Slipped Capital Femoral Epiphysis (SCFE)
What is Slipped Capital Femoral Epiphysis?
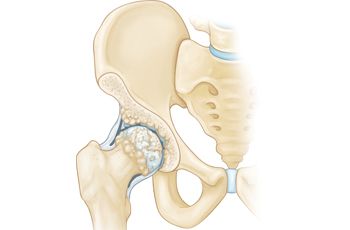
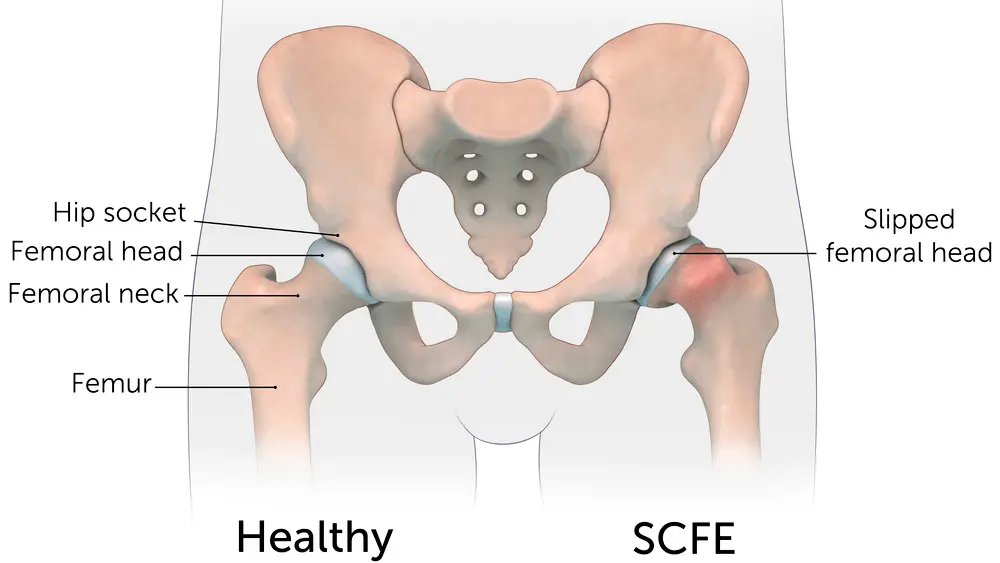
Slipped capital femoral epiphysis (SCFE) is a disease of adolescents in which the growth plate is injured and the femoral head moves (slips) to the rest of the femur. The head of the femur remains in the cup of the hip joint while the rest of the femur is moved.
Types of SCFE contain:
Stable SCFE. In stable Slipped Capital Femoral Epiphysis – SCFE, the patient can put weight on the involved hip, either with or without crutches. Most patients of Slipped Capital Femoral Epiphysis – SCFE are stable slips.
Unstable SCFE. This is a more extreme slip. The person cannot place weight on their hip, even with crutches. Unstable Slipped Capital Femoral Epiphysis – SCFE needs urgent therapy. Complications associated with Slipped Capital Femoral Epiphysis – SCFE are much more familiar in persons with unstable slips.
Slipped Capital Femoral Epiphysis – SCFE generally happens on only one side; yet, it can happen on the opposite side, as well. If so, this occurs within 18 months from the time of the initial attack.
Epidemiology
The majority of Slipped Capital Femoral Epiphysis – SCFE is 10.8 cases per 100 000 children. Slipped Capital Femoral Epiphysis – SCFE shows bilaterally in 18 to 50 percent of persons. The majority is more familiar in boys than girls and differs widely among ethnic groups (higher majority rate in Hispanics, blacks, Polynesians, and Native Americans ), geographic places (more elevated rates in the north and western regions of the United States), and various seasons (late summer and fall).
