
Suprascapular Nerve
The suprascapular nerve is the lateral branch of the superior trunk given by the brachial plexus. It receives nerve fibers that originate in the nerve roots C5 & C6[ & sometimes C4]. The suprascapular nerve is a mixed nerve, meaning that it gives both sensory & motor supply to the suprascapular region.
The main function of this nerve is to give motor supply to two muscles, which are the supraspinatus and infraspinatus muscles. These two muscles are part of the muscle group called the rotator cuff muscles. In addition, the suprascapular nerve gives a sensory supply to the joints of the scapula (glenohumeral & acromioclavicular joints).
Origin & course of Suprascapular nerve
The suprascapular nerve (root value C5, C6) starts from the superior trunk of the brachial plexus. It is contemplated to be one of the preterminal branches or supraclavicular branches of the brachial plexus cooperatively with the dorsal scapular nerve, long thoracic nerve, subclavian nerve & accessory phrenic nerve.
course
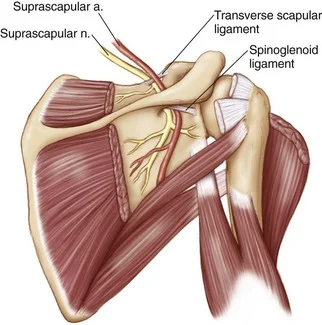
From its origin, the suprascapular nerve runs laterally, passing superior to the brachial plexus & through the posterior triangle of the neck. It then crossways the scapular notch (inferior to the superior transverse scapular ligament) into the supraspinous surface of the scapula. Here, it gives off a branch to the supraspinatus muscle & continues through the greater scapular (spinoglenoid) notch between the root of the spine of the scapula & the glenoid cavity, to reach the infraspinous fossa.
The nerve definitely terminates within the infraspinatus muscle, supplying it. To avoid confusion, the path of the suprascapular nerve differs from the suprascapular artery & vein, which runs above the superior transverse scapular ligament.
Branches & innervation
- Supraspinatus muscle
- Infraspinatus muscle
- Supraspinatus muscle
- Musculus supraspinatus
The suprascapular nerve is a mixed nerve. Its main function is to give motor supply for two of five muscles of the rotator cuff, including:
- supraspinatus muscle
- infraspinatus muscle
the nerve gives off a sensory branch that gives sensory supply to two joints
- Glenohumeral (shoulder joint)
- Acromioclavicular joint
Clinical relations
Suprascapular nerve entrapment
Suprascapular nerve entrapment (suprascapular neuropathy) is an uncommon syndrome characterized by pain & muscle weakness in the posterior shoulder region, resulting in weakened abduction & external rotation of the shoulder. It is usually caused by a traumatic injury to the suprascapular nerve which causes damage to its nerve fibers & results in weakness of the supraspinatus & infraspinatus muscles. The other recurrent cause is traumatic or non-traumatic compression of the nerve on its path through the suprascapular notch.
Etiology
Common sites for suprascapular nerve compression
Compression neuropathy develops from nerve entrapment is the most common cause of suprascapular nerve palsy. The common sites of nerve entrapment are the suprascapular notch & the spinoglenoid notch.
- Trauma to the shoulder resulting from fractures of the scapula, clavicle & proximal humerus can significantly damage the suprascapular nerve.
- Post-surgical complications after open or arthroscopic shoulder surgery can lead to suprascapular nerve damage.
- Scapula dyskinesia can give rise to suprascapular nerve palsy.
- Tumors, cysts & other space-occupying injuries around the shoulder can compress the suprascapular nerve.
- In rare cases, systemic conditions like systemic lupus erythematosus & rheumatoid arthritis can result in suprascapular nerve palsy
Clinical presentation
- normally, patients will present with dull aching pain over the superior or posterolateral aspect of the shoulder
- Pain might radiate down to the upper limb and to the neck.
- Cross-body adduction & internal rotation might increase pain.
- Pain will not be present if the nerve injury is distal to the area of the spinoglenoid notch.
- Almost 40% of cases present with related trauma to the shoulder.
- This is common in athletes involved in repeated and overhead activities.
- Patients with a history of injury can also report a sense of instability in the shoulder.
- The most common clinical sign of suprascapular nerve palsy includes
- atrophy of the supraspinatus &/or infraspinatus muscles.
- It is seen in 80% of cases.
- receivable to the anatomical course of the nerve, if the injury is proximal to the spinoglenoid notch, both muscles will be atrophied & if the injury is distal to the spinoglenoid notch, the supraspinatus is spared & only the infraspinatus will present with atrophy.
The “suprascapular nerve stretch test” is useful to resolve the involvement of the suprascapular nerve during physical examination. Here, the patient is asked to laterally rotate the head away from the affected shoulder & retract the neck. If the pain in the shoulder worsens with this maneuver, the test is positive.
Diagnosis
Nerve conduction studies & electromyography is examined to be the gold standard for the diagnosis of suprascapular nerve palsy. Prolonged latency, decreased amplitude, fibrillation potentials, & positive sharp waves in the nerve conduction study are indicative of suprascapular nerve compression & denervation. X-rays can help exclude trauma to the surrounding bones. CT, MRI, & diagnostic ultrasound can help restrict the site of injury. quick pain relief following an aesthetic injection to either the suprascapular or supraglenoid notch can support the diagnosis.
