign positional vertigo. However, it appears to be overly aggressive for the pathologies involved. Historically, the solitary nerve cut was thought to be the best treatment option.
- However, few, if any, surgeons were able to perform this treatment without injuring critical hearing structures.
- Aminoglycosides (such as Gentamicin and Streptomycin) can also be administered transtympanic.
- However, like labyrinthectomy, it may be excessive.
- Each individual has six semicircular canals (three on each side) and four linear acceleration sensors.
- Labyrinthectomy and transtympanic aminoglycoside administration eliminate three semicircular canals and two linear acceleration sensors.
- Posterior Semicircular Canal Occlusion is the least invasive surgical treatment option for benign positional vertigo because it only fixes the affected semicircular canal.
- Semicircular canal occlusion works on the principle that vertigo is induced by particle movement within one of the semicircular canals.
- Crushing the canal would isolate these particles, thereby stopping the vertigo.
- Canal occlusion is completed via a mastoidectomy method.
- The preoperative examination should positively identify the affected semicircular canal.
- The canal is then surgically defined using a fine diamond drill pushed.
- The membranes within the semicircular canal are carefully treated to prevent complete fluid leaking.
- The membranes are then sealed with muscle and autologous tissue grafts, trapping and immobilizing the particles.
Medications:
There are no drugs that directly cure BPPV.
Antivert, Meclizine, and vestibular suppressants can be used to treat dizziness, nausea, and other symptoms associated with BPPV.
- Drug therapies are not currently suggested for BPPV or bilateral vestibular paresis.
- Prophylactic medications (L-channel calcium channel antagonists, tricyclic antidepressants, and beta-blockers) are the primary treatment for migraine-related vertigo.
- Individuals with stroke or other structural abnormalities of the brainstem or cerebellum should take an varied strategy that includes vestibular suppressant trials as well as physical treatment.
- Psychogenic vertigo is associated with panic disorder, anxiety disorder, and agoraphobia. Benzodiazepines are the most effective medicines in this scenario.
- The majority of vertigo diagnoses are for undetermined or ill-defined causes. A scientific strategy to these patients is recommended, which includes trials of drugs with broad value, such as benzodiazepines, as well as trials of medication withdrawal where appropriate, physical therapy, and mental consultation.
Other treatments for BPPV
The effective therapies for BPPV include the following:
Epley maneuver-
To remove calcium carbonate crystals from the semicircular canals, conduct a specific set of head movements known as the Epley maneuver.
This treatment can be administered by a skilled healthcare expert, who will also teach patients how to perform the movements at home.
To perform the Epley maneuver:
- Start by sitting on the edge of the bed.
- Make a 45-degree turn with your head.
- Lie down on your back, head turned, and hold for 30 seconds.
- Turn the head 45 degrees to the left and hold for 30 seconds.
- Roll the body to the left side and hold for 30 seconds.
- Sit up on the left side.
- Repeat these procedures on the opposite side, first rotating your head to the left.
- Repositioning techniques are quite effective for curing BPPV. In a study with BPPV, researchers discovered that repositioning movements were 75-100% effective one month following treatment.
- A doctor may urge a patient to keep their head erect for several days after the procedure. This will prevent the crystals from returning to the semicircular canals.
Brandt-Daroff Exercises
These exercises are less successful than the Epley maneuver because they do not always clear calcium carbonate crystals from the semicircular canals. Instead, these activities disperse any buildups. However, Brandt-Daroff exercises can alleviate vertigo symptoms.
To perform Brandt-Daroff exercises:
- Start in an upright, seated position at the edge of the bed.
- Lie down on your left side, with your head turned to the right and your face pointing toward the ceiling.
- Hold this position for thirty seconds.
- Sit up and return to your starting posture.
- Repeat this practice with the right side.
- Some persons may experience dizziness or lightheadedness after completing a set of Brandt-Daroff exercises. If this is the case, they should wait until the dizziness subsides before standing.
- People should discontinue these activities if they experience new or worsening symptoms.
Semont Maneuver
- Patient sits in a brief sitting position, head rotated 45 degrees towards the unaffected ear.
- Examiner places one hand under the bottommost shoulder and the other hand supports the neck.
- The patient quickly moves into a side-lying position on the affected side.
- Hold this position for thirty seconds.
- Without moving his head, the patient should lie sideways on the other side of his body (face orientated towards the bed). Hold this position for thirty seconds.
The Lempert Maneuver
Treatment for horizontal or lateral canal BPPV
- The patient lies supine on the examination table, afflicted ear down.
- Quickly move the head 90 degrees to the unaffected side looking up.
- Wait for 15-20 seconds between each head turn.
- Turn the head 90 degrees, so the affected ear is up.
- Have the patient tuck their arms to their chest, then roll them into a prone position.
- Turn the patient on their side and roll their head 90 degrees (return to original posture, afflicted ear down).