Even though the pathogenesis is most probably multi-factorial, mechanical factors (particularly obesity and growth surges/abnormal morphology of the proximal femur and acetabulum) appear to play a key part. Further factors that either decrease the resistance to shear or raise the stresses across the proximal femoral physis are endocrine diseases,
Several factors can contribute to evolving a Slipped Capital Femoral Epiphysis – SCFE:
- Obesity
- Femoral retroversion (>10)
- Increased physis height
- The more vertical slope of the physis
Metabolic and pathological conditions such as:
- Renal failure osteodystrophy
- Previous radiation therapy
Endocrine disorders such as:
- Hypothyroidism
- Growth hormone deficiency
- Growth hormone excess
- Panhypopituitarism
- Craniopharyngioma
- Hypogonadism
- Hyperparathyroidism
- Multiple endocrine neoplasias
- Turner’s syndrome
- Elevation of Leptin levels
Symptoms of Slipped Capital Femoral Epiphysis
Symptoms of Slipped Capital Femoral Epiphysis – SCFE differ, depending upon the severity of the disease.
A person with a stable Slipped Capital Femoral Epiphysis – SCFE:
- Will generally have an intermittent ache in the hip, groin, knee, and/or thigh for several weeks or months that generally worsens with movement
- May walk or run with a limp after a period of movement
- May maintain the involved side in a position of improved external rotation, resulting in an out-toed gait
In the more extreme unstable Slipped Capital Femoral Epiphysis – SCFE, in which the femoral head has moved abruptly, symptoms may contain:
- Sudden onset of ache, frequently after a fall or injury
- Incapability to put weight on the involved leg
- Outward turning (external rotation) of the involved leg
- A discrepancy in leg length the involved leg may seem shorter than the opposite leg
Differential Diagnosis
Further conditions to rule out:
- Femoral fractures
- Avascular Necrosis Femoral Head
- Legg-Calve-Perthes Disease
- Osteomyelitis
- Septic Arthritis
- Groin Strain
- Apophyseal avulsion fracture of the anterosuperior iliac spine and anteroinferior iliac spine
- Apophysitis of the anterosuperior iliac spine and anteroinferior iliac spine
- Transient synovitis
Doctor Examination
Physical Examination
During the test, your child’s doctor or physician will ask about your child’s general fitness and medical record. They will then speak with you about your kid’s symptoms and ask when the symptoms started.
While your kid is lying down, the doctor or physician will conduct a careful examination of the involved hip and leg, looking for:
Pain with extremes of movement
Limited range of movement in the hip particularly limited internal rotation
Involuntary muscle protection and muscle spasms are present to avoid painful action
The doctor or physician will also observe your kid’s gait (the way they walk). A kid with Slipped Capital Femoral Epiphysis – SCFE may limp or have an abnormal gait.
Drehmann sign. The Drehmann sign is positive if an unavoidable passive external rotation of the hip joints happens when conducting a hip flexion. In extra, an internal rotation of the respective hip joint or junction is either not possible or accompanied by pain when strongly induced. The positive Drehmann sign is a specific clinical characteristic in slipped capital femoral epiphysis (SCFE)
Lab test
X-rays
X-rays deliver images of dense structures, like bone. Your kid’s doctor or physician will order X-rays of the hip, pelvis, and thigh from two various angles to assist verify the diagnosis.
In a person with Slipped Capital Femoral Epiphysis – SCFE, an X-ray will indicate that the head of the femur seems to be slipping off the neck of the bone.
Degree of Deformity
Morphological categories have relied on radiographic pictures using the linear displacement of the femur head on the neck of the femur or the slip arch (arc between the shaft and opposite to the physis per Southwick) as parameters.
The degrees of deformity are:
- Pre-slip (widening of the physis, no displacement)
- Mild slip (up to 1/3 displacement, or 30 of femoral head tilt)
- Moderate slip (1/3 to 1/2 displacement or 30 to 60 slip angle)
- Severe slip (> 1/2 displacement or > 60 of slip angle)
Treatment of Slipped Capital Femoral Epiphysis
Medical treatment
Medications may contain nonsteroidal anti-inflammatory medications, acetaminophen, or narcotics, depending on the doctor’s or physician’s preference.
