Gemelli Muscles
Gemelli Muscles Anatomy
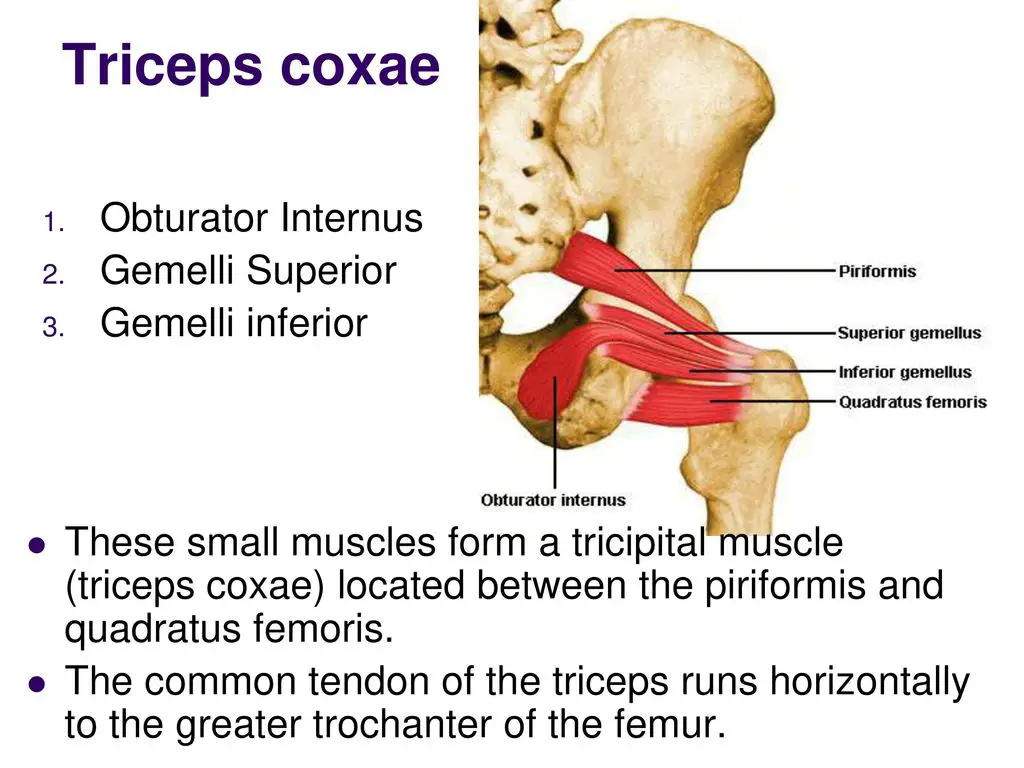
Often referred to as the gemelli muscles, the superior and inferior gemellus muscles are a pair of tiny, triangle-shaped muscles located between the gluteal and posterior hip musculature in the posterior proximal lower limb. In the gluteal area of the proximal thigh, there are six short external rotator muscles, of which the gemelli muscles are two.
The quadratus femoris, obturator externus, piriformis, and obturator internus are the remaining external rotators. Occasionally called the triceps coxae, the superior and inferior gemelli form a conjoined tendon that joins the obturator internus.
The deep gluteal space syndrome, also known as gemelli-obturator syndrome, is a sciatic nerve dysfunction that is related to the gemelli muscles, which help in thigh external rotation. Along with the obturator internus, the gemelli muscles are crucial surgical landmarks in the Kocher-Langenbeck and posterior approaches to the hip.
They are also necessary for locating and protecting the medial circumflex femoral artery. Surgical hip dislocations, complete hip replacement, hip hemiarthroplasty, loose body excision, treatment of posterior wall and column acetabular, and pelvic ring fractures can all benefit from the surgical techniques discussed.
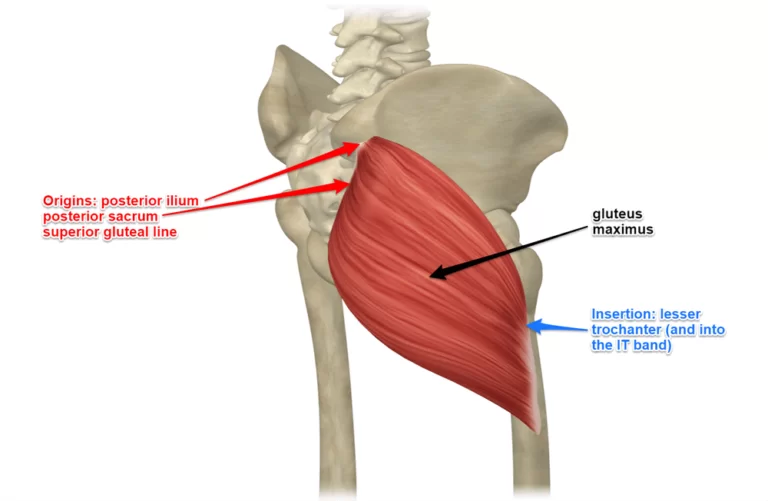
Origin and Insertion
The ischial tuberosity is the source of the inferior gemellus muscle, whereas the superior gemellus muscle begins at the ischial spine. The two gemelli muscles insert on the posteromedial surface of the greater trochanter of the femur, together with the obturator internus.
