Test for Cervical Instability:
- Instability in the cervical spine is most commonly the result of ligament damage [ transverse ligament, Alar ligaments], bone or joint damage [ fracture or dislocation ], or weak muscles [ deep flexors or extensors ].
- The instability may be the result of chronic arthritic conditions [ rheumatoid arthritis], trauma, long-term corticosteroid use, congenital malformation, down syndrome & osteoporosis.
- One commonly should have a high level of suspicion of instability if in the history the patient complains of instability, a lump in the throat, lip paresthesia, severe headache [ mostly with movement ]muscle spasms, nausea, or vomiting.
- If the examiner [ therapist ] anticipates doing mobilization [ mostly end-range techniques ] or manipulation techniques to the cervical spine, especially the upper cervical spine, a selection of appropriate clearing tests should be performed to rule out instability.
- If instability is present, mobilization & manipulation should not be performed.
Name of the special test of cervical instability:
- Anterior shear test
- Lateral flexion Alar ligament stress test
- Lateral [ transverse ] stress test
- Rotational Alar ligaments stress test
Anterior shear test:-

- This test is also known as the sagittal stress test.
- This anterior shear test is similar to the posteroanterior central vertebral pressure [ PACVP ] testing in the joint play section.
- Purpose = This anterior shear test is designed to test the integrity of the supporting ligament & capsular tissues of the cervical spine.
- Technique = The patient lies supine with the head in neutral resting on the bed.
- The examiner [ therapist ] applies an anteriorly directed force through the posterior arch of C1 or the spinous processes of C2 to T1 or bilaterally Through the lamina of each vertebral body.
- In each case, the normal end feel is tissue stretch with an abrupt stop.
- Result = Positive signs, especially when the upper cervical spine is tested, include nystagmus, pupil changes, dizziness, soft end feel, nausea, facial or lip paresthesia,& a lump sensation in the throat.
Lateral flexion Alar ligament stress test:-
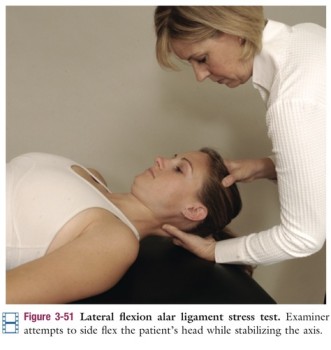
- Purpose = This lateral flexion alar ligament stress test is used to check the capsular & end feel of instability of the cervical spine.
- Technique = The patient lies supine with the head in the physiological neutral position while the examiner [ therapist ] stabilizes the axis with a wide pinch grip around the spinous process & lamina.
- The examiner [ therapist ] then attempts to side flex the head & axis.
- Result = Normally, if the ligament is intact, minimal side flexion occurs with a strong capsular end feel & a solid stop.
Lateral [ transverse ] stress test:
- Purpose = This lateral [ transverse ] stress test is used to determine instability of the atlantoaxial articulation caused by odontoid dysplasia.
- Technique = The patient lies supine with head supported.
- The examiner [ therapist ] places the radial side of the second metacarpophalangeal [ MCP ] joint of one hand against the transverse process of the atlas & the MCP joint of the other hand against the opposite transverse process of the axis.
- The examiner’s hands are then carefully pushed together, causing a shear force of one bone on the other.
- Normally, minimal motion & no symptoms are produced.
- Result = Because this test is normally painful because of the compression of soft tissues against the bone, the patient should be warned the pain is a normal sensation to be expected.
- The test can also be used to test other levels of the cervical spine [ C2 to C7 ].
Rotational Alar ligaments stress test:
- Purpose = This rotational Alar ligaments stress test is used to check the instability of the cervical spine.
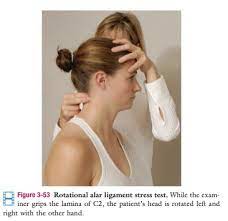
- Technique = The patient is in a sitting position.
- The examiner [ therapist ] grips the lamina & spinous process of C2 between the finger & thumb.
- While stabilizing C2, the examiner [ therapist ] passively rotates the patient’s head left or right moving to the no symptom side first.
- If more than 20 ‘ to 30’ rotation is possible without C2 moving, it is indicative of injury to the contra lateral Alar ligament especially if the lateral flexion Alar stress test is positive in the same direction.
- If the do the excessive motion is in the opposite direction for both tests, the cervical instability is due to an increase in the neutral zone in the joint of the cervical spine.
- Kaale et al. advocated doing the test differently.
- They advocate placing the patient in a sitting position.
- The examiner [ therapist ] supports the patient’s head against his or her body & place both hands on the same side of the patient’s occipitocervical junction.
- The lower hand stabilizes C2 by pressing the second & third fingers against the lateral aspect of C2 pulling it backward.
- The other hand is placed above with the third finger under the lateral mass of the atlas & the second finger under the mastoid process pulling upward into rotation.
- This test is performed in different angles of rotation to locate the position of maximum movement between C1 & C2.