Surgical treatment
The purpose of treatment is to control the mildly displaced femoral head from slipping any added. This is always conducted via surgery.
Early diagnosis of Slipped Capital Femoral Epiphysis – SCFE delivers the best option for stabilizing the hip and avoiding complications. When treated early and properly, a long-term hip function can be predicted to be very good.
Once Slipped Capital Femoral Epiphysis – SCFE is verified, your kid will not be permitted to place weight on their hip and will likely be admitted to the hospital. In most patients, surgery is conducted within 24 to 48 hours.
Procedures
The surgical method your kid’s doctor or physician suggests will depend upon the severity of the slip. Methods used to manage Slipped Capital Femoral Epiphysis – SCFE contain:
In situ fixation. This is the method used most frequently for persons with stable or mild Slipped Capital Femoral Epiphysis – SCFE. The doctor or physician creates a small incision near the hip, then inserts a metal nail across the growth plate to hold the position of the femoral head and control any further slippage. Over time, the growth plate will close, or merge. Once the growth plate is locked, no further slippage can happen.
Open reduction. In persons with unstable Slipped Capital Femoral Epiphysis – SCFE, the doctor or physician may first create an open incision in the hip, then slightly manipulate (decrease) the head of the femur back into its usual anatomic position. The doctor or surgeon will then insert one or two metal nails to maintain the bone in the spot until the growth plate seals. This is a more extensive method and needs a longer healing time.
In situ fixation in the opposite hip. Some persons are at higher risk for Slipped Capital Femoral Epiphysis – SCFE happening on the opposite side. If this is the matter with your kid, the doctor or physician may suggest inserting a nail into the uninvolved hip at the same time to decrease the risk of Slipped Capital Femoral Epiphysis – SCFE. The doctor or surgeon will talk with you regarding whether this therapy is suitable for your kid.
Physiotherapy treatment in Slipped Capital Femoral Epiphysis
Physiotherapy treatment for a slipped upper femoral epiphysis is specific to each person but may include:
- Heat and ice treatment
- Range of motion exercises
- Strengthening exercises
- Education on walking aids and gait pattern
- Balance exercises
- Gradual return to function and sport-specific exercises/drills
Range of Movement Exercise
Range of motion exercises will be specified upon the result of a physiotherapy assessment. This review will glance at the range and the quality of the motion. Quite frequently strengthening exercises are specified alongside or shortly after a range of motion exercises as the increased motion at a joint or junction without increasing the strength could cause further damage. Range of motion exercise programs will contain:
Passive range of movement exercises – where another person or another body part finishes the full motion without muscle activation
Active-assisted range of movement exercises – where the muscles finish the motion within the available range and then further pressure is applied to complete a few extra degrees.
Gravity-assisted range of movement exercises – where the motion is done by muscle activation in a position where gravity can help to drag the weight of the limb to the end of the joints or junctions available range.
Range of motion exercises within the water can be recommended by the physiotherapist as warm water can assist to calm the tissues and raise the extensibility of the tissues raising the achievable range.
The range of motion exercises will be specified upon the result of the initial review and review of the result measure. Strengthening activities may also accompany a range of motion activities.
Strengthening exercise
Strengthening activities are activities that are planned to raise the muscle bulk of certain regions of the body and aim to raise the power which a muscle can produce. The most familiar form of strength training is resistance training. Resistance activities make use of opposing forces to raise the workload that muscles require to overcome to carry the part of the body. Instances of resistance exercises contain:
Weight training
Therabands
Advantages of Strengthening Exercises
There are many benefits of strengthening activities. The benefits will depend upon the precise requirements of your kid as to what they will gain from them. Some of the key benefits are listed following.
