
Dupuytren’s Contracture
What is a Dupuytren’s Contracture?
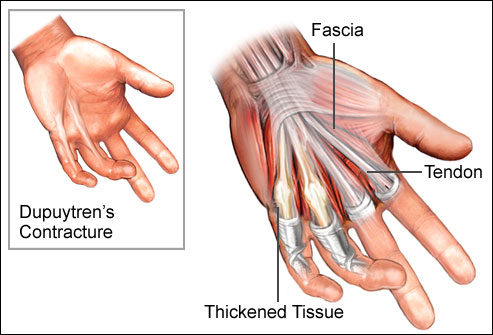
Dupuytren’s contracture is a condition in which one or more fingers become permanently bent in a flexed position. It usually begins as small hard nodules just under the skin of the palm. It then worsens over time until the fingers can no longer be straightened. While typically not painful some aching or itching may be present.
The ring finger followed by the little and middle fingers are most commonly affected. It can interfere with preparing food, writing, and other activities.
The cause is unknown. Risk factors include family history, alcoholism, smoking, thyroid problems, liver disease, diabetes, previous hand trauma, and epilepsy. The underlying mechanism involves the formation of abnormal connective tissue within the palmar fascia. Diagnosis is usually based on symptoms.
Initial treatment is typically with steroid injections into the affected area and physical therapy. Among those who worsen, clostridial collagenase injections or surgery may be tried.[ While radiation therapy is used to treat this condition, the evidence for this use is poor. The condition may recur despite treatment.
Dupuytren’s most often occurs in males over the age of 50. It mostly affects white people and is rare among Asians and Africans. In the United States, about 5% of people are affected at some point in time, while in Norway about 30% of men over 60 years old have the condition. In the United Kingdom, about 20% of people over 65 have some form of the disease. It is named after Guillaume Dupuytren, who first described the underlying mechanism in 1833.
Anatomy related to Dupuytren’s Contracture
The palmar aponeurosis (palmar fascia) invests in the muscles of the palm and consists of central, lateral, and medial portions.
The central portion occupies the middle of the palm, is triangular in shape, and is of great strength and thickness.
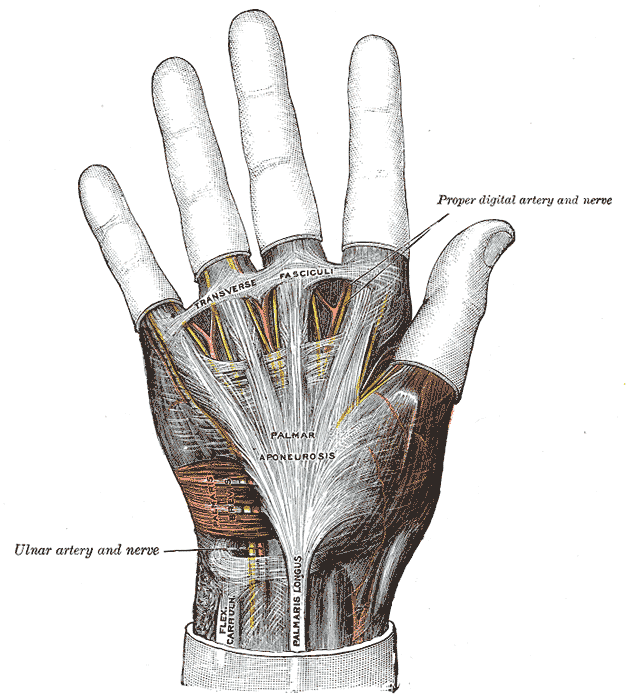
Its apex is continuous with the lower margin of the transverse carpal ligament, and receives the expanded tendon of the palmaris longus.
Its base divides below into four slips, one for each finger. Each slip gives off superficial fibers to the skin of the palm and finger, those to the palm joining the skin at the furrow corresponding to the metacarpophalangeal articulations, and those to the fingers passing into the skin at the transverse fold at the bases of the fingers.
The deeper part of each slip subdivides into two processes, which are inserted into the fibrous sheaths of the flexor tendons. From the sides of these processes offsets are attached to the transverse metacarpal ligament.
