Pain management with interferential current therapy

- The basic principle of Interferential Therapy (IFT) is to utilise the significant physiological effects of low frequency (<250pps) electrical stimulation of nerves without the associated painful and somewhat unpleasant side effects sometimes associated with low-frequency stimulation.
- To produce low-frequency effects at sufficient intensity and at sufficient depth, patients can experience considerable discomfort in the superficial tissues (i.e. the skin).
- This is due to the impedance of the skin being inversely proportional to the frequency of the stimulation.
- [The barrier presented by the skin to the passage of an electric current is more complex than just impedance, or resistance, but will be regarded as such for the purpose of this explanation] In other words, the lower the stimulation frequency, the greater the impedance to the passage of the current & so, more discomfort is experienced as the current is ‘pushed’ into the tissues against this barrier.
- The effects of tissue stimulation with these ‘medium frequency’ currents (medium frequency in electromedical terms is usually considered to be 1KHz-100KHz) has yet to be established.
- It is unlikely to do nothing at all, but in terms of current practice, little is known of its physiological effects. It is not capable of direct stimulation of a nerve in the common context of such stimulation, though some researchers are currently investigating this area.
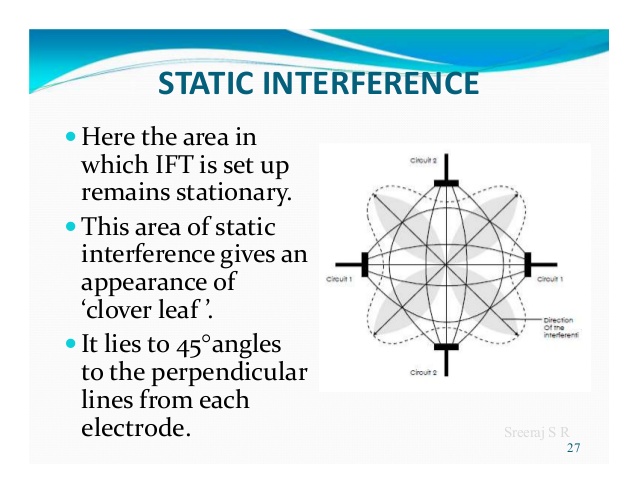
- Interferential therapy utilises two of these medium frequency currents, passed through the tissues simultaneously, where they are set up so that their paths cross & they literally interfere with each other – hence another term that has been used in the past but appears to be out of favour at the moment – Interference Current Therapy.
- This interaction gives rise to an interference current (or beat frequency) which has the characteristics of low-frequency stimulation – in effect, the interference mimics a low-frequency stimulation.
- The exact frequency of the resultant beat frequency can be controlled by the input frequencies. If for example, one current was at 4000Hz and its companion current at 3900Hz, the resultant beat frequency would be at 100Hz, carried on a medium frequency 3950Hz amplitude modulated current.
- By careful manipulation of the input currents, it is possible to achieve any beat frequency that you might wish to use clinically. Modern machines usually offer frequencies of 1-150Hz, though some offer a choice of up to 250Hz or more.
Frequency Sweep
- Nerves will accommodate to a constant signal & a sweep (or gradually changing frequency) is often used to overcome this problem.
- The principle of using the sweep is that the machine is set to automatically vary the effective stimulation frequency using either pre-set or user-set sweep ranges. The sweep range employed should be appropriate to the desired physiological effects (see below).
- It has been repeatedly demonstrated that ‘wide’ sweep ranges are ineffective whenever they have been tested or evaluated in the clinical environment are needs to be taken when setting the sweep on a machine in that with some devices, the user sets the actual base and top frequencies (e.g. 10 and 25Hz) and with other machines, the user sets the base frequency and then how much needs to be added for the sweep (e.g. 10 and 15Hz). Knowing which was round your machine works is critical to effective treatment.