Increased independence
Increased strength
Increased expectoration
Increase aerobic capacity
Increased work capacity
Increased quality of life
Decreased need for carers
Better posture
Return to sports sooner
Return to school sooner
Better gait
Faster recovery from surgery
Balance exercise
Balance activity schedules are concentrating on challenging a patient’s balance to create the vestibular and musculoskeletal system. Balance activity programs will contain:
Exercises on various terrain
Exercises on various bases of support eg. one foot, on a wobble board
Exercises with no visual feedback
Exercises that are away from your base of support eg. reaching
Exercises that are out of your base of support whilst moving (dynamic activities)
These activities will be specified upon a comprehensive assessment and will be observed with an outcome measure. This will provide the physiotherapist and yourself with a measurement that will observe your progress.
Prognosis
The Loder type is important in prognosis. The original analysis in 1993 found that a person with Slipped Capital Femoral Epiphysis – SCFE classified as stable did not generate osteonecrosis, whereas 47% of the person with Slipped Capital Femoral Epiphysis – SCFE that were considered unstable went on to generate osteonecrosis. More recent analyses, involving a systematic study, have verified these results.
Complications of Slipped Capital Femoral Epiphysis
Complications of Slipped Capital Femoral Epiphysis – SCFE contain femoral growth arrest due to early closure of the physis, femoral head osteonecrosis,femoroacetabular impingement, chondrolysis, infection, labral tears, chronic pain, and growth of Slipped Capital Femoral Epiphysis – SCFE in the contralateral hip. After complications of Slipped Capital Femoral Epiphysis – SCFE contains early-onset osteoarthritis of the hip joint.
Femoral head osteonecrosis could result from the initial damage, with a more elevated risk in unstable Slipped Capital Femoral Epiphysis – SCFE patients. Also, it can evolve as a postoperative complication due to metalwork placement in the posterosuperior aspect of the femoral neck, where it poses a threat of disrupting the blood supply of the femoral neck.
Chondrolysis could be a result of articular surface penetration. Persons will generally present with aches and a decreased range of movement. Radiographs will demonstrate decreased joint or junction space, and a CT scan would be the best modality to evaluate metalwork penetration.
Femoroacetabular impingement is due to the defeat of proximal femoral remodeling (pistol grip malformation). This can be addressed, as mentioned before, by proximal femoral osteotomy.
Slip progression: This has been documented in 1 to 2% of patients with single screw fixation.
FAQ
Is SCFE more common in boys or girls?
Slipped Capital Femoral Epiphysis – SCFE has been defined as the most familiar hip disease of adolescent kids in the USA. Boys are more exposed than girls creating this disease. It is most frequently diagnosed in obese kids around puberty and kids with endocrinopathies or chronic systemic conditions.
How long is recovery for SCFE?
In general, expect that your kid will require crutches or a walker for up to approximately four weeks after surgery for stable Slipped Capital Femoral Epiphysis – SCFE and for at least six to eight weeks for unstable Slipped Capital Femoral Epiphysis – SCFE. Your kid will work with a physical therapist to assist to strengthen leg and hip muscles and enhance range of motion.
Is slipped capital femoral epiphysis a disability?
Slipped Capital Femoral Epiphysis – SCFE happens via the unfused growth plate of the proximal femur where the femoral head slips posteriorly on the femoral neck. Severe outcomes of the issue, like post-traumatic arthritis, gait disturbance, chondrolysis, and osteonecrosis of the femoral head can happen, leading to lifelong disability.
What is femoral epiphysis in a fetus?
The sonographic evaluation of distal femoral epiphysis/proximal tibial epiphysis can be used as separate features for the estimation of gestational age during the third trimester, a period in which standard fetal biometric assessments of gestational age are least correct.
Does SCFE lead to hip replacement?
It is known that persons with Slipped Capital Femoral Epiphysis – SCFE are probable to require total hip arthroplasty (THA) shortly, with 45% of Slipped Capital Femoral Epiphysis – SCFE persons requiring THA by age 50. These persons are thought to have accelerated joint or junction degeneration due to AVN, residual malformation, and chondrolysis.