
Serratus anterior myofascial pain syndrome:
What is Serratus anterior myofascial pain syndrome?
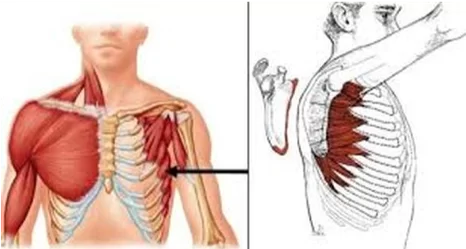
Serratus anterior myofascial pain syndrome is a condition that is characterized by pain and discomfort in the serratus anterior muscle, which is located on the side of the ribcage. This muscle is responsible for stabilizing the scapula (shoulder blade) and aiding in the movements of the arm and shoulder.
The pain associated with this syndrome is typically described as a dull ache that is located in the upper chest, under the armpit, and/or along the side of the ribcage. The pain may also radiate down the arm, causing weakness and a limited range of motion.
Serratus anterior myofascial pain syndrome is often caused by overuse or strain of the serratus anterior muscle. Poor posture, heavy lifting, repetitive movements, and sports activities that involve throwing or swinging motions are common contributing factors. In some cases, the condition may be related to underlying medical conditions, such as thoracic outlet syndrome or scapular dyskinesis.
Treatment for serratus anterior myofascial pain syndrome typically involves a combination of physical therapy, stretching exercises, and pain management techniques such as massage, heat therapy, and medication. In severe cases, surgery may be necessary to relieve pressure on the affected muscle. It is important to consult with a healthcare provider for proper diagnosis and treatment of this condition.
Myofascial pain syndromes are very common, yet there are no universally recognized diagnostic criteria for them. Pain that is felt above the fifth to seventh ribs at the midaxillary line and spreads to the shoulder is the most typical sign of serratus anterior myofascial pain syndrome. anterior chest wall, the medial aspect of the arm, the medial border of the scapula, and on rare occasions towards the fourth and fifth digits mimicking radiculopathy. As it was in our patient, who underwent unsuccessful shoulder surgery due to shoulder impingement syndrome, this syndrome is sometimes mistaken for persistent mechanical neck discomfort, glenohumeral instability, and shoulder impingement syndrome.
Patients who are suspected of having myofascial pain are first evaluated physically and given a complete medical history. Patients frequently describe symptoms as having lingering pain in a specific area that limits the use of a target muscle group. Inciting circumstances can be as blatant as prior trauma or damage or as subtle as a minor posture flaw. Imaging studies can identify related anatomic processes, such as deteriorating joints or connective tissue, in the body.
What causes serratus anterior pain?
- Tension
- Stress
- Overuse
- Minor injuries
- Slipped or broken rib
- Pleurisy
- Ankylosing spondylitis is a spinal form of arthritis.
- Asthma
What are the symptoms of serratus anterior pain?
- Arm or finger pain
- Difficulty with deep breathing
- Sensitivity
- Tightness
- Pain in the chest or breasts
- Shoulder blade pain
- Deep, aching pain in a muscle
- Pain that persists or worsens
- A tender knot in a muscle
- Difficulty sleeping due to pain
When should someone experiencing serratus anterior pain visit a doctor?
- Difficulty breathing
- Dizziness
- High fever with a stiff neck
- A tick bite or bull’s-eye rash muscle aches following the initiation of a new drug or an increase in dosage of an already-taken prescription
- Back or chest pain that is becoming worse yet doesn’t get better with rest
- Pain that keeps you from sleeping or performing your normal tasks
Risk factors of serratus anterior pain?
- Muscle injury
- Stress and anxiety
Muscle pain:
Continuing muscle stress or a recent muscle injury can both cause trigger points to develop. A region within or close to a strained muscle, for instance, could develop into a trigger point. Poor posture and repetitive actions might also raise your risk.
Stress and anxiety:
Trigger points in the muscles may be more likely to form in those who feel stress and anxiety often. According to one idea, these persons may clench their muscles more frequently, which is a repetitive tension that makes muscles more prone to trigger points.
Complication of serratus anterior myofascial pain:
- Sleep problems
- Fibromyalgia
Sleep problems:
Myofascial pain syndrome symptoms and signs can make it difficult to fall asleep at night. Finding a comfortable sleeping position could be challenging. Additionally, if you walk at night, you can encounter a trigger and wake up.