By this arrangement short channels are formed on the front of the heads of the metacarpal bones; through these the flexor tendons pass. The intervals between the four slips transmit the digital vessels and nerves, and the tendons of the lumbricales.
At the points of division into the slips mentioned, numerous strong, transverse fasciculi bind the separate processes together.
The central part of the palmar aponeurosis is intimately bound to the integument by dense fibroareolar tissue forming the superficial palmar fascia, and gives origin by its medial margin to the palmaris brevis.
It covers the superficial volar arch, the tendons of the flexor muscles, and the branches of the median and ulnar nerves; and on either side, it gives off a septum, which is continuous with the interosseous aponeurosis, and separates the intermediate from the collateral groups of muscles.
Lateral and medial portions
The lateral and medial portions of the palmar aponeurosis are thin, fibrous layers, which cover, on the radial side, the muscles of the ball of the thumb, and, on the ulnar side, the muscles of the little finger; they are continuous with the central portion and with the fascia on the dorsum of the hand
Pathophysiology of Dupuytren’s Contracture
The pathophysiology of Dupuytren disease involves abnormal myofibroblastic growth in the hand.
Type III collagen predominates, which under a non-disease state would be Type I collagen.
Dupuytren contracture progresses through three phases: (1) proliferative, (2) involution, and (3) residual. The proliferative phase has a characteristically high concentration of immature myofibroblasts and fibroblasts arranged in a whorled pattern.
In the involution phase, fibroblasts become aligned in the longitudinal axis of the hand following lines of tension. In the residual phase, relatively acellular collagen-rich chords remain causing contracture deformity.
The disorder is not always progressive and in at least 50-70% of patients, it may stabilize or even regress.
Several cords can develop which can cause unique deformities of the hand.
Pretentious cords cause skin pitting and metacarpal phalangeal (MCP) joint contracture.
Natatory cords are responsible for web space contractures.
Spiral cords are the most important in the disease process and can cause proximal interphalangeal (PIP) contracture.
Risk factors for increased severity and recurrence of disease after treatment include male gender; onset before age 50; bilateral disease; sibling/parent involvement; the presence of Garrod pads, Ledderhose, or Peyronies diseases.
Signs and symptoms of Dupuytren’s Contracture
Dupuytren’s contracture of the right little finger. The arrow marks the area of scarring
Typically, Dupuytren’s contracture first presents as a thickening or nodule in the palm, which initially can be with or without pain. Later in the disease process, there is a painless increasing loss of range of motion of the affected fingers. The earliest sign of contracture is a triangular “puckering” of the skin of the palm as it passes over the flexor tendon just before the flexor crease of the finger, at the metacarpophalangeal (MCP) joint. Generally, the cords or contractures are painless, but, rarely, tenosynovitis can occur and produce pain. The most common finger to be affected is the ring finger; the thumb and index finger are much less often affected. The disease begins in the palm and moves towards the fingers, with the metacarpophalangeal (MCP) joints affected before the proximal interphalangeal (PIP) joints.
In Dupuytren’s contracture, the palmar fascia within the hand becomes abnormally thick, which can cause the fingers to curl and impair finger function. The main function of the palmar fascia is to increase grip strength; thus, over time, Dupuytren’s contracture decreases a person’s ability to hold objects. People may report pain, aching, and itching with the contractions. Normally, the palmar fascia consists of collagen type I, but in Dupuytren sufferers, the collagen changes to collagen type III, which is significantly thicker than collagen type I.[citation needed]
Related conditions
Dupuytren’s contracture is related to a number of similar conditions that affect different areas of the body, including:
Garrod’s pads – nodules that develop on the back of the knuckles on the fingers
Ledderhose’s disease (plantar fibromatosis) – nodules and contractures that affect the foot
Peyronie’s disease – where the tissue of the penis is affected, causing it to become abnormally curved
Risk factors in Dupuytren’s contracture
Dupuytren’s contracture is a non-specific affliction but primarily affects:
Non-modifiable
For people of Scandinavian or Northern European ancestry, it has been called the “Viking disease”, though it is also widespread in some Mediterranean countries (e.g., Spain and Bosnia Dupuytren’s is unusual among ethnic groups such as Chinese and Africans.
Men rather than women; men are more likely to develop the condition)
People over the age of 50; the likelihood of getting Dupuytren’s disease increases with age.
