Esotropia
What is Esotropia?
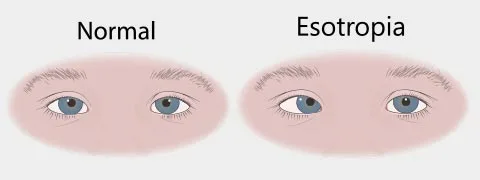
The Esotropia word derives from Greek, where eso- indicates inward, and trope suggests turn. Esotropia is an eye disease that guides either one or both of your eyes pointing inward. Esotropia is a variety of strabismus, which suggests that your eyes don’t line up perfectly. You may hear someone talking about crossed eyes rather than esotropia. Esotropia can be monocular (which includes one eye) or binocular (which includes both eyes).
The muscles and nerves that maintain your eyes generally work to permit both of your eyes to work jointly. In esotropia, this power isn’t as coordinated as it should be.
What Are the Types of Esotropia?
There are several varieties of esotropia, and an eye care professional will determine the therapy based on specific characteristics:
Age of onset: Esotropia may be hereditary or acquired at any age.
Frequency: Esotropia may be continuous or intermittent.
Eye focusing: Esotropia may be generated by the eye-straining to see absolutely (accommodative vs. nonaccommodative).
Congenital Esotropia
Congenital esotropia, also called infantile esotropia, forms within the first six months of life. Though it is known as congenital esotropia, this state infrequently presents at birth. The reason for congenital esotropia is unfamiliar, but it is familiar and involves one in 50 newborns.
Transient misalignment of the eyes is familiar up to 3 months old, and should not be mistaken for infantile esotropia.
Acquired Esotropia
Acquired esotropia occurs later in life, and can evolve in kids and grown-ups as an outcome of injuries or disorders. An infrequent subtype of acquired esotropia known as acute acquired comitant esotropia is indicated by the sudden beginning of a fairly large angle of esotropia, along with diplopia (double vision) and the tiniest refractive error, where your eye isn’t turning light perfectly, resulting in a blurred vision.
Acquired esotropia is generally managed with eyeglasses, but some circumstances may not enhance with corrective lenses.
Constant Esotropia
Constant esotropia happens when the eye is rotated inward all the time. Most patients with esotropia are constant, but some circumstances of accommodative esotropia are intermittent.
Intermittent Esotropia
The intermittency of accommodative esotropia is attributed to the irregular accommodative status of the person as their eyes work to focus. Without therapy, intermittent esotropia is probable to turn into constant esotropia. The intermittent strabismus noticed in infants is associated with regular development and generally goes out before 3 months of age.
Accommodative Esotropia
Accommodative esotropia also called refractive esotropia, guides to eye crossing that is induced by the focusing steps of the eyes as they attempt to see absolutely. The focusing step is known as accommodation. A person with this kind of esotropia generally has hyperopia (farsightedness), where a patient can’t see close things perfectly. It is familiar and includes 50% of all childhood esotropia circumstances.
Accommodative esotropia can be categorized into three varieties: refractive, non-refractive, and partially accommodative or decompensated. All three states have an age of beginning between 6 months and 7 years. It is often associated with amblyopia (lazy eye, or low vision due to irregular visual development).
If the angle of the esotropia is completely fixed with glasses, the strabismus is said to be a completely accommodative esotropia. If the angle of the strabismus is not completely fixed with glasses, it is known as partly accommodative esotropia. Subjects, where there is no change in the angle of strabismus with glasses, are nonaccommodative esotropia.
Nonaccommodative Esotropia
Acquired nonaccommodative comitant esotropia guides to a group of diseases not associated with accommodating action. It is not related to any refractive issues, but it can be associated with an intracranial tumor or different central nervous system (CNS) lesions.
Nonaccommodative esotropia can’t be corrected with glasses. Nevertheless, persons can frequently have this issue fixed with surgery.
Symptoms of Esotropia
Symptoms of esotropia contain:
- inward turning of the eyes
- crossing of the eyes
- lazy eye
A person with esotropia may see that they cannot concentrate their eyes on the same spot at the exact time, and they may solely be capable to see things completely with one eye.
Complications
Infants and young kids may experience:
- loss of 3-D vision
- problems with depth perception
- amblyopia (loss of eyesight in the crossed eye)
Yet, if congenital esotropia is managed in infancy, difficulties are less probable to be experienced long-term.
