
Oral Submucous Fibrosis (OSMF)
What is an Oral Submucous Fibrosis?
- Oral submucous fibrosis is defined as the chronic, insidious disease affecting the oral cavity and sometimes pharynx, although occasionally preceded and/or associated with vesicle formation and is always associated with juxtaepithelial inflammatory reaction followed by fibro elastic changes in the lamina propria with epithelial atrophy leading to stiffness of oral cavity leading to trismus and inability to eat.
- Oral submucous fibrosis is a chronic debilitating and well-recognized potentially malignant condition associated with areca nut chewing, an ingredient of betel quid, and is prevalent in South Asian population. Pathogenesis is not yet established but is believed to be due to multifactorial causes; hence the treatment of oral submucous fibrosis postulates a major challenge for oral physicians.
Causes and Patho-Physiology
- The pathogenesis of the disease is not well established, but the cause of OSF is believed to be multi-factorial.
A number of factors may trigger the disease process by causing a juxtaepithelial inflammatory reaction in the oral mucosa. Factors include are areca nut chewing, ingestion of chilies, genetic and immunologic processes, nutritional deficiencies, and other factors. - Areca Nut (Betel Nut) Chewing:
- The areca nut component of betel quid plays a major role in the pathogenesis of OSF 15. Betel nut is frequently used as a psychotropic and antihelminthic agent and used as an after-meal digestant which is taken to ease abdominal discomfort.
- Smoking and alcohol consumption alone, habits common to areca nut chewers, have been found to have no effect on the development of OSF. The strongest evidence regarding the etiology of OSF is the habit of areca nut chewing.
- Areca nut form may be available in the following form:
- Supari + Tobacco
- Supari + Pan+ Tobacco
- Supari + Pan + Pan masala
- Pan Parag / Pan masala
- Supari + Pan + Lime
- Supari- Roasted / Raw Areca nut
- Role of areca nut in pathogenesis of OSF:
- Arecoline, is an active alkaloid found in betel nuts. Stimulates fibroblasts to increase the production of collagen by 150%.
- To elevate the mRNA and protein expression of cystatin C, a nonglycosylated basic protein consistently up-regulated the variety of fibrotic diseases, in a dose-dependent manner in persons with OSF.
- Areca nuts have also been shown to have a high copper content, and chewing areca nuts for 5-30 minutes significantly increases soluble copper levels in oral fluids. This increased level of soluble copper supports the hypothesis as an initiating factor in individuals with OSF.
- Nutritional Deficiencies:
- Iron deficiency anemia, vitamin B complex deficiency, and malnutrition are promoting factors that derange the repair of the inflamed oral mucosa, leading to defective healing and resultant scarring.
- The resultant atrophic oral mucosa is more susceptible to the effects of chilies and betel nuts. Mucosal changes are similar to those in vitamin B and iron deficiency are seen in oral sub-mucosal fibrosis.
- Chillies:
- The role of chillies ingestion in the pathogenesis of OSF is controversial.
- A hypersensitivity reaction to chilies is believed to contribute to OSF.
- Genetic and Immunologic Processes:
- A genetic component is assumed to be involved in OSF Patients with increased frequency of HLA-A10, HLA-B7, and HLA-DR3.
Stages Oral Submucous Fibrosis (OSF):
- Stage 1:
- Stomatitis includes erythematous mucosa, vesicles, mucosal ulcers, melanotic mucosal pigmentation, and mucosal petechia.
- Stage 2:
- Fibrosis occurs in ruptured vesicles and ulcers when they heal, which is the hallmark of this stage.
Early lesions demonstrate blanching of the oral mucosa. - Older lesions include vertical and circular palpable fibrous bands in the buccal mucosa and around the mouth opening or lips, resulting in a mottled, marble-like appearance of the mucosa because of the vertical, thick, fibrous bands running in a blanching mucosa. Specific findings include the following:
- Reduction of the mouth opening (trismus).
- Stiff and small tongue.
- Blanched and leathery floor of the mouth.