People with a family history (60% to 70% of those afflicted have a genetic predisposition to Dupuytren’s contracture)
Modifiable
Smokers, especially those who smoke 25 cigarettes or more a day
Thinner people (i.e., those with a lower than average body mass index)
Manual workers
Alcoholics
Other conditions
People with a higher-than-average fasting blood glucose level
People with previous hand injury
People with Ledderhose disease (plantar fibromatosis)
People with epilepsy (possibly due to anti-convulsive medication)
People with diabetes mellitus
People with HIV
In one study, those with stage 2 of the disease were found to have a slightly increased risk of mortality, especially from cancer.
Diagnosis of Dupuytren’s Contracture
Types
According to the American Dupuytren’s specialist Dr Charles Eaton, there may be three types of Dupuytren’s disease:
Type 1: A very aggressive form of the disease found in only 3% of people with Dupuytren’s, which can affect men under 50 with a family history of Dupuytren’s. It is often associated with other symptoms such as knuckle pads and Ledderhose disease. This type is sometimes known as Dupuytren’s diathesis.
Type 2: The more normal type of Dupuytren’s disease, usually found in the palm only, and which generally begins above the age of 50. According to Dr Eaton, this type may be made more severe by other factors such as diabetes or heavy manual labour.
Type 3: A mild form of Dupuytren’s which is common among diabetics or which may also be caused by certain medications such as the anti-convulsants taken by people with epilepsy. This type does not lead to full contracture of the fingers and is probably not inherited.
Staging of Dupuytren’s disease.( TFD- Total flexion deformity )
Stage Deformity
0 No lesion
N Palmar nodule without presence of contracture
1 TFD between 0° and 45°
2 TFD between 45° and 90°
3 TFD between 90° and 135°
4 TFD greater tha
Treatment in Dupuytren’s contracture
Currently, there is no cure for Dupuytren’s; however, the condition is not dangerous.
Although it varies from patient to patient, Dupuytren’s usually progresses very slowly and may not become troublesome for many years. In fact, for some patients, the condition may never progress beyond developing lumps in the palm.
If the condition progresses, your doctor may first recommend nonsurgical treatment to help slow the disease.
1. Nonsurgical Treatment
Steroid injection. Corticosteroids are powerful anti-inflammatory medications that can be injected into a painful nodule. In some cases, a corticosteroid injection may slow the progression of a contracture. The effectiveness of a steroid injection varies from patient to patient.
Splinting. Splinting is not known to prevent the progression of a finger contracture. Forceful stretching of the contracted finger may not be helpful and, in fact, could cause an injury to the finger or hand.
Splinting may be used after surgery for Dupuytren’s contracture to protect the surgical site; however, it is not known if it reduces the risk of recurrent contracture or tightening of the healing wound.
2. Surgical Treatment
If the contracture interferes with hand function, your doctor may recommend surgical treatment. The goal of surgery is to reduce the contracture and improve motion in the affected fingers.
There is no known cure for Dupuytren’s contracture; however, surgery is intended to “set back the clock” by reducing the restricting effect of the cords by either disrupting or removing them. Unfortunately, the healing tissues will form with the same potential to develop cords in the future—but the gains in hand function can still be substantial.
The surgical procedures most commonly performed for Dupuytren’s contracture are:
Fasciotomy
Subtotal palmar fasciectomy
Fasciotomy.
Treatment is indicated when the so-called table top test is positive. With this test, the person places their hand on a table. If the hand lies completely flat on the table, the test is considered negative. If the hand cannot be placed completely flat on the table, leaving a space between the table and a part of the hand as big as the diameter of a ballpoint pen, the test is considered positive and surgery or other treatment may be indicated. Additionally, finger joints may become fixed and rigid.
3. Recent Developments in Treatment
The recently developed treatments described below are intended to reduce a contracture and improve motion in the affected fingers by disrupting the tethering effect of the Dupuytren’s cords.
Enzyme Injection
The injection of an enzyme solution for the treatment of Dupuytren’s contracture has recently been approved by the Federal Drug Administration. The enzyme, collagenase, is administered on an outpatient basis by doctors who have been specifically trained in the technique.