More senior kids and grown-ups that acquire esotropia can form:
- diplopia (double vision)
- reduced binocular vision (the capability of the eyes to function together)
- depth perception problems
Causes of Esotropia
Strabismus may conduct in the family. Yet, involved family members do not necessarily convey the same kind or severity of strabismus. A kid with a family record of strabismus should be seen by a pediatric ophthalmologist.
Other issues like hyperthyroidism, diabetes, and neurologic issues can also generate esotropia.
In Children
Esotropia may be noticed in kids with extremely poor vision in one eye or in association with specific genetic conditions that involve the eyes. Kids can also form strabismus after congenital cataract surgery.
Yet, crossed eyes in childhood are generally induced either by idiopathic infantile esotropia, suggesting the reason is unknown, with early beginning within the first six to eight months of life, or accommodative esotropia, which is first recorded between 1 and 4 years of age, in association with raised levels of farsightedness.
In Adults
Some diseases that can induce esotropia in adults to contain:
Stroke: During a stroke, ocular motility abnormalities can happen, indicating abnormal eye alignment or problems in controlling eye actions, and result in strabismus. It is one of the most familiar elements of stroke.
Thyroid eye disease: Strabismus in thyroid eye condition is an outcome of inflammation and thickening of the extraocular muscles. This can limit eye motion, generating misalignment and double vision.
Neurodegenerative disorders: Keeping right eye alignment is required to develop a cohesive visual picture. This affects the coordination of complex neural networks, which can evolve damaged by various neurodegenerative conditions. Thus, different varieties of strabismus can be activated by Huntington’s or Parkinson’s disease, for instance.
Sixth cranial nerve palsy: Sixth cranial nerve palsy is a weakness of the nerve that innervates the lateral rectus muscle, which prevents the lateral motion of the eyeball. The lateral rectus muscle turns the eye out from the nose. When the lateral rectus muscle is sickly, the eye transits inward toward the nose, resulting in an esotropia.
Risk factors
Some factors raise the risk of having esotropia, involving:
- a family record of strabismus
- having another eye disease, like cataracts or glaucoma
- certain medical diseases, like diabetes and overactive thyroid
- neurological diseases, involving extreme fluid in the brain
- premature birth
- stroke
There are no known risk elements for youth esotropia.
Differential Diagnosis
It is important to determine esotropia from different close differentials, as discussed beneath:
Pseudoesotropia – can be differentiated from true esotropia by the presence of major epicanthic folds, small interpupillary length, negative angle kappa, or an overly broad nasal bridge.
Ciancia syndrome – This is indicated by the presence of large-angle esodeviation (>60 prism diopters). Both eyes seem to be clung towards the nose, restricted bilateral abduction with right abduction saccades, jerk endpoint nystagmus on tried abduction, face turn towards specifying eye, with no nystagmus on adduction, and a tight medial rectus muscle on forced duction examination.
Congenital fibrosis syndrome – This is also known as strabismus fixus. The person generally presents with large-angle esotropia with extreme limitation of abduction of one or both eyes. Frequently, a family record is present in these issues and displays an autosomal dominant inheritance design.
Congenital sixth nerve palsy – These can present as unilateral or bilateral issues. Doll’s head trick reveals restricted abduction established on laterality.
Nystagmus blockage syndrome – guides to a situation in which esotropia happens in a kid with congenital nystagmus. It is suggested that esotropia happens secondary to an adduction or extreme convergence to decrease nystagmus. Few writers have suggested the two parts of esotropia in these circumstances a static angle of infantile esotropia and a superadded dynamic angle of esotropia due to convergence to exhaust the nystagmus.
Cyclic Esotropia – Alternate repeated strabismic and non-strabismic stages describe this form. The cycles may differ from 24 hours of strabismic and non-strabismic stages or 48 hours or 72 hours of cycles per. This state of strabismus can be obtained at any age but is most generally noticed between 2 to 6 years.
Microtropia – This is indicated by a slight angle of heterotopia in the range of 1 to 5 degrees. Further clinical features contain a comparable scotoma on the fovea, mild amblyopia, abnormal retinal correspondence, impaired stereo acuity, and a normal or near-normal peripheral fusion with amplitudes.
Diagnosis
An eye care specialist or doctor diagnoses esotropia by bringing a family record and conducting a complete eye examination. During the examination, they will pay close concentration to how the eyes concentrate and move.