Treatment
Medical
Non-steroidal anti-inflammatory drugs & anesthetic injections (nerve block) are used to conservatively manage the pain.
Surgical
Surgery is only examined in cases that show no improvement after 6-12 months of conservative management. Surgical decompression of the suprascapular nerve is conducted along with repair of the contributing shoulder pathology (if present).
Physiotherapy treatment
- Sports-specific activity moderation is advised for the overhead activities for the athletes to prevent repetitive trauma. A full range of motion should be maintained or sustained at the shoulder to prevent adhesive capsulitis. Posterior shoulder capsule stretching & strengthening of the rotator cuff & shoulder muscles is recommended.
- Physiotherapy is aimed at reducing or decreasing symptoms & restoring function. Treatment may include:
- Electrotherapy
- Stretching exercises
- Strengthening exercises
- The practice of functional movements
Dorsal scapular nerve
The dorsal Scapular Nerve is the branch of the brachial plexus, rising from the ventral ramus of the C5 root. It is a motor nerve that rises from the C5 root, and penetrates the middle scalene muscle, coursing deep to & supplying levator scapulae & the rhomboid muscles.
Emerging from the middle scalene, it passes posteriorly between the posterior scalene, levator scapulae, & the serratus posterior superior muscle. From this location, the Dorsal scapular nerve passes inferior & medial to the scapula, coursing anterior to the rhomboid minor & major. In this position, the Dorsal scapular nerve terminates by supplying the rhomboid major and minor on their anterior surfaces.
Function
It is a motor nerve that supplies 3 muscles for the upper back ( levator scapulae, rhomboid major, & minor). These muscles work dynamically & collectively & are known as periscapular stabilizing muscles.
Associated structure
The dorsal scapular artery (DSA) follows the DSN to provide blood to the trapezius, levator scapulae, & rhomboid muscles. The DSA commonly spirals around the DSN as it runs medial to the scapula & anterior to the rhomboid muscles.
Clinical relevance
Compression of the dorsal scapular nerve (DSN): It is a condition in which the dorsal scapular nerve entraps in the middle scalene muscle causing pain and stiffness in the shoulder girdle and limited end range motion, along with winging of the scapula. The most common source of Dorsal scapular nerve entrapment is a hypertrophied middle scalene muscle.
- Abnormal and/or reduced shoulder movement
- Pain around the lower neck, upper/mid back & shoulder region
- Winging of the shoulder blade (i.e. tilting of the scapular blade away from the rib cage)
- Difficulty with drawing shoulders backward & together
- Difficulty with raising the arm upwards to the full range
- The altered resting position of the shoulder blade on the injured side. because of the poor functioning of the rhomboid muscles, the shoulder blade may sit away from the spine compared to the non-affected side.
- Weakness of the affected shoulder muscles
- Stiffness in the neck/spine
Treatment
- Conservative management
- Conservative treatment focuses on reducing or reducing the secondary muscle tension & on improving posture. Non-pharmacological treatments like Transcutaneous electrical nerve stimulation (TENS) & acupuncture can be tried.
- Pharmacological treatment
- Anti-neuropathic drugs like tricyclic antidepressants & antiepileptics (gabapentin, pregabalin) can help to relieve the pain or symptoms.
FAQ
What happens if the dorsal scapular nerve is get damaged?
Patients with dorsal scapular nerve entrapment mainly complain of pain over the medial border side of the scapula. Patients may also experience interscapular pain, shoulder & arm pain, weakness of arm abduction, & winged scapula.
Which muscles can be weak because of a suprascapular nerve condition?
Injury to the nerve at the suprascapular notch causes weakness of both the supraspinatus & infraspinatus muscles, whereas injury at the spinoglenoid region affects only the infraspinatus muscle.
What causes scapular nerve pain?
Acute injury of the suprascapular nerve is frequently caused by direct trauma, such as fracture or dislocation of the shoulder. However, chronic lesions of this nerve occur from the repetitive microtrauma associated with forceful occupational and sports activities.
What happens if the suprascapular nerve is damaged?
A suprascapular nerve injury presents as an unclear shoulder pain with associated weakness in shoulder abduction & external rotation. Later, the muscles of the shoulder girdle supplied by the suprascapular nerve may become atrophied.
How long does a suprascapular nerve block last?
normally, the suprascapular nerve block lasts between 3-5 minutes.
How long does it take for the suprascapular nerve block to work?
The local anesthetic will wear off 12–18 hours following your procedure. The steroid will take approximately 48 hours to start working. During this time there might be a window of increased discomfort or pain.
What does suprascapular nerve pain feel like?
the most common complaint of suprascapular neuropathy is a burning pain that radiates to the affected arm, neck, or back. Other symptoms of suprascapular nerve entrapment include Shoulder pain & upper back discomfort. Pain that generally worsens with shoulder movement
What are the major functions of the scapular muscles?
Structure & Function
The scapula is an important bone in the function of the complex of the shoulder joint. It allows 6 various types of motion, which allow for full-functional upper extremity movement including protraction, retraction, elevation, depression, upward rotation, and downward rotation.


7 Comments