Fibromyalgia:
According to certain studies, some persons with myofascial pain syndrome may go on to develop fibromyalgia. Chronic fibromyalgia is characterized by widespread pain. Over time, it’s thought that fibromyalgia patients’ brains become more sensitive to pain signals. Some medical professionals think that this process may be triggered by myofascial pain syndrome.
Anatomy of serratus anterior myofascial:
Origin of serratus anterior:
The eight or nine upper ribs’ top lateral surface is where it starts. Once it has wrapped posteromedially around the ribcage, it inserts on the medial edge of the scapula’s underside.
Tendinous septa separate the muscle into nine finger-like clusters of muscle fibers called digitations as it extends from the ribs.
By slanting between these septa, the fibers create a multipennate muscular architecture.
The inferior fibers are the lower six digitations, and the superior fibers are the upper three digitations. The lower four digitations of the serratus anterior and the external oblique’s fibers interdigitate.
The eight or nine upper ribs’ top lateral surface is where it starts. After coiling posteromedially across the ribs, it inserts on the medial scapular line by sliding beneath the scapula.
Tendinous septa separate the muscle as it spreads from the ribs into nine finger-like bundles of muscle fibers known as “digitations.”
To varied degrees, the fibers obliquely pass through these septa to create the multipennate muscle architecture. The inferior fibers are the lower six digitations, and the superior fibers are the upper three digitations. The lower four digitations of the serratus anterior and the external oblique’s fibers interdigitate.
Insertion:
- Upper/superior: superior angle of the scapula and first to second ribs.
- Middle/Intermedius: Medial scapular border and second to third ribs.
- Lower/Inferior: medial border of the fourth to ninth ribs, and inferior angle of the scapula. It is the most potent and noticeable component.
Nerve and Blood Supply:
- The C5 to C7 brachial plexus nerve roots give rise to the long thoracic nerve.
- thoracodorsal artery, superior thoracic artery, and lateral thoracic artery.
Function:
The scapulothoracic joint’s principal movements are protraction and upward rotation. Additionally, it serves as a vital scapular stabilizer by maintaining the shoulder blades close to the rib cage both at rest and during movement. Additionally, it cooperates with the upper and lower trapezius fibers to maintain the scapula’s upward rotation, which permits overhead arm movement. See Scapulohumeral Rhythm and Dynamic Stabilisers of the Shoulder Complex.
The accessory inspiratory muscles are recruited when the shoulder blade is in a fixed position, such as after a boxing match or in a person with emphysema. The serratus anterior supports respiration by lifting the ribcage.[6]The sternocleidomastoid, scalene muscles, pectoralis major, pectoralis minor, trapezius, latissimus dorsi, erector spine, iliocostalis lumborum, and quadratus lumborum are among the other auxiliary inspiratory muscles.
The serratus anterior, sometimes referred to as the “boxer’s muscle,” is largely to blame for the protraction of the scapula that happens after delivering a punch. The accessory inspiratory muscles contract while the shoulder blade is secured in place.
Palpation:
The side of the ribcage is covered by the paper-thin serratus anterior muscle. The primary portion of the serratus anterior is plainly palpable between the pectoralis major and latissimus dorsi muscles, deep to the scapula and pectoral muscles.
Between the latissimus dorsi and pectoralis major muscles, SA saw her. Placing your hand just below the armpit will allow you to feel it. Additionally, getting a sense of how your ribs feel will help you differentiate between the ribs and this thin, superficial muscle.
Treatment of Serratus anterior myofascial pain syndrome:
All workouts for the anterior deltoid indirectly train the serratus anterior. In the limited chest workouts that include scapular protraction, it functions somewhat. Several instances include
- Plank and straight-arm plank are two isometric exercises.
incline your shoulders up
raised flat shoulders - In the air shrug
Push-ups plus a punch to the serratus anterior
When you feel discomfort in your muscles while engaging in an activity, a pulled muscle is usually the cause. In these circumstances, a modified version of RICE is advised.
Rest: Go slowly in your normal routines and attempt to give the muscle as much time to recover as you can.
Ice: Several times a day, apply an ice pack to the aching area of the muscle for 20 minutes at a time.
Compression: It could be challenging to squeeze the serratus anterior. To help minimize swelling, you can experiment with wearing tighter clothing or bandaging the affected area.