Function
The external (lateral) rotation of the thigh and the extension of the hip are the principal actions of the gemelli muscles. In the flexed position, they also aid in the abduction of the hip. Together with the obturator internus and the remaining short external rotator, the two gemelli muscles provide movement.
Blood Supply
The superior and inferior gemelli muscles are supplied by the inferior gluteal artery. The inferior gluteal artery originates from the internal iliac artery’s anterior trunk, travels through the sacral plexus’s second and third segments, and emerges from the larger sciatic foramen beneath the piriformis to nourish the gemelli muscles.
Lymphatic Drainage
There are two main categories of lower limb lymphatic vessels: superficial and deep channels. A medial group that follows the bigger saphenous vein and a lateral group that follows the small saphenous vein comprise the lower limb’s superficial lymph veins. The peroneal, posterior, and anterior tibial deep lymph vessels all run parallel to the appropriate vascular pathways.
The popliteal, superficial inguinal, deep inguinal, external iliac, lumbar, or aortic lymph nodes are the lymph nodes that receive drainage from the lower limb lymph veins.
Nerve Supply
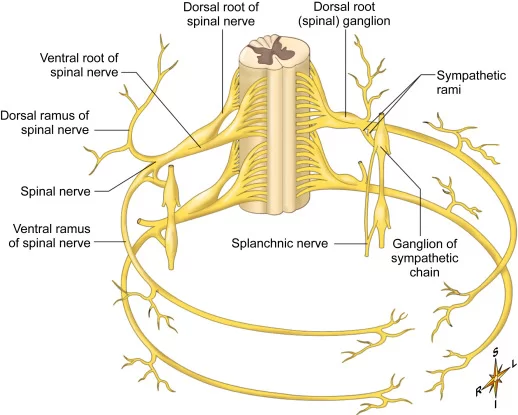
The nerve supplies innervation to the quadratus femoris (L4-S1) from the inferior gemellus muscle and the obturator internus (L4-S2) from the superior gemellus muscle. Every one of these nerves stems from the sacral plexus. The first four sacral ventral rami (L4-S4) and the fourth and fifth lumbar ventral rami combine to produce them.
The larger sciatic foramen is where the nerve that supplies the obturator internus exits the pelvis inferior to the piriformis muscle. The nerve innervates the superior gemellus throughout its passage, innervating the obturator internus on its way back into the pelvis via the smaller sciatic foramen.
The larger sciatic foramen, located deep in the piriformis muscle, is where the quadratus femoris nerve leaves the pelvis. It supplies the inferior gemellus muscle as it descends deeply to the short external rotators, which terminate on the deep surface of the quadratus femoris.
Embryology
Around four to five weeks into the embryo’s gestation, the limb buds begin to develop. The mesoderm migrates into the limb bud and forms an anterior and posterior condensation, which eventually gives rise to the lower limb’s skeletal and muscular components.
Myoblasts move out of the somites in the fourth or fifth week of gestation. The lower limb’s flexor and adductor musculature will arise from the anterior condensation, or ventral muscle mass, and the lower limb’s extensor and abductor musculature, from the posterior condensation, or dorsal muscle mass.
The creation of limb bud musculature is influenced by several variables, including as HOX genes, retinoic acid, sonic hedgehog (SHH), apical ectodermal ridge (AER), and the zone of polarizing activity (ZPA). The global organizing gradient known as retinoic acid triggers the synthesis of transcription factors that determine limb polarization and regional differentiation. Fibroblast growth factor (FGF) is produced by the apical ectodermal ridge (AER) and stimulates mitosis to augment limb buds.
This mechanism depends on the activity of FGF and AER; limb growth may stop in the absence of the proper signals. FGF10 is the particular fibroblast growth factor that plays a role in hindlimb development. It is induced by T-box transcription factor 4 (Tbx4).
Anatomical Variations
Because of their similar insertion and function, the superior gemellus, inferior gemellus, and obturator internus muscles were once thought to be a single muscle. According to available data, these muscles have distinct origins and innervations, which implies they are distinct entities.