To begin, your doctor will inject the enzyme directly into the cords in your hand. During the 24 to 72 hours following the injection, the enzyme will weaken/dissolve the contracted tissue.
The next step is performed under local anesthesia. Your doctor will manipulate and straighten your bent fingers to break or pull apart the restrictive cords. Often, this improves the contracture and increases the range of motion in the fingers.
Enzyme injection typically results in less pain and swelling than major surgery. Although rare, the injection may cause an allergic reaction or flexor tendon rupture. Other potential complications are the same as those for surgery.
Early results for enzyme injection are promising, but long-term results and recurrence rates are not yet known.
4. Physiotherapy, massage, and exercise before surgery
Physiotherapy treatment may help relieve some of the pain and tension that patients feel in their hands or arms.
Massaging the palm of the hand and the forearm may help reduce the tension in the palmar fascia and the Palmaris Longus muscle (a muscle in most people’s arms that pulls on the fascia).
Physiotherapy will not remove the nodules, though some therapists can help with releasing tension in the arm and treating the tissues around the lumps to give relieve of pain and increase the range of movement. Physiotherapy can consist of massaging or exercises.
Some patients will wear splints to try slow down contracture, an example can be found on this page.
Acupuncture and reflexology are other treatments sometimes used to try slow or even reverse the progression.
Many consultants believe that physiotherapy will not stop the disease progress, but can help with the symptoms for a while.
Exercises are not commonly recommended and are unlikely to prevent contractures. However some patients do report good results, even if for a limited period of time until the condition worsens and they need further treatment.
Some treatments that have helped patients:
massaging the whole arm and hand to create good flow of fluid from the hand to the heart and from the heart to the hand.
gentle stretching exercises ( if stretching too vigorously you risk microtrauma to the fascia which can aggravate Dupuytren’s it should not be painful, at most a bit uncomfortable). Gentle stretching and holding the position for 10-15 seconds , then release and repeat 10 times is better and will tire the contracted strands more than brute force)
hot wax treatments to the hand or other warm applications, for many people applying heat or at least warmth first help to make exercises easier.
ultrasound treatment of the nodules to soften them and maybe reduce the pain after heat treatment or ultrasound, massaging sideways over the palm may help to loosen the tissues a bit, with the other hand or done by a professional with tools made for tissue release techniques.
wearing night splints, the idea being that at night many people have their fingers slightly curved which makes it easier for the contracture to settle in a curved position.
for painful palms or nodules a lot of patients wear weightlifting gloves that are padded in the palm, to protect their hand and reduce the pain, and still have good grip
There are different type of exercises with different goals.
Remember that most exercises work best if you stretch until you feel resistance, NOT stretch until it really hurts. Hold that tension for 10-15 seconds, release and repeat 10 times.
Tendon Glide exercises: are meant to make the deep and superficial flexor tendons (the ones that bend your fingers) move separately. The are done by making different types of fists, as shown in the pictures here, going from a flat hand via fingers only bend at the hand joint to a fist with bend fingers to a fist with fingers straight.
TENDON GLIDE 1:

TENDON GLIDE 2

TENDON GLIDE 3 EXERCISE

TENDON GLIDE 4 EXERCISE

TENDON GLIDE 5 EXERCISE

TENDON GLIDE 6 EXERCISE

Range of motion exercises: can be to stretch the fingers and joints or to widen the reach of the fingers. A lot of websites will give ideas for this, especially sites for guitar or piano players. Some examples follow here:
To strengthen the fingers and increase the reach:
Place your hand against each other with the fingers stretched and the tips touching, try pushing the palms together as well. If you can get palms and fingertips touching, try to push the fingertips of one hand away with the tips of the other hand.
Place hand on a flat tabletop. Lift the palm off the table while keeping your fingers on the table, to stretch the joints between the hands and fingers.
Place the hand flat on the table and try to lift each finger up separately
With the hand flat on the table try to spread your fingers as wide as they will go. Then move each finger toward the thumb (start with the index finger) while holding the hand flat to create as much space between the fingers as you can each time. This exercise can be doe the other way around as well by moving each finger toward the little finger.
Hold you hand up, and make the thumb touch the tip of each finger in turning, creating a circle of the finger and thumb.
