
FRENKLE’S CO-ORDINATION EXERCISE
What is a Frenkel’s Exercise?
The Frenkel’s exercise was created by Heinrich Frenkel to help individuals with ataxia, to improve coordination and proprioception. With these exercises, the central nervous system is trained by carefully repeating activities, especially in the lower limbs, while maintaining a high level of focus. There are three ways to perform the exercises: sitting, lying down, and standing.
As the pioneer of exercise-based rehabilitation medicine, Frenkel is recognized for having introduced the concept of physical activity as a means of enhancing gait and restoring coordination. The exercise was developed for people with sensory ataxia, namely tabetic ataxia, but it has also been shown to be beneficial for other neurological diseases that compromise proprioception and coordination.
Definition of Coordination Exercises
It is the ability to execute smooth, accurate, controlled motor responses (optimal interaction of muscle function).
Coordination is the ability to select the right muscle at the right time with proper intensity to achieve proper action.
Coordinated movement is characterized by appropriate speed, distance, direction, timing, and muscular tension.
It is the process that results in the activation of motor units of multiple muscles with simultaneous inhibition of all other muscles in order to carry out a desired activity
Importance of the cerebellum in coordination :
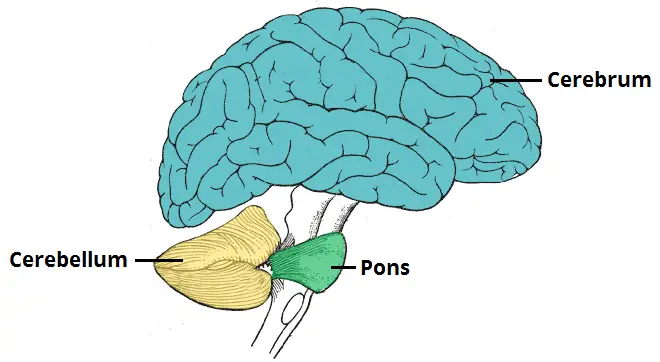
The cerebellum is the primary center in the brain for the coordination of movement.
Components of Coordinated Movement:
Volition: is the ability to initiate, maintain, or stop an activity or motion.
Perception: intact proprioception and subcortical centers to integrate motor impulses and sensory feedback. When proprioception is affected it is compensated with visual feedback.
Engramformation: is the neurological muscular activity developed in the extrapyramidal system. Research proved that high repetitions of precise performance must be performed in order to develop an engram
Types of coordination:
1) Fine motor skills:
Require coordinated movement of small muscles (hands, face).
Examples: include writing, drawing, buttoning a shirt, blowing bubbles
2) Gross motor skills:
Require coordinated movement of large muscles or groups of muscles (trunk, extremities).
Examples: include walking, running, and lifting activities.
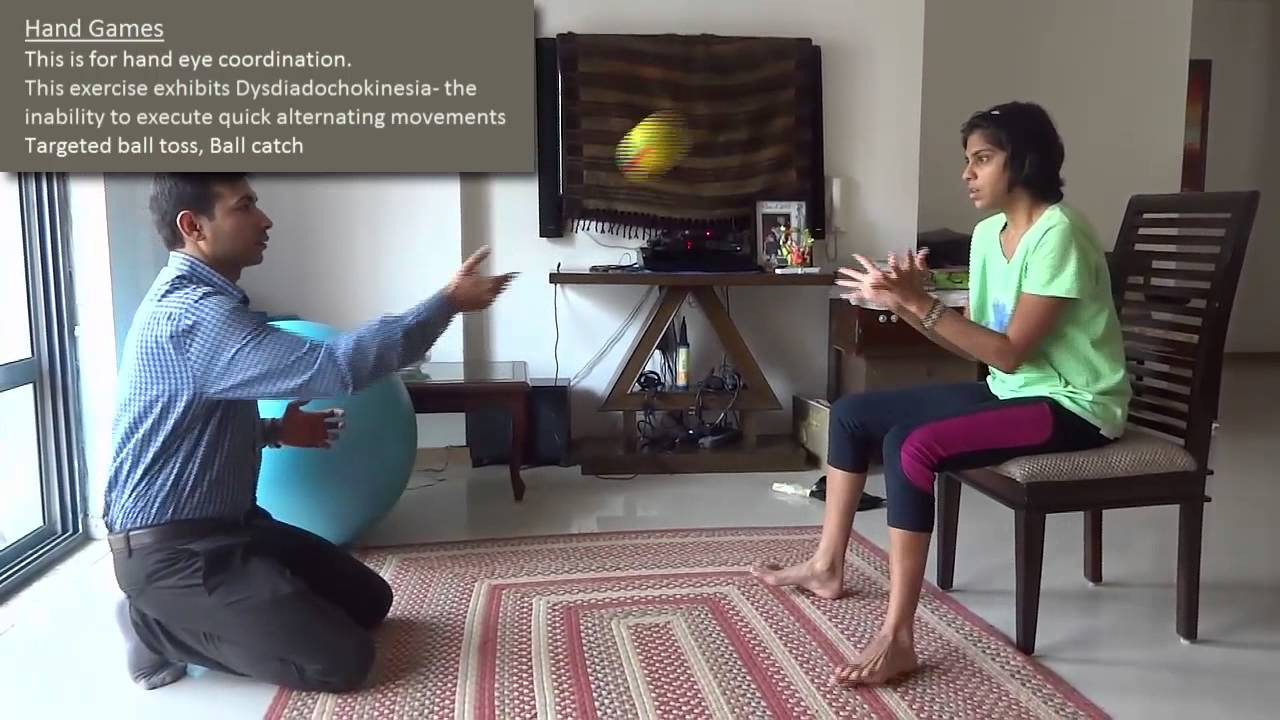
3) Hand-eye skills:
The ability of the visual system to coordinate visual information. Received and then controlled or directed the hands in the accomplishment of a task.
Examples: include catching a ball, sewing, and computer mouse use.
Causes of coordination impairments, Causes of Ataxia
Degeneration, damage, or loss of nerve cells in the cerebellum, which is the part of the brain that controls muscle coordination, causes ataxia. The cerebellum comprises two small ball-shaped folded tissues present at the base of the brain near the brainstem. Diseases that damage the spinal cord and peripheral nerves that connect the cerebellum to the muscles can also cause ataxia