- Reposition the patient so that they are face up and sitting.
The Gufoni Maneuver
Treatment for horizontal or lateral canal BPPV
- The patient was moved from sitting to lying on either the affected or unaffected side.
- Geotropic nystagmus remains unchanged.
- Apogeotropic: Affected
- Turn the patient’s head fast to the ground (45-60 degrees) and hold this position for 2 minutes.
- The patient returns to sitting with the head remaining in that position.
Habituation Techniques
- Avoid fast spins or movements that can cause vertigo.
- Sleep in a semi-recumbent position for the next two nights, using Epley’s approach (use a recliner or stack of pillows).
- Avoid sleeping on the affected side.
- Try to keep your head straight during the day and avoid all supine activities.
- After a week of being conservative, begin to place your head (in controlled conditions) in vertigo-provoking positions.
Vestibular Rehabilitation Exercises.
- Vestibular rehabilitation activities are frequently used in the treatment of BPPV and are intended to teach the brain to use alternative visual and proprioceptive cues to maintain balance and gait.
- These exercises have been proven to improve nystagmus, postural control, movement-induced dizziness, the ability to do daily tasks independently, and levels of discomfort.
- While no single vestibular rehabilitation exercise has been shown to reduce BPPV symptoms, a combination of therapies, such as self-administered repositioning maneuvers, gaze stabilization exercises, falls prevention training, and patient education, may help to reduce BPPV symptoms and improve quality of life.
- There is limited data to support the effectiveness of vestibular rehabilitation activities in improving BPPV symptoms.
- Scientist discovered that Epley’s maneuver, delivered by a healthcare practitioner, was a more effective therapy method than vestibular rehabilitation activities.
- Vestibular exercises were, nevertheless, rated superior to no treatment at all.
- There is no superior kind of vestibular rehabilitation exercise, and activities appear to have a stronger benefit when performed in combination rather than individually.
Cawthorne Cooksey Exercises
- Cawthorne-Cooksey exercises are designed to relax the neck and shoulder muscles, train the eyes to move independently of the head, and practice balancing and head movements that create dizziness.
- The exercises involve a sequence of increasingly demanding eye, head, and torso movements designed to elicit symptoms.
- The purpose of these exercises is to wear out the vestibular response and push the central nervous system to adapt by becoming accustomed to the stimuli.
FAQ
What is the most effective treatment for BPPV?
First-line therapeutic option for posterior canal BPPV is a repositioning motion aimed at clearing debris from the afflicted semicircular canal. The repositioning movements effectively improve posterior canal BPPV.
What is the first-line therapy for BPPV?
BPPV is treated with a canalith repositioning operation known as the Epley maneuver, which moves the canalith from the semicircular canal to the vestibule30. The success rate is around 70% on the first attempt and nearly 100% on subsequent maneuvers.
Is BPPV easily treatable?
It is easily identified following a thorough history and bedside examinations. BPPV can be successfully treated with a specific combination of physical movements that remove these crystals from the inner ear.
How do you sleep with BPPV?
Elevate your head: Sleep with your head elevated by at least 45 degrees. View Source may help reduce benign paroxysmal positional vertigo. To accomplish this angle of elevation, utilize pillows to support the upper back, neck, and head.
Why does BPPV worsen at night?
The majority of BPPV patients suffer vertigo when they change their head position in bed [11]. This is normal, and as previously noted, variations in head posture can trigger vertigo episodes. This, in turn, can impact patients’ sleep quality.
References
Professional, C. C. M. (n.d.-b). Benign Paroxysmal Positional Vertigo (BPPV). Cleveland Clinic. https://my.clevelandclinic.org/health/diseases/11858-benign-paroxysmal-positional-vertigo-bppv
Eske, J. (2023, June 26). What is benign paroxysmal positional vertigo? https://www.medicalnewstoday.com/articles/326157#diagnosis
Vestibular Disorders Association. (2023, September 22). Benign Paroxysmal Positional Vertigo (BPPV) – Vestibular Disorders Association. https://vestibular.org/article/diagnosis-treatment/types-of-vestibular-disorders/benign-paroxysmal-positional-vertigo-bppv/?gclid=Cj0KCQiAnfmsBhDfARIsAM7MKi2BSBCBTzDIFut15Q2gabt9ol2z9lMGxSb04uQan0LWi-Mm3OsHe64aAp4uEALw_wcB
ENT Health. (n.d.). Benign Paroxysmal Positional Vertigo (BPPV) – ENT Health. https://www.enthealth.org/conditions/benign-paroxysmal-positional-vertigo-bppv/
Benign Positional Paroxysmal Vertigo (BPPV). (n.d.). Physiopedia. https://www.physio-pedia.com/Benign_Positional_Paroxysmal_Vertigo_(BPPV)
Posterior semicircular canal occlusion. (n.d.). http://www.dr-li.net/canal_occlusion.html