Gripping exercises
Use a folded up towel, or a sponge (cut to size of you want). Place it in your hand and squeeze tight, then release after 10 seconds and repeat. Soft exercise balls or babies toy balls work as well.
Exercises after the surgery:
Exercises may need to be done for up to 6 months. Repeat each one 10 times, do at least 3 times per day. It may be easier to do the exercises with the hand in lukewarm water, soapy or plain.
Please note exercising can be uncomfortable but should not be really painful. It is better to go gently, hold for 10 seconds and release, and try to get more movement slowly than to force the issue, that may do damage!
Any exercises where you use the other hand to push the joints (passive exercises) are best only started when the wound has healed and any scabs have come off.
Straightening the fingers: (note that a swollen finger will not straighten completely)
Finger Walking (Spreading the finger)s Rest palm on flat surface, move thumb to the side, slide one finger at a time toward the thumb. Finger Walking (Spreading the finger)s Rest palm on flat surface, move thumb to the side, slide one finger at the time toward the thumb.
Tendon Glide
Start with the hand open, make a fist by bending each joint one by one, then open the fist the same way.
Cat’s Paw– open hand wide, bend the fingertips but not the large knuckles, hold six seconds.
Making a fist (whole hand, try first around a ping pong ball or even small foam ball or sponge, later without anything between the fingers and the palm)
Making a fist finger by finger by using your other hand to bend the joints, passive exercises, only start these when the wound has healed and any scabs have come off.
Use the other hand to gently bend the affected finger at the large knuckle, hold for 10 seconds.
Complications
As with any surgery, there are risks associated with surgery for Dupuytren’s contracture. The likelihood of complications increases with the following:
The severity of the contracture
The number of contractures addressed in a single procedure
The presence of any other medical conditions
Possible risks and complications of surgery for Dupuytren’s include:
Pain
Scarring
Injury to nerves and/or blood vessels
Wound infection
Stiffness
Loss of sensation. Temporary loss of sensation may result from stretching nerves that have been contracted for a long time.
Loss of viability of a finger/loss of a finger (rare)
Prognosis
Dupuytren’s disease has a high recurrence rate, especially when a person has so called Dupuytren’s diathesis. The term diathesis relates to certain features of Dupuytren’s disease and indicates an aggressive course of disease
The presence of all new Dupuytren’s diathesis factors increases the risk of recurrent Dupuytren’s disease by 71% compared with a baseline risk of 23% in people lacking the factors. In another study the prognostic value of diathesis was evaluated. They concluded that presence of diathesis can predict recurrence and extension. A scoring system was made to evaluate the risk of recurrence and extension evaluating the following values: bilateral hand involvement, little finger surgery, early onset of disease, plantar fibrosis, knuckle pads and radial side involvement.
Minimally invasive therapies may precede higher recurrence rates. Recurrence lacks a consensus definition. Furthermore, different standards and measurements follow from the various definitions.[citation needed]
Post-operative care
Postoperative care involves hand therapy and splinting. Hand therapy is prescribed to optimize post-surgical function and to prevent joint stiffness.[citation needed]
Besides hand therapy, many surgeons advise the use of static or dynamic splints after surgery to maintain finger mobility. The splint is used to provide prolonged stretch to the healing tissues and prevent flexion contractures. Although splinting is a widely used post-operative intervention, evidence of its effectiveness is limited, leading to variation in splinting approaches. Most surgeons use clinical experience to decide whether to splint. Cited advantages include maintenance of finger extension and prevention of new flexion contractures. Cited disadvantages include joint stiffness, prolonged pain, discomfort, subsequently reduced function, and edema.
A third approach emphasizes early self-exercise and stretching.
Author: Nitesh Patel - Physiotherapist
Physiotherapist in Samarpan Physiotherapy Clinic Ahmedabad Bapunagar Amaraiwadi Vastral Mobile Physiotherapy Clinic Dr. Nitesh Patel ( Physiotherapist ) : Mo No : 09898607803





My wife suffers from left hand mild dupuytrens contracture, which is painful and causes problems with gripping items.She also suffers pain in her right side from a shoulder fracture. I have to assist my wife with dressing, washing etc. She has been advised that “power-gripping” is the answer. What is “power-gripping? Will it help? Regards Terry