.
Other causes of ataxia include:
Stroke is a condition where the blood supply to a part of the brain gets severely diminished or interrupted, which deprives the brain tissue of oxygen and other nutrients resulting in the death of brain cells.
Trauma or injury to the head, which causes damage to the brain or spinal cord, can cause sudden-onset ataxia (acute cerebellar ataxia).
Chickenpox can result in a complication in the form of Ataxia; although this is not common. Ataxia can appear during the healing stages of the infection persist for days to weeks and gradually resolve over time.
Transient ischemic attack (TIA) is caused by a temporary reduction in blood supply to a part of the brain. The majority of the TIAs last only for a few minutes. Some of the symptoms of TIA include ataxia, which is temporary.
Multiple sclerosis is a chronic, potentially debilitating medical condition, which affects the central nervous system.
Cerebral palsy consists of a group of disorders, which occurs as a result of damage to a child’s brain during its early development. It can be before, during, or shortly after birth. It affects the ability to coordinate movements of the body.
Paraneoplastic syndromes are rare, degenerative disorders, which are triggered by the response of the immune system to a tumor or neoplasm. This tumor is commonly in the lungs, ovaries, lymph nodes, or breast. Patients can experience ataxia many months or years before cancer is actually diagnosed.
Toxic reactions to some medications can also cause ataxia. Medicines, especially barbiturates and certain sedatives, like benzodiazepine, can cause ataxia as a side effect. Other things, that could cause toxic reactions, are heavy metal poisoning, alcohol and drug intoxication, and solvent poisoning.
Any type of growth on the brain, either cancerous or noncancerous, can damage the cerebellum and cause ataxia.
Deficiency of vitamin E or B-12 can also lead to ataxia.
No specific cause can be found for some adults who develop sporadic ataxia, also known as sporadic degenerative ataxia, which can be of many types, such as multiple system atrophy which is a progressive and degenerative disorder.
Examples of co-ordination tests:
1) In the upper limb:

A) Finger-to-nose test
The shoulder is abducted to 90o with the elbow extended, the patient is asked to bring the tip of the index finger to the tip of the nose. Finger to therapist finger: the patient and the therapist sit opposite to each other, the therapist’s index finger is held in front of the patient, and the patient is asked to touch the tip of the index finger to the therapist’s index finger.
B) Finger-to-finger test
Both shoulders are abducted to bring both elbows extended, the patient is asked to bring both hands toward the midline and approximate the index finger from the opposing hand
C) Finger-to-doctor’s finger test
the patient alternately touch the tip of the nose and the tip of the therapist’s finger with the index finger.
D) Adiadokokinesia or dysdiadokokinesia:
The patient was asked to do rapidly alternating movements e.g. forearm supination and pronation, hand tapping.