Tests and methods used to diagnose strabismus contain:
Corneal light reflex test: Also called the Hirschberg test, this is a fast way to study ocular alignment, particularly in young kids. During the examination, a patient’s attention is attracted to a mark (a light or a brightly colored thing), while the light in front of them is produced in their eyes. This permits the specialist or doctor to inspect whether the eyes are symmetrical.
Cycloplegic refraction: The eye care specialist or doctor will calm the focusing muscle of your eye utilizing cycloplegic eye drops. This permits them to specify the full refractive error.
Cover-uncover test: This examination estimates deviation and eye motion. Your eye care provider or doctor will ask you to fixate on a mark. The specialist or doctor will protect one eye and watch how the uncovered eye reacts.
Prism cover test: This examination is utilized to estimate the angle of deviation. Your eye care provider or doctor will use a prism bar to protect the misaligned eye, following the exact direction as the deviation.
Treatment of Esotropia
The treatment for esotropia relies on the severity of the situation, and the length of time it has been current.
Different factors informing the therapy plan contain whether misalignment is current in one or both eyes, and whether the esotropia is accommodative or not.
Treatment always purposes at:
- eye alignment
- fixing double vision
- decreasing vision issues in both eyes
- fixing lazy eye
Treatment options contain:
Glasses or contact lenses: This is frequently the first line of therapy. Prescription glasses can fix eye misalignment or farsightedness. If a patient’s eyes still cross while wearing the glasses, they may need a bifocal lens.
Vision therapy: Eye activities may assist to boost eye function and the muscles near the eye to enhance vision. One state of vision treatment includes wearing a patch over the uninvolved eye to enhance the role of the crossed eye.
Botox injections: Botox may be injected to realign the eyes of some patients who have gentle esotropia.
Patching: is the common method for the therapy of amblyopia, and may also be useful in ameliorating small angles of strabismus as well as promoting the growth of binocular vision.
Surgery: Some patients may need surgical therapy to alter the length of the muscles near their eyes, although this does not ever fully remove the requirement to wear glasses or contact lenses.
Surgery is mostly conducted on infants with esotropia, but some grown-ups may also undergo a surgical process.
Esotropia may fix without any intervention in babies less than 5 months old, particularly if the symptoms are gentle and the eye misalignment is irregular.
Exercises: are commonly not useful in esotropia. Time consumed in this plan may slow the right diagnosis and adequate treatment, and therefore may compromise results.
Physiotherapy treatment in Esotropia
Pencil pushups
Pencil pushups are easy ocular movements that bring both eyes aimed at the exact fixed point. They are also called near the point of convergence activities.
Begin by maintaining a pencil out at arm’s length, pointing it out from you. Concentrate your gaze on the eraser or numeral or letter on the side. Gradually move the pencil toward the bridge of your nose. Maintain concentration for as long as you can, but quit once your vision brings blurry.

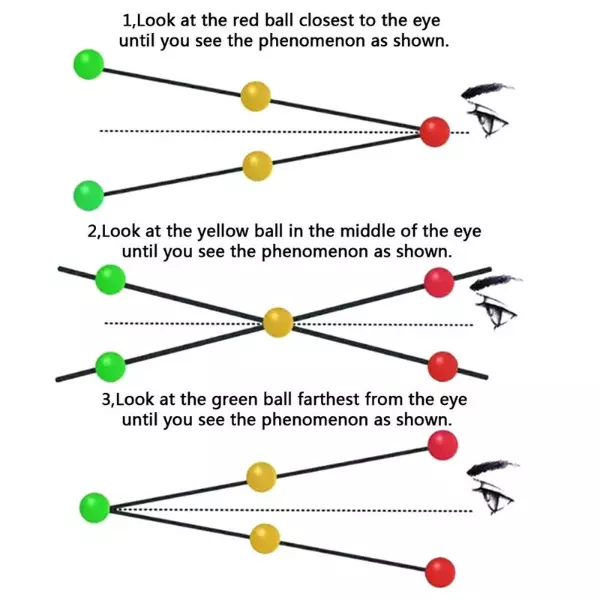
Brock string
Swiss optometrist Frederick Brock created this activity to enhance eye coordination. You’ll require a string approximately 5 feet long with three various colored beads.
Assure one end of the string to a fixed point like a handrail or the back of a chair. Space the beads out at similar lengths. Maintain the further end of the string tightly to your nose.
