
Knee Valgus (Genu Valgum)
What is a Knee Valgus (Genu Valgum)?
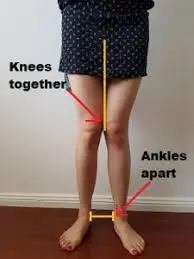
Knee valgus is valgus collapse and medial knee displacement. It is characterized by hip adduction and hip internal rotation, usually when in a hips-flexed position (the knee actually abducts and externally rotates)
Knee Valgus also known as a knock knee or Genu valgum
When standing with the feet shoulder-width apart, this misalignment causes the knees to come into contact with one another. While genu valgum is a typical growth phase in young children, it can cause a number of issues, including unequal wear on the knee joint, joint pain, and ligament stress.
Knee valgus can be caused by a number of things, such as a genetic predisposition, early-life dietary inadequacies, hormonal imbalances, and specific medical disorders such as rickets and skeletal dysplasia. Furthermore, because obesity puts additional strain on the knee joints and may increase misalignment, it can aggravate knee valgus.
Mild occurrences of knee valgus normally go away on their own as a child develops, but more severe or persistent cases may need to be treated with physical therapy, orthotic devices, or, in the worst situations, surgery. The general goals of treatment are to strengthen the muscles surrounding the knee, treat the underlying cause, and enhance joint stability and alignment. Furthermore, early management is essential to guarantee optimal musculoskeletal health and prevent long-term consequences.
What are the Causes of Knee Valgus?
Knee valgus, or genu valgum, can be caused by various factors, including:
- Physiologic and developmental; no underlying bone illness or congenital abnormality.
- Congenital: caused by a fibula deficit in length.
- Contracture of the iliotibial band.
- Injury
- Malunion of the fracture
- Greenstick fracture of the proximal tibial metaphysic stimulates growth.
- Asymmetric growth halt caused by fracture-separation of the distal femoral physis or the lateral section of the upper tibial physis.
- An imbalance in asymmetric growth is caused by infection.
- Knee arthritis: rheumatoid, hemophylia
- bone metabolism disorders.
- Obesity: Excess weight can strain the knees more, especially in young children. This additional pressure has the potential to worsen knee valgus and cause the knee joint to become misaligned.
- One of the most commonly held theories is that reduced gluteal activity levels allow for a greater degree of hip internal rotation and consequently also tibial rotation and therefore knee valgus.
Classification
Depending on the degree of deformity and the soft tissue involved, there are several grading systems for classifying knee deformities. However, the most current one describes three valgus deformity classes that are based on the angle’s degree.
- Grade I
The deviation is less than 10°, contraction of the lateral soft tissue but no elongation of the medial collateral ligament, and passively correctable.
- Grade II
The MCL is extended but still functioning, the lateral tissues are constricted, and the axial deviation is between 10 and 20°.
- Grade III
The lateral structures are taut, the medial stabilizers are non-functional, and the axial deformity exceeds 20°.
Risk Factor
→ It is most commonly implicated in injuries involving the anterior cruciate ligament (ACL) but it also features as a risk factor in respect of other leg injuries, including patellofemoral pain syndrome, knee osteoarthritis, medial collateral ligament sprains, and more general knee cartilage and meniscus damage.
Diagnosis
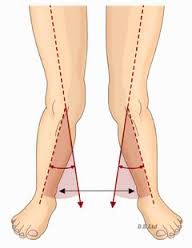
→ The degree of genu valgum can be estimated by the Q angle, which is the angle formed by a line drawn from the anterior superior iliac spine through the center of the patella and a line drawn from the center of the patella to the center of the tibial tubercle.
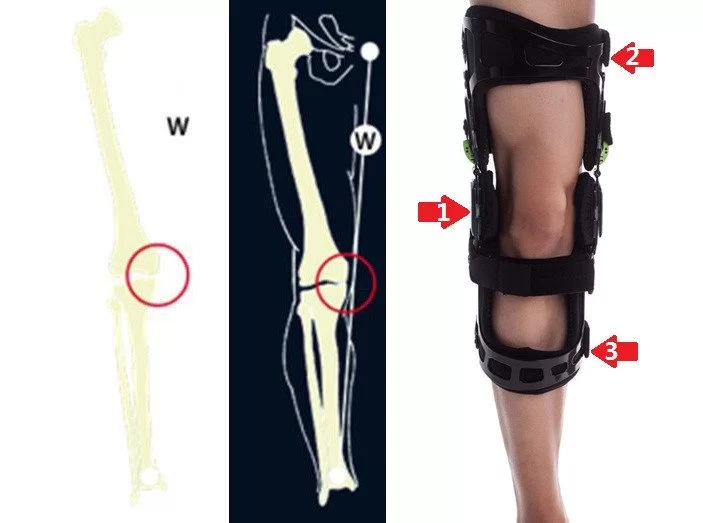
X-Ray of Knee Valgus Deformity


→ In women, the Q angle should be less than 22 degrees with the knee in extension and less than 9 degrees with the knee in 90 degrees of flexion.
→ In men, the Q angle should be less than 18 degrees with the knee in extension and less than 8 degrees with the knee in 90 degrees of flexion.
→ A typical Q angle is 12 degrees for men and 17 degrees for women.
Treatment
→ It is normal for children to have knock knees between the ages of two and five years of age, and almost all of them resolve as the child grows older.
→ If symptoms are prolonged and pronounced or hereditary, doctors often use orthotic shoes or leg braces at night to gently move a child’s leg back into position.
→ If the condition persists and worsens later in life, surgery may be required to relieve pain and complications resulting from severe or hereditary genu valgum. Available surgical procedures include adjustments to the lower femur and total knee replacement (TKR).
→ Weight loss and substitution of high-impact for low-impact exercise can help slow the progression of the condition.
Physiotherapy Treatment
→ Activating and developing the arches of the feet,
→ Waking up the outer leg muscles (abductors), and
→ Learning how to move the inner ankle bone inwards towards the outer ankle bone, and upwards towards the knee.
→ Strengthening exercise-



These all are Strengthening Exercises.