Numerous writers have documented the existence of physiological differences in the gemelli muscles, such as having two superior gemelli, not having both gemelli, and having different origins and insertions. Surgeons may find it easier to reach this area during surgical intervention if they are aware that anatomical variances may exist.
Clinical Importance
Sciatica and posterior hip or gluteal pain are two of the more prevalent diagnoses and treatment issues that orthopaedic surgeons and general practitioners deal with. The phrase “piriformis syndrome” used to refer to a number of illnesses in this area. With the development of imaging tools and the assessment of nerve and muscle kinematics, the term “deep gluteal syndrome (DGS)” has become the preferred nomenclature. Due to non-discogenic sciatic nerve entrapment, DGS is characterized by pain and/or dysesthesias in the buttocks, hip, or posterior thigh, with or without radicular discomfort.
DGS includes a number of pathologic conditions, such as tumoral compression, gemelli-obturator syndrome, and piriformis syndrome. When the gemelli obturator complex is extended, the sciatic nerve is dynamically compressed, resulting in gemelli-obturator syndrome. The sciatic nerve passes via the triceps coxae and piriformis muscles, deep and superficially, respectively. As a result, this interaction may compress the sciatic nerve, causing sciatic pain to manifest clinically and necessitating its inclusion in the differential diagnosis of non-discogenic sciatica.
Imaging methods and physical examination procedures can help provide a reliable diagnosis for DGS by helping to distinguish between its causes. A physician using magnetic resonance imaging (MRI) can help assess anatomical variations in soft tissues. Physical therapy, anti-inflammatory medications, and imaging-guided intra- and/or extra-articular injections are commonly used in the treatment of DGS in order to address the underlying cause. Surgical treatment (open or endoscopic) may be considered in rare instances where conservative treatments (physical therapy, analgesics, anti-inflammatory medications, and injections) fails.
Surgical Considerations
The posterior surgical approach to the hip is the most frequent surgical use of the gemelli muscles. A frequent surgical technique for both total and partial hip arthroplasty is the posterior approach to the hip, often referred to as the Kocher-Langenbeck method. This route has various benefits, including a clear anatomical layer, a decreased incidence of heterotopic ossification, and undamaged hip abductors.
After the initial approach, the muscles of the triceps coxae are raised from their insertion site by about 1 to 2 cm on the back of the greater trochanter.
The conjoint tendon may be elevated straight off the bone per the surgeon’s discretion. Although these muscles are prone to injury, there is disagreement on the best ways to prevent damage, whether or not to heal the muscles, and how the repair will turn out.
Current research shows that a comprehensive posterior capsule repair, with special attention to the deep external rotators, such as the triceps coxae muscles, significantly lowers the likelihood of posterior dislocation.
To lower the risk of reduction and promote postoperative recovery and rehabilitation, an efficient repair of the gemelli and obturator internus muscles may be crucial early in the postoperative phase.
FAQ
What do the Gemelli muscles do?
The gemellus superior and inferior, like the internal obturator muscle, aid in maintaining the femoral head’s position in the acetabulum. By supporting the internal obturator, both muscles also aid in the laterally rotation of the extended thigh and the abduction of the flexed thigh at the hip.
What are the obturator internus and gemelli muscles?
Because of their similar insertion and function, the superior gemellus, inferior gemellus, and obturator internus muscles were once thought to be a single muscle. According to available data, these muscles have distinct origins and innervations, which implies they are distinct entities.
Where are the Gemelli muscles located?
The lower limb’s gluteal area contains the superior and inferior gemelli muscles. Their form is triangular and thin, with the obturator internus tendon dividing them. Attachments: The ischial spine is the place where the superior gemellus muscle begins.
What is the pain in the Gemellus muscles?
The condition known as gemellus pain syndrome normally comes on by hypertight hip flexor muscles, which overcompensate and overwork the deep hip rotator muscles.
What is the Gemelli muscle in radiology?
The tricipital (three-headed) triceps coxae, which fills the space between the inferiorly located quadratus femoris muscle and the superiorly located piriformis muscle, is formed by the small, triangular superior gemellus muscle, inferior gemellus muscle, and obturator internus muscle.
How do you stretch Gemellus?
With the elbows on the outside of the right knee, bend forward and plant your hands on the ground. Strive to maintain balance on the ball of the left foot while you push the left leg straight out and lower your hips. On the opposite side, carry out the same exercise. Do ten reps on each side.
References
Lezak, B. (2023, August 21). Anatomy, Bony Pelvis and Lower Limb, Gemelli Muscles. StatPearls – NCBI Bookshelf. https://www.ncbi.nlm.nih.gov/books/NBK557420/