E) Rebound phenomena:
The patient with his elbow fixed, flexes it against resistance. When the resistance is suddenly released the patient’s forearm flies upward and may hit his face or shoulder.
F) Buttoning and unbuttoning test.
In any of the previous tests, we may find:
Intention tremors and Decomposition of movements
Dysmetria: in the form of hypermetria or hypometria
2) In the lower limb:

A) Heel-to-knee test
B) Walking along a straight line. Foot close to foot: In the case of a cerebellar lesion, there is a deviation of gait
C) Romberg test: Ask the patient to stand with heels together. Swaying or loss of balance occurs while his eyes are open or closed.
General principles of co-ordination exercises involve:
Constant repetition of a few motor activities
Use of sensory cues (tactile, visual, proprioceptive) to enhance motor performance
Increase of speed of the activity over time
Activities are broken down into components that are simple enough to be performed correctly.
Assistance is provided whenever necessary.
The patient therefore should have a short rest after two or three repetitions, to avoid fatigue.
High repetition of precise performance must be performed for the engram to form.
Whenever a new movement is trained, various inputs are given, like instruction(auditory), sensory stimulation(touch), or positions in which the patient can view the movement (visual stimulation) to enhance motor performance.
Physiotherapy exercises used to improve coordination:
Frenkel’s exercises
Proprioceptive Neuromuscular Facilitation
Neurophysiological Basis of Developmental Techniques
Sensory Integrative Therapy
FRENKEL’S EXERCISES:
Frenkel aimed at establishing voluntary control of movement by the use of any part of the sensory mechanism that remained intact, notably sight, sound, and touch, to compensate for the loss of kinaesthetic sensation.
The process of learning this alternative method of control is similar to that required to learn any new exercise,
the essentials being: Concentration of attention, Precision, and Repetition
The ultimate aim is to establish control of movement so that the patient is able and confident in his ability to carry out these activities which are essential for independence in everyday life.
They are a system of slow repetitious exercises. They increase in difficulty over the time of the program. The patient watches his hand or arm movements (for example) and corrects them as needed.
Although the technique is simple, needs virtually no exercise equipment, and can be done on one’s own, concentration and some degree of perseverance is required. Research has shown that 20,000 to 30,000 repetitions may be required to produce results. A simple calculation will show that this can be achieved by doing 60 repetitions every hour for six weeks in a 16-hour daily waking period. The repetitions will take just a few minutes every hour.
The brain as a whole learns to compensate for motor deficits in the cerebellum (or the spinal cord where applicable). If the ataxia affects say, head movements, the patient can use a mirror or combination of mirrors to watch their own head movements.
History:
Best Physiotherapy Exercises for In-Coordination–Frenkel’s Exercises:
Frenkel Exercises are a series of motions of increasing difficulty performed by ataxic patients to facilitate the restoration of coordination. Frenkel’s exercises are used to bring back the rhythmic, smooth, and coordinated movements.
Dr. H S Frenkel was a physician from Switzerland who aimed at establishing voluntary control of movement by the use of any part of the sensory mechanism that remained intact, notably sight, sound, and touch, to compensate for the loss of kinaesthetic sensation.
Frenkel Exercises were originally developed in 1889 to treat patients of tabes dorsalis and problems of sensory ataxia owing to loss of proprioception. These exercises have been applied in the treatment of individuals with ataxia, in particular cerebellar ataxia. The exercises are performed in supine, sitting, standing, and walking.
Each activity is performed slowly with the patient using vision to carefully guide correct movement. These exercises require a high degree of mental concentration and effort. For those patients with the prerequisite abilities, they may be helpful in regaining control of movement through cognitive compensation strategies. Patients with partial sensation can progress to practicing exercises with their eyes closed. The main principles of Frenkel exercises are the following:
Concentration or attention
Precision
Repetition
This program consists of a planned series of exercises designed to help the patient compensate for the inability to tell where the arms and legs are- in space without looking.
1. Exercises are designed primarily for coordination; they are not intended for strengthening.
2. Commands should be given in an event, slow voice; the exercises should be done to counting.
3. It is important that the area is well-lit and that patients are positioned so that they can watch the movement of their legs.
4. Avoid fatigue. Perform each exercise not more than four times. Rest between each exercise.
5. Exercises should be done within a normal range of motion to avoid over-stretching of muscles.
6. Start With simple exercises that should be adequately performed before progressing to more difficult patterns.
General Instructions for Frenkel exercises:
Exercises can be performed with the part supported or unsupported, unilaterally or bilaterally.