- Fibrotic and depigmented gingiva.
- Rubbery soft palate with decreased mobility.
- Blanched and atrophic tonsils.
- Shrunken budlike uvula.
- Sinking of the cheeks, is not commensurate with age or nutritional status.
- Stage 3:
- Squeal of OSF are as follows:
- Leukoplakia is precancerous and is found in more than 25% of individuals with OSF.
- Speech and hearing deficits may occur because of the involvement of the tongue and the eustachian tubes.
Which SYMPTOMS Seen in Oral Submucuous Fibrosis?
- Xerostomia.
- Recurrent ulceration.
- Pain in the ear or deafness.
- Nasal intonation of voice.
- Restriction of the movement of the soft palate.
- Thinning and stiffening of the lips.
- Pigmentation of the oral mucosa.
- Dryness of the mouth and burning sensation.
- Decreased mouth opening and tongue protrusion.
Which are the CAUSES of Oral Submucuous Fibrosis?
- Immunological diseases.
- Extreme climatic conditions.
- Prolonged deficiency to iron and vitamins in the diet.
DIFFERENTIAL DIAGNOSIS:
- Oral manifestations of scleroderma
- Oral manifestations of Plummer Vinson syndrome (Iron deficiency Anemia).
INVESTIGATION:
- Complete Hemogram
- Toludine blue test
- Biopsy :- Incisional biopsy
- Immunofluorescent test:
a) Direct b) Indirect
Treatment and Prevention
- The treatment of patients with OSF depends on the degree of clinical involvement. If the disease is detected at a very early stage, cessation of the habit is sufficient. Most patients with OSMF present with moderateto- severe staging. Moderate-to-severe staging of OSF is irreversible. Medical treatment is symptomatic and aimed at improving mouth movements.
- Not to consume areca nut & other chronic irritant such as hot and spicy food including chiles.
- Advice green leafy vegetables.
- Administration of Vit. A, B complex & high protein diet.
- Administration of Antoxid OD for 6 – 8 weeks.
- Administration of Lycored OD for 6-8 weeks.
- Maintaining proper oral hygiene.
- Supplementing the diet with foods rich in vitamins A, B complex, and C and iron.
- Forgoing hot fluids like tea, coffee.
- Forgoing alcohol.
- Employing a dental surgeon to round off sharp teeth and extract third molars.
SURGICAL MANAGEMENT:
- Surgical treatment is indicated in patients with severe conditions. These include:-
- Simple excision of the fibrous bands: Excision can result in contracture of the tissue and exacerbation of the condition.
- Split-thickness skin grafting following bilateral temporalis myotomy or coronoidectomy: Trismus associated with OSF may be due to changes in the temporalis tendon secondary to OSF; therefore, skin grafts may relieve.
- Nasolabial flaps and lingual pedicle flaps: Surgery performed only in patients with OSF in whom the tongue is not involved.
Physiotherapy Treatment in Oral Submucuous Fibrosis
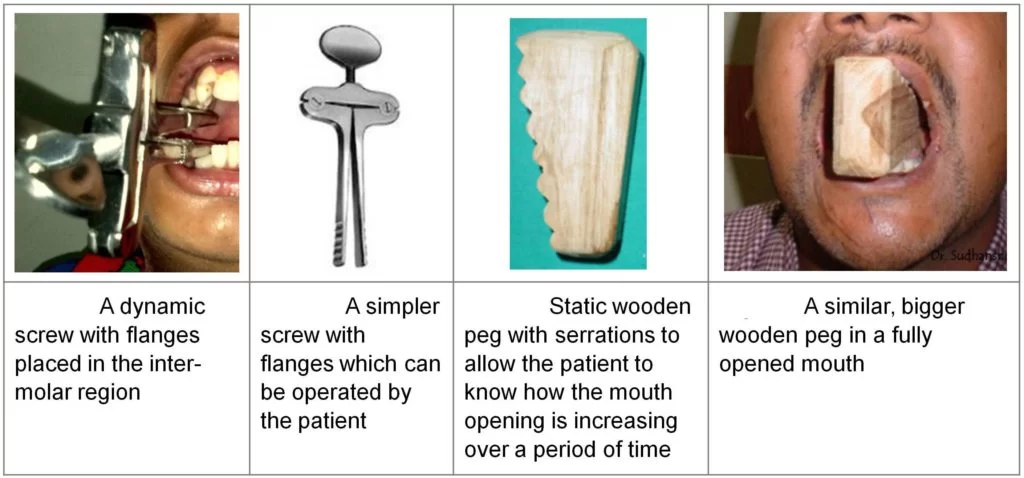
- Muscle stretching exercises for the mouth may be helpful to prevent further limitations of mouth opening forceful mouth opening has been tried with a mouth gag and acyclic surgical screw.
