Tests for leg length
- There are two – 2 types of leg length discrepancy.
- The first, called true leg length discrepancy or true shortening is caused by anatomic or structural changes in the lower leg resulting from congenital maldevelopments such as congenital hip dysplasia, bony abnormality, adolescent coxa vara, or trauma such as a fracture.
- Because an anatomic short leg results, the spine & pelvis are often affected leading to lateral pelvic tilt & scoliosis.
- The second type of leg length discrepancy is called functional leg length discrepancy or functional shorting,& it is the result of compensation for a change that may have occurred because of positioning rather than structure.
- For example, this discrepancy could occur because of unilateral foot pronation/spinal scoliosis.
True leg length:

- Before any measuring, the examiner must be set the pelvis square, level,/in balance with lower limbs.
- The leg should be 15 to 20 cm [ 4 to 8 inches]apart & parallel to each other.
- If the legs are not placed in proper relation to the pelvis, apparent shorting of the limb may occur.
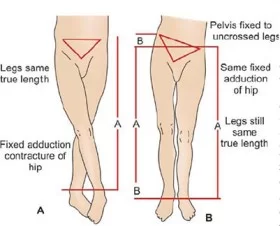
- The lower limbs are must be placed into comparable positions which are relative to the pelvis because abduction of the hip are brings the medial malleolus which is closer to the ASIS on the same side & adduction of the hip are take the medial malleolus farther from to ASIS on the same side.
- If one hip is fixed into abduction or adduction as the result of contracture.
- some other cause, the normal hip do the adducted/abducted an equal amount to the ensure accurate to leg length measurement.
- In North America, leg length measurement is usually taken from the ASIS to the medial malleolus; however, these values may be altered by muscle wasting on obesity.
- Measuring the lateral malleolus is less likely to be affected by the muscle bulk.
- To obtain the leg length, the examiner measures from the ASIS to the lateral or medial malleolus.
- The flat metal end of the tape measure is placed immediately distal to the ASIS &pushed up against it.
- The thumb then presses the tape end firmly against the bone, rigidly fixing the tape measure against the bone.
- The index finger of the other hand is placed immediately distal to the lateral or medial malleolus & pushed against it.
- The thumbnail is brought down against the tip of the index finger so that the tape measure is pinched between them.
- A slight difference as much as 1 to 1.5 cm in leg length is considered normal; however, this difference can still cause symptoms.
Weber – Barstow maneuver:
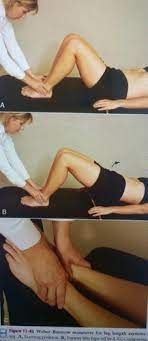
- It is also called the visual method.
- It is also be used to measure leg length asymmetry.
- The patient lies supine in starting position.
- In supine with the hips & knees flexed.
- The examiner stands at the patient’s feet & palpates the distal aspect of the medial malleoli with the thumbs.
- The patient then lifts the pelvis from the examining table & returns to the starting position.
- Next, the examiner passively extended the patient’s leg & compares the positions of the malleoli using the border of the thumb.
- Different levels indicate asymmetry.
If one leg is shorter than the other, the examiner can determine where the difference is by measuring the following:
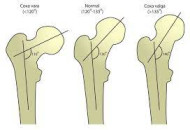
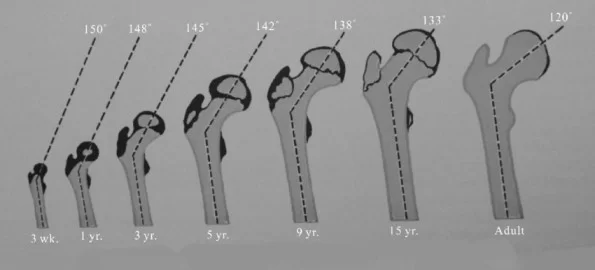
- For coxa vara or coxa valga means from the ilica crest to the greater trochanter of the femur :
- The neck-shaft angle of the femur is normally 150′ to 160′ at birth & decreases to between 120′ & 135′ in the adult.
- If the angle is less than 120′ in an adult, it is
- If the angle is more than 135′ in the adult, it is known as coxa valga.
- Form the greater trochanter of the femur to the knee joint line on the lateral aspect = for femoral shaft shorting.
- Form the knee joint line on the medial side to the medial malleolus = for tibial shaft shorting.
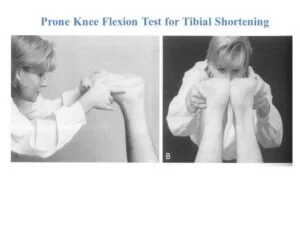
- The tibial length is relative also be examined when the patient in lying prone position.
- The examiner places the thumbs transversely across the soles of the feet just in front of the heels.
- The knees are flexed 90′,&the relative heights of the thumb are noted.
- Take care ensure that the legs are perpendicular to the examining table.
- Similarly, the femoral lengths can be compared by having the patient lie supine with the hips & knees flexed to 90′.
- When one femur is longer than the other, its height will be too higher.
Apparent shorting:
- It is also known as the functional shortening, of the leg is evident if the patient has a lateral pelvic tilt when the measurement is taken.
- Apparent or functional shorting of the limbs the result of adaptations the patient has made in response to pathology or contracture somewhere in the spine, pelvis, or lower limbs.
- In reality, there is no structural or anatomic difference in bone length.
- If there were, it would be called true shorting of the limb.
- For measures the apparent leg length shortening, the examiner is measure the distance from the tip of the xiphisternum /umbilicus to the medial malleolus.
- When true leg length is normal but the umbilicus-to-medial/lateral malleolus measurements are different,this situation is, this the presence of a functional leg length the discrepancy.
- Values obtained by these measurements may be affected by muscle wasting, obesity, asymmetric position of the xiphisternum or umbilicus, or asymmetric positioning of the lower limbs.
Standing [ functional ] leg length:
![Standing [ functional ] leg length Test](https://mobilephysiotherapyclinic.in/wp-content/uploads/2022/01/Standing-functional-leg-length-Test.webp)
- First assessed when the patient is in a relaxed position.
- In this position, the examiner palpates the ASIS & the PSIS, noting any asymmetry.
- The examiner then places the patient in an asymmetric stance, ensuring that the subtalar joint is in a natural position.
- The knees are extended&the toes are facing straight ahead.
- The ASIS & PSIS are again assessed for asymmetry.
- If differences are still noted, the examiner should check for structural leg length difference, sacroiliac joint dysfunction, or weak glutes medius or quadratus lumborum muscles.