They should be practiced as smooth, timed movements, performed at a slow, even tempo by counting out loud.
Consistency of performance is stressed and a specified target can be used to determine range.
Four basic positions are used: lying, sitting, standing, and walking.
The exercises progress from postures of greatest stability (lying, sitting) to postures of greatest challenge (standing, walking).
As voluntary control improves, the exercises progress to stopping and starting on command, increasing the range, and performing the same exercises with eyes closed.
Concentration and repetition are the keys to success.
Frenkel exercises for lower limb:
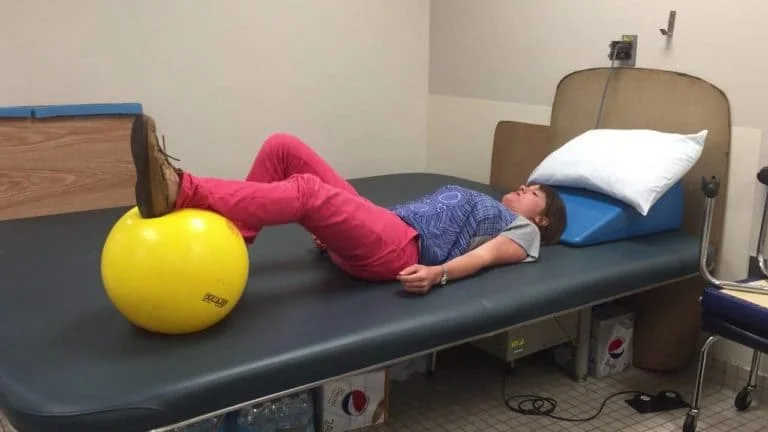
Exercises for the legs in lying
Flex and extend one leg by the heel sliding down a straight line on the table.
Abduct and adduct hip smoothly with knee bent and heel on the table.
Abduct and adduct leg with knee and hip extended by sliding the whole leg on the table.
Flex and extend hip and knee with heel off the table.
Flex and extend both legs together with the heel sliding on the table.
Flex one leg while extending the other.
Flex and extend one leg while taking the other leg into abduction and adduction.
The heel of one limb to the opposite leg (toes, ankle, shin, patella).
The heel of one limb to the opposite knee, sliding down the crest of the tibia to the ankle.
Whether the patient slides the heels or lifts it off the bed he has to touch it to the marks indicated by the patient on the plinth. The patient may also be told to place the heel of one leg on various points of the opposite leg under the guidance of the therapist.
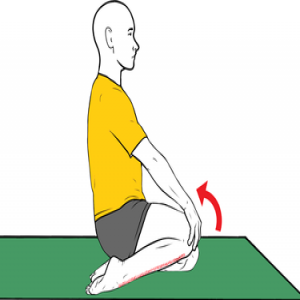
Exercises for the legs in Sitting
One leg is stretched to slide the heel to a position indicated by a mark on the floor.
The alternate leg is lifted to place the heel on the marked point.
From stride sitting posture patient is asked to stand and then sit.
Rise and sit with knees together.
Sitting hip abduction and adduction.
Exercises for the Legs in Standing
In stride standing weight is transferred from one foot to another.
Place your foot forward and backward in a straight line.
Walk along a winding strip.
Walk between two parallel lines
Walk sideways by placing your feet on the marked point.
Walk and turn around
Walk and change direction to avoid obstacles.
Frenkel exercises for upper limb:

Similar exercises can be devised for the upper limb wherein the patient may be directed to place the hand on the various points marked on the table or wallboard to improve coordination of all the movements in the upper limb.
Some examples of Frankel exercises of the upper limb in a sitting position
Have the patient sit in front of a table and place a number of objects on the table. The patient then touches each object with the right hand and then the left hand.
The patient flexes the right shoulder to 90 degrees with the elbow and wrist extended. The patient then takes his or her right index finger and touches the tip of his or her nose. This exercise is then repeated with the left hand. The exercise is performed alternating right and left index fingers.
The patient taps bilateral hands on bilateral thighs while alternating palmer and dorsal surfaces as fast as possible.
Certain diversional activities such as building with toy bricks or drawing on a blackboard, buttoning, combing, writing, and typing are some of the activities that also improve coordination.
Author: Nitesh Patel - Physiotherapist
Physiotherapist in Samarpan Physiotherapy Clinic Ahmedabad Bapunagar Amaraiwadi Vastral Mobile Physiotherapy Clinic Dr. Nitesh Patel ( Physiotherapist ) : Mo No : 09898607803


plastic sarjary