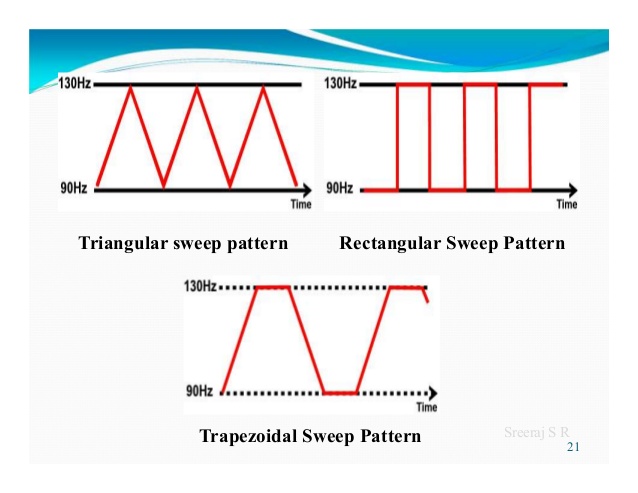
- The pattern of the sweep makes a significant difference to the stimulation received by the patient. Most machines offer several sweep patterns, though there is very limited ‘evidence’ to justify some of these options.
- In the classic ‘triangular’ sweep pattern, the machine gradually changes from the base to the top frequency, usually over a time period of 6 seconds – though some machines offer 1 or 3-second options.
- In the example illustrated, the machine is set to sweep from 90 to 130Hz employing a triangular sweep pattern. All frequencies between the base and top frequencies are delivered in equal proportion.
- Other patterns of sweep can be produced on many machines, for example, a rectangular (or step) sweep. This produces a very different stimulation pattern in that the base and top frequencies are set, but the machine then ‘switches’ between these two specific frequencies rather than gradually changing from one to the other.
Physiological Effects & Clinical Applications
- It has been suggested that IFT works in a ‘special way’ because it is ‘interferential’ as opposed to ‘normal’ stimulation. The evidence for this special effect is lacking and it is most likely that IFT is just another means by which peripheral nerves can be stimulated.
- It is rather a generic means of stimulation – the machine can be set up to act more like a TENS type device or can be set up to behave more like a muscle stimulator – by adjusting the stimulating (beat) frequency.
- It is often regarded (by patients) to be more acceptable as it generates less discomfort than some other forms of electrical stimulation.
- The clinical application of IFT therapy is based on peripheral nerve stimulation (frequency) data, though it is important to note that much of this information has been generated from research with other modalities, and its transfer to IFT is assumed rather than proven. There is a lack of IFT specific research compared with other modalities (e.g. TENS).
- Selection of a wide frequency sweeps has been considered less efficient than a smaller selective range in that by treating with a frequency range of say 1-100Hz, the effective treatment frequencies can be covered, but only for a relatively small percentage of the total treatment time. Additionally, some parts of the range might be counterproductive for the primary aims of the treatment.
Clinical Application
There are 4 main clinical applications for which IFT appears to be used:
- Pain relief
- Muscle stimulation
- Increased local blood flow
- Reduction of oedema
- In addition, claims are made for its role in stimulating healing and repair and for various specialised application – e.g. stress incontinence, though for the former examples (healing and repair) there is a dearth of quality research information available.
- As IFT acts primarily on the excitable (nerve) tissues, the strongest effects are likely to be those which are a direct result of such stimulation (i.e. pain relief and muscle stimulation). The other effects are more likely to be secondary consequences of these.
Pain Relief:
- Electrical stimulation for pain relief has widespread clinical use, thought the direct research evidence for the use of IFT in this role is limited. Logically one could use the higher frequencies (90-130Hz) to stimulate the pain gate mechanisms & thereby mask the pain symptoms.
- Alternatively, stimulation with lower frequencies (2-5Hz) can be used to activate the opioid mechanisms, again providing a degree of relief. These two different modes of action can be explained physiologically & will have different latent periods & varying duration of effect.