You should notice a consistent way as you move your focus from bead to bead. The dot you are looking at will seem by itself at the crossroad of two identical strings with doubles of the different beads, creating an X. Your eyes are not correctly concentrated on the bead if you notice the strings crossing in front of the bead or back of the bead. Be certain you can obtain the X at all beads (but the one at the distant end, which will solely have the two strings arriving out toward you in a V).
Reposition the beads along the string and resume the activity.
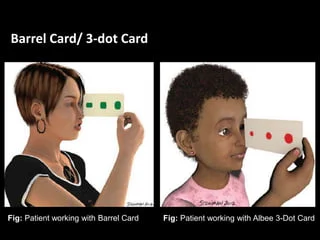
Barrel cards
This is a handy activity for exotropia. Draw three barrels of evolved size in red lengthwise on one side of a card. Accomplish the same item in green on the further side.
Maintain the card lengthwise and vertically opposite your nose so that the biggest barrel is most distant away. Stare at the distant barrel until it evolves into one picture with both colors and the different two barrel pictures have doubled.
Hold your gaze for approximately five seconds. Then reprise with the middle and smallest barrel pictures.
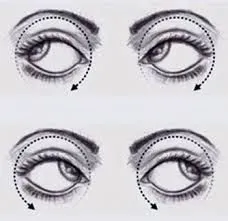
Eye Roll Exercise
This eye roll activity is designed to boost your eye muscles as well as asset relax your eyes. Begin by sitting down in a chair with your back erect and your feet firmly touching the bottom. Shut both of your eyes, putting your fingertips on the tops of both of your eyelids. Create certain that you are depressing on your eyelids with just three fingers per hand. From here, complete one full eye roll in a clockwise order. Move your eyes in the opposite order one time. Recount this movement back and forth until you have conducted the movement 50 times. Conduct three to five days a week, relying on your eye strength.
Computer Vision Therapy
Computer vision therapy activities are designed to assist decrease the result of esotropia on your vision. Sit in front of your computer with your back erect and your eyes level with the computer screen. Utilizing any basic vision schedule, like Home Vision Therapy, conduct computer-based eye movements for an hour or more a day 2. Numerous of these computer activities instantly target problems with convergence and perform on boosting your eye muscles to assist eliminate these issues. Activities include small dots on your screen connecting at the center of the screen. Both of your eyes must observe the different dots until they converge in the center of the screen.
Prognosis
In General, the prediction of esotropia is fine. Well-planned management system, close follow-up, and observance of therapy are the major factors on which prediction depends. Though most concomitant esotropia can be supervised conservatively, congenital esotropia needs surgical intervention. There are two various schools of thought regarding earlier versus late surgical intervention for congenital esotropia.
It is now thought that early ocular alignment before the age of 2 years results in finer visual acuity and conservation of binocular fusion to some time, frequently affecting peripheral fusion. Analyses have shown that adequate long-term stability, more suitable stereopsis, and sensorimotor growth have been associated with the early alignment of the eyes. It is essential to mention that the reoperation rates in congenital esotropia have been registered as elevated as 50%.
FAQ
Can esotropia be corrected?
Esotropia, a kind of eye misalignment, occurs when one or both eyes turn inward toward your nose. Standard treatments include glasses or contact lenses, surgery, or injections of botulinum toxin.
Is esotropia the same as the lazy eye?
The most familiar of these misalignments are esotropia, generally known as crossed eyes and occasionally directed to them as lazy eyes or squint. Approximately 1 to 2 percent of kids will have esotropia.
Is esotropia a birth defect?
Congenital (infantile) esotropia is a kind of strabismus that first occurs sometime within the first six months of life. This esotropia may be current at birth but frequently grows within the first few months. In the first months of life, it is familiar for the eyes to intermittently evolve misaligned.
How do you fix esotropia naturally?
Pencil pushups
Begin by maintaining a pencil out at arm’s length, pointing it out from you. Concentrate your gaze on the eraser r or numeral or a letter on the side. Gradually push the pencil toward the bridge of your nose. Hold it in your direction for as prolonged as you can, but prevent it once your vision brings blurry.
Does esotropia get better with age?
Yes, kids can outgrow accommodative esotropia. This generally occurs during the grade school and juvenile years as a kid evolves less farsighted. It is hard to indicate early in youth whether any given kid will outgrow their requirement for glasses.