- Mouth-opening devices are also used to gradually open the mouth.
- Ice cream sticks are also used to open the mouth. First day you have insert spoon in mouth with maximum number of spoon and gradually increase the spoon as your mouth are opened.
- Diathermy: Microwave diathermy seem superior to short wave, because selective heating of juxtaepitheliel connective tissue is possible it acts by physio fibrinolysis of bands.
- Ultrasound: Ultrasound selectivity raises the temperature in some well-accumulated areas. Ultrasound proves to be an efficient deep heating modality.
Latest Research
Researchers have demonstrated that injecting autologous bone marrow stem cells intralesionally is a secure and successful therapeutic option for oral submucosal fibrosis. It has been demonstrated that injecting autologous bone marrow stem cells causes angiogenesis in the lesion location, which reduces the degree of fibrosis and causes a noticeable increase in mouth opening.
History
T. Sheikh first used the name distrophica idiopathica mucosa oris in 1952 to characterize a disease that causes oral fibrosis that he found in five Indian women living in Kenya. In 1953, S. G. Joshi came up with the name oral submucous fibrosis (OSF) to describe the condition.
FAQs
What causes oral submucous fibrosis?
Chewing areca nuts appears to be linked to the disorder, and the 5A genotype of the matrix metalloproteinase 3 (MMP3) promoter is linked to an increased risk of OSMF. Even in the absence of submucous fibrosis, iron-deficiency anaemia is not unusual in Asians.
Can oral submucous fibrosis be cured?
The patient’s oral cavity is impacted by OSMF. Even though OSMF patients have a significant death rate, the condition is treatable. Early detection and treatment can both cure oral submicrofibrosis and save the patient’s life.
How do you treat submucosal fibrosis?
In instances of increasing fibrosis, surgical intervention is advised when the interincisor distance falls below 2 centimetres (0.79 in). (Multiple release incisions made deep into the mucosa, submucosa, and fibrotic tissue; the gap or dehiscence thus formed is sutured using a tongue-derived mucosal graft and Z-plasty.
Can OSMF be stopped?
The course of treatment for OSMF is determined by the clinical involvement and rate of disease development. Early on, dietary supplements and habit cessation are carried out. In moderate levels, medicinal therapy is used in addition to conservative measures such intralesional injections.
Is OSMF a cancerous disease?
A chronic, sneaky premalignant condition with a high probability of malignancy, oral submucous fibrosis (OSMF) causes severe functional impairment. Originating from OSMF, oral squamous cell carcinomas (OSCC) are frequently highly aggressive, metastatic, and well-differentiated.
References
Oral submucous fibrosis. (2023, October 6). In Wikipedia. https://en.wikipedia.org/wiki/Oral_submucous_fibrosis
Author: Nitesh Patel - Physiotherapist
Physiotherapist in Samarpan Physiotherapy Clinic Ahmedabad Bapunagar Amaraiwadi Vastral Mobile Physiotherapy Clinic Dr. Nitesh Patel ( Physiotherapist ) : Mo No : 09898607803





Muh nahi khukta, khana khane me problem hoti he or garam-tikha nahi kha sakta , gal chipat gaye he
Contact us for Exercise