- It remains possible that relief of pain may be achieved by stimulation of the reticular formation at frequencies of 10-25Hz or by blocking C fibre transmission at >50Hz.
- Although both of these latter mechanisms have been proposed (theoretically) with IFT, neither have been categorically demonstrated.
Muscle Stimulation:
- Stimulation of the motor nerves can be achieved with a wide range of frequencies. Clearly, stimulation at low frequency (e.g. 1Hz) will result in a series of twitches, whist stimulation at 50Hz will result in a tetanic contraction.
- There is limited evidence at present for the ‘strengthening’ effect of IFT (though this evidence exists for some other forms of electrical stimulation), though the paper by Bircan et al (2002) suggests that it might be a possibility.
- On the basis of the current evidence, the contraction brought about by IFT is no ‘better’ than would be achieved by active exercise, though there are clinical circumstances where assisted contraction is beneficial. For example to assist the patient to appreciate the muscle work required (similar to surged Faradism used previously – but much less uncomfortable).
- For patients who can not generate useful voluntary contraction, IFT may be beneficial as it would be for those who, for whatever reason, find active exercise difficult. There is no evidence that has demonstrated a significant benefit of IFT over active exercise.
- Bellew et al (2012) evaluated the stimulatory effects of IFT and various Burst Mode currents in terms of their capacity to generate significant-quality muscle contraction, the results were supportive of IFT as a treatment option.
- The choice of treatment parameters will depend on the desired effect. The most effective motor nerve stimulation range with IFT appears to lie between approximately 10 and 20, maybe 10 and 25Hz. Stimulation below 10Hz results in a series of coarse twitches which may be of clinical benefit, though it has yet to be unequivocally demonstrated with IFT.
- Stimulation at higher frequencies than that needed to bring about partial tetany (usually around 20 or 25Hz) can generate a strong tetanic contraction, which might be considered beneficial to assist patient appreciation of the required muscle work, but again, in terms of IFT intervention, it has yet to be demonstrated that this contraction level is needed over and above partial tetany.
- Caution should be exercised when employing IFT as a means to generate clinical levels of muscle contraction in that the muscle will continue to work for the duration of the stimulation period (assuming sufficient current strength is applied).
- It is possible to continue to stimulate the muscle beyond its point of fatigue – the contractions are forced via the motor nerve – and short stimulation periods with adequate rest might be a preferable option.
- Some IFT devices are capable of generating a ‘surged’ stimulation mode which might be advantageous in that fatigue would be minimised – this surged intervention would be similar, but more comfortable than Faradism.
Blood flow
- There is very little if any quality evidence demonstrating a direct effect if IFT on local blood flow changes. Most of the work that has been done involves laboratory experimentation on asymptomatic subjects, and most blood flow measurements are superficial i.e. skin blood flow.
- Whether IFT is actually capable of generating a change (increase) in blood flow at depth remains questionable. The elegant experimentation by Noble et al (2000) demonstrated vascular changes at 10–20Hz, though was unable to clearly identify the mechanism for this change.
- The stimulation was applied via suction electrodes, and the outcome could therefore be as a result of the suction rather than the stimulation, though this is largely negated by virtue of the fact that other stimulation frequencies were also delivered with the suction electrodes without the blood flow changes.
- The most likely mechanism is via muscle stimulation effects (IFT causing muscle contraction which brings about a local metabolic and thus vascular change). The possibility that the IFT is acting as an inhibitor or sympathetic activity remains a theoretical possibility rather than an established mechanism.
- Based on currently available evidence, the most likely option for IFT use as a means to increase local blood flow remains via the muscle stimulation mode, and thus the 10-20 or 10-25Hz frequency sweep options appears to be the most likely beneficial option.
Oedema
- IFT has been claimed to be effective as a treatment to promote the reabsorption of oedema in the tissues. Again, the evidence is very limited in this respect and the physiological mechanism by which could be achieved as a direct effect of the IFT remains to be established.