Surgical Treatment
Hemiepiphysiodesis
Hemiepiphysiodesis combined with guided growth is commonly used to repair angular abnormalities. Extraperiosteally implanted screws, plates, or staples are implant options. When a patient is older than 10 years old and their mechanical axis lies in the lateral quadrant of their proximal tibia, they may have medial-sided hemiepiphysiodesis about their distal femur and/or proximal tibia.
When physeal width and skeletal age are known, the Green-Anderson growth charts can be used to estimate when angular correction through epiphysiodesis will occur. Generally speaking, a correction is obtained more quickly for younger patients. In some situations, hardware removal can be necessary to prevent varus overcorrection. Given the propensity for “rebound” growth, it is advised to let overcorrection before removing hardware. Every four to six months, patients are closely observed.
Osteotomy
Genu valgum is also treated with osteotomies centered on the distal femur. When the deformity mostly affects the distal femur, a medial closing wedge osteotomy or a lateral opening wedge osteotomy may be used (most frequent). Patients who have reached or are approaching skeletal maturity and whose remaining growth is insufficient to benefit from directed growth are considered indications. If lengthening is also necessary, an external fixator can also be used.
Joint replacement surgery
Knee Joint replacement surgery may be required to replace the injured knee joint with an artificial prosthesis in cases of severe deterioration or deformity. When an older person has advanced knee arthritis, this is usually taken into consideration.
Post-operative Management
A thorough rehabilitation program following surgery is necessary to ensure optimal recovery, restore strength and mobility, and avoid problems. This program should include physical therapy and targeted exercises. Even if a surgical correction can significantly relieve pain and improve knee alignment, it is essential to stick to the post-operative recommendations given by the surgical team in order to guarantee a speedy recovery and favorable results over the long term. Knee valgus correction surgery carries some possible risks and problems, just like any other surgical operation. These should be discussed with the surgeon prior to the procedure.
Complications
When pathologic genu valgum is not recognized, complications may result. They typically have something to do with the underlying cause.
The following are a few of the side effects of surgical intervention:
- Physeal damage resulting from subperiosteal implant placement
- Over or below the deformity’s repair
- Infection
- Neurovascular injury
Prognosis
Cozen’s phenomena and physiological genu valgum are nearly always correct on their own. When the underlying problem is treated, pathologic genu valgum associated with metabolic bone disorders may improve. It is uncertain how frequently and to what extent juvenile genu valgum accompanies adult degenerative joint disease.
Conclusion
In children, genu valgum is a normal physiological process, but it can also be pathogenic if it’s connected to rickets, skeletal dysplasia, physeal injuries, tumors, or other conditions. Clinical diagnosis is established when increasing genu valgum is present after the age of seven.
A youngster under 7 years old who has genu valgum less than 15 degrees is treated with observation. If a child is more than seven years old and has a severe and progressive genu valgum, surgical intervention is recommended.
FAQs
What is genu valgum knee valgus?
A disorder known as knock knees (genu valgum) causes the knees to bend inward while the ankles stay apart. Although boys can also have the illness, ladies are significantly more likely to have it. Typically, a child’s natural growth and development include knock knees.
How do you treat genu valgum in the knee?
Time and regular growth and development are the only treatments for genu valgum. The majority of children with genu valgum recover on their own, but more testing and examination may be necessary if the knock-knees worsen or do not get better by the time
What is the cause of genu valgum?
The idea that medial metaphyseal overgrowth results from enhanced vascularity during fracture healing is the most widely accepted explanation for this phenomena. Radiation, infection, and tumours (osteochondromas, numerous hereditary exostoses, fibrous dysplasia) are some causes of genu valgum.
What is a knee valgus?
A lower leg malformation is known as valgus knee or knock knee results from the knee joint’s bone being tilted outward and away from the body’s midline. A valgus angle (Q angle) equal to or greater than 10° is the definition of this malformation.
Can knee valgus be corrected?
A V-shaped supracondylar osteotomy is an effective treatment for valgus abnormalities in the knee. Low morbidity, high stability with early weight-bearing, no requirement for internal fixation, and the option to modify alignment with a postoperative cast are the benefits of this very straightforward approach.
Is knee valgus good?
The valgus posture puts the knee at greater risk of damage. In reality, a knee valgus posture is strongly linked to a number of knee problems, including rupture of the anterior cruciate ligament (ACL).
References
- Patel, M. (2023, May 29). Genu Valgum. StatPearls – NCBI Bookshelf. https://www.ncbi.nlm.nih.gov/books/NBK559244/



2 Comments