Elevation: The serratus anterior is an exception.
Nonsteroidal anti-inflammatory medications, such as aspirin or ibuprofen, can occasionally help with pain relief and swelling reduction. Make sure these medications are safe for you by seeing your doctor.
You can also try these exercises, warm compresses, and massages to help your muscles relax. Consult your doctor if remedies you can do at home don’t work. Your doctor may prescribe medication based on the severity of your wounds and what they discover during the examination.
- oral steroids
- muscle relaxers
- stronger pain medication
- joint injections
Physiotherapy Treatment of Serratus Anterior Myofascial pain syndrome
Physiotherapy can be an effective treatment approach for Serratus anterior myofascial pain syndrome. The following are some of the physiotherapy treatment options that may be used:
- Soft tissue mobilization: This technique involves manual manipulation of the affected muscle tissue to relieve tension and promote healing.
- Stretching exercises: Gentle stretching of the serratus anterior muscle and surrounding muscles can help improve range of motion and reduce pain.
- Strengthening exercises: Specific exercises designed to strengthen the serratus anterior muscle can help improve its function and reduce the risk of further injury.
- Postural re-education: Poor posture can contribute to the development of Serratus anterior myofascial pain syndrome. A physiotherapist can teach you, proper body mechanics, to prevent further injury.
- Modalities: Heat therapy, ice therapy, and electrical stimulation may also be used to relieve pain and promote healing.
- Education: A physiotherapist can educate you on how to modify your daily activities to avoid aggravating the condition and to prevent recurrence.
It is important to note that the treatment plan for Serratus anterior myofascial pain syndrome will vary depending on the severity and underlying cause of the condition. A physiotherapist can provide an individualized treatment plan tailored to your specific needs.
Summary:
Pain that occasionally travels to the fourth and fifth digits, the medial aspect of the arm, the medial border of the scapula, and the anterior chest wall s radiculopathy mimics and is a common symptom of serratus anterior myofascial pain syndrome. Myofascial pain syndromes, which encompass a variety of disorders, include serratus anterior myofascial pain syndrome. In the process of myofascial pain, localized trigger points develop and remain, causing pain and dysfunction. According to estimates, myofascial pain accounts for around 30% of visits to general practitioners, 21% to orthopedic surgeons, and 85-73% to pain management specialists.
Patients who are suspected of having myofascial pain are first evaluated physically and given a complete medical history. Patients frequently describe symptoms as having lingering pain in a specific area that limits the use of a target muscle group. Inciting circumstances can be as blatant as prior trauma or damage or as subtle as a minor posture flaw. Imaging studies can identify related anatomic processes, such as deteriorating joints or connective tissue, in the body.
FAQ:
What does serratus anterior pain feel like?
When reaching or holding your arm overhead, you may experience shoulder or neck pain. trembling or weakness while performing bench or overhead pressing exercises in the gym. As you extend in front and overhead, your shoulders may click or squeak. the feeling of pins and needles or numbness from the hand down the arm.
How do you stop serratus anterior pain?
Rest. Take it easy on yourself throughout regular activities and try to give the muscle as much time to recover as you can.
Ice. Several times throughout the day, apply an ice pack that has been wrapped in a towel to the aching area of the muscle.
Compression.
Elevation.
What nerve is the weakness of the serratus anterior?
The long thoracic nerve is the only source of innervation for the serratus anterior muscle, also referred to as the “boxer’s muscle,” and when it is injured, the muscle paralyzes, a condition known as a winged scapula.
Where is serratus anterior pain felt?
A typical sign of serratus anterior myofascial pain syndrome is pain that radiates to the anterior chest wall, the medial aspect of the arm, the medial border of the scapula, and rarely towards the fourth and fifth digits. This pain mimics radiculopathy.
Can serratus cause shoulder pain?
The shoulder blade simply cannot move out of the way of the arm if the serratus is weak, which results in subacromial impingement syndrome, also known as subacromial bursitis, or pinching at the top of the shoulder. It may potentially eventually result in the development of a rotator cuff tear.
What nerve goes to the serratus anterior?
The serratus anterior muscle receives innervation from the long thoracic nerve, a motor neuron. This muscle lifts the ribs to aid in breathing and drags the scapula anteriorly to allow for arm anteversion.




2 Comments