- The preferable clinical option in the light of the available evidence is to use the IFT to bring about local muscle contraction(s) which combined with the local vascular changes that will result could be effective in encouraging the reabsorption of tissue fluid. The use of suction electrodes may be beneficial but also remains unproven in this respect.
- A study demonstrated a change in oedema following knee surgery in an IFT group, though the patients did the circumferential knee measures (rather than the therapist) and circumferential knee measurement is not an especially reliable method for identifying oedema as such. The Christie and Willoughby study (1990) failed to demonstrate a significant benefit on ankle oedema following fracture and surgery.
- The treatment parameters employed are unlikely to be effective given the information now available. If IFT has a capacity to influence oedema, the current evidence and physiological knowledge would suggest that a combination of pain relief (allowing more movement), muscle stimulation (above) and enhanced local blood flow (above) is the most likely combination to be most effective.
treatment Parameters:
- Stimulation can be applied using pad electrodes and sponge covers (which when wet provide a reasonable conductive path), though the electro-conductive gel is an effective alternative.
- The sponges should be thoroughly wet to ensure even current distribution.
- Self-adhesive pad electrodes are also available (similar to the newer TENS electrodes) and make the IFT application easier in the view of many practitioners.
- The suction electrode application method has been in use for several years, and whilst it is useful, especially for larger body areas like the shoulder girdle, trunk, hip, knee, it does not appear to provide any therapeutic advantage over pad electrodes (in other words, the suction component of the treatment does not appear to have a measurable therapeutic effect).
- Care should be taken with regards maintenance of electrodes, electrode covers and associated infection risks.
- IFT pad electrodes IFT adhesive electrodes
- Whichever electrode system is employed, electrode positioning should ensure adequate coverage of the area for stimulation.
- Using larger electrodes will minimise patient discomfort whilst small, closely spaced electrodes increase the risk of superficial tissue irritation and possible damage/skin burn.
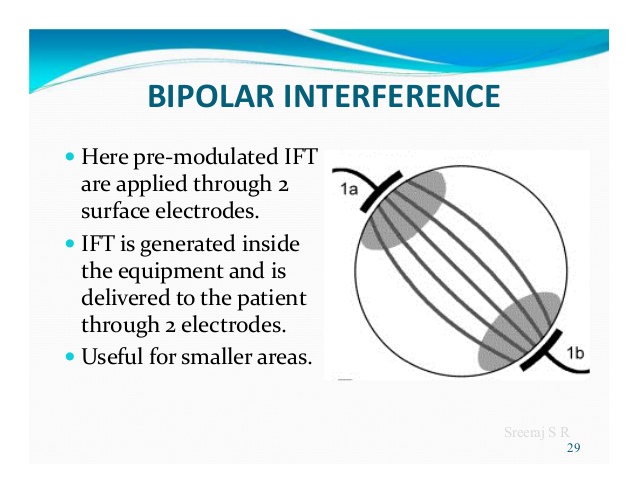
- The bipolar (2 poles) application method is perfectly acceptable, and there is no physiological difference in treatment outcome despite several anecdotal stories to the contrary. Recent research evidence supports the benefit of 2 pole application.
- Treatment times vary widely according to the usual clinical parameters of acute/chronic conditions & the type of physiological effect desired. In acute conditions, shorter treatment times of 5-10 minutes may be sufficient to achieve the effect.
- In other circumstances, it may be necessary to stimulate the tissues for 20-30 minutes. It is suggested that short treatment times are initially adopted especially with the acute case in case of symptom exacerbation.
- These can be progressed if the aim has not been achieved and no untoward side effects have been produced. There is no research evidence to support the continuous progression of a treatment dose in order to increase or maintain its effect.
other related articles:


Author: Bhoomi Physiotherapist
Bhoomi Patel - Physiotherapist in Mobile Physiotheray Clinic, B - 01, Jagatnagar Society, Opp. Shaktidhara Society, India Colony Road, Tollnaka, Bapunagar, Ahmedabad.