
Bicipital Tendinitis: Symptoms, Diagnosis, Physiotherapy Treatment
Bicipital tendinitis is a condition characterized by inflammation or irritation of the biceps tendon. It commonly affects individuals involved in repetitive overhead activities or sports that require repetitive arm movements.
Introduction:
- Biceps tendinitis is caused by degeneration of the tendon from athletics requiring overhead motion or from the normal aging process.
- Inflammation of the biceps tendon in the bicipital groove, which is known as primary biceps tendinitis, occurs in 5 percent of patients with biceps tendinitis.
- Biceps tendinitis and tendinosis are commonly accompanied by rotator cuff tears or SLAP (superior labrum anterior to posterior) lesions.
- Patients with biceps tendinitis or tendinosis usually complain of a deep, throbbing ache in the anterior shoulder. The repetitive overhead motion of the arm initiates or exacerbates the symptoms.
- The most common isolated clinical finding in biceps tendinitis is bicipital groove point tenderness with the arm in 10 degrees of internal rotation.
- Local anesthetic injections into the biceps tendon sheath may be therapeutic and diagnostic.
- Ultrasonography is preferred for visualizing the overall tendon, whereas magnetic resonance imaging or computed tomography arthrography is preferred for visualizing the
- intra-articular tendon and related pathology. Conservative management of biceps tendinitis consists of rest, ice, oral analgesics, physical therapy, or corticosteroid injections into the biceps tendon sheath.
- Surgery should be considered if conservative measures fail after three months, or if there is severe damage to the biceps tendon.
Anatomy and Physiology:
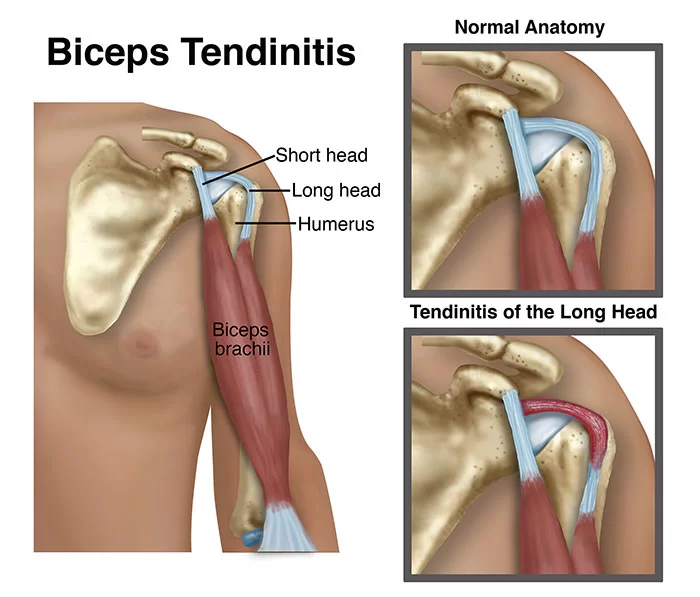
- The long head of the biceps tendon rises from the supraglenoid tubercle and the superior glenoid labrum.
- The proximal portion of the long head of the biceps tendon is extra synovial but intra-articular.
- The tendon travels obliquely inside the shoulder joint, across the humeral head anteriorly, and exits the joint within the bicipital groove of the humeral head beneath the transverse humeral ligament.
- The bicipital groove is defined by the greater tuberosity (lateral) and the lesser tuberosity (medial).
- The biceps tendon is contained in the rotator interval, a triangular area between the subscapularis and supraspinatus tendons at the shoulder. The rotator interval is responsible for keeping the biceps tendon in its correct location.6–8 Because the rotator interval is usually indistinguishable from the rotator cuff and capsule, lesions of the biceps tendon are usually accompanied by lesions of the rotator cuff.
- SLAP lesions are often present in patients with biceps tendinitis and tendinosis.
- The anterosuperior labrum and superior labrum are more likely to tear than the inferior portion of the labrum because they are not attached as tightly to the glenoid.9–13 Additionally, certain conditions that affect the glenohumeral joint may also involve the biceps tendon because it is intra-articular.
- These may include rheumatologic (e.g., rheumatoid arthritis, lupus), infectious, or other types of reactive or inflammatory conditions.
Symptoms of Bicipital Tendinitis:
- Patients with biceps tendinitis often complain of a deep, throbbing ache in the anterior shoulder.
- The pain is usually localized to the bicipital groove and may radiate toward the insertion of the deltoid muscle, or down to the hand in a radial distribution.
- This makes it difficult to distinguish from pain that is secondary to impingement or tendinitis of the rotator cuff, or cervical disk disease.
- Pain from biceps tendinitis usually worsens at night, especially if the patient sleeps on the affected shoulder.
- Repetitive overhead arm motion, pulling, or lifting may also initiate or exacerbate the pain.
- The pain is most noticeable in the follow-through of a throwing motion.
- Instability of the tendon may present as a palpable or audible snap when the range of motion of the arm is tested.
- The rupture of the biceps tendon is one of the most common musculotendinous tears.
- If the biceps has ruptured, patients will describe an audible, painful popping, followed by relief of symptoms.
- The anterior shoulder may be bruised, with a bulge visible above the elbow as the muscle retracts distally from the rupture point.
Risk factors of biceps rupture:
- History of rotator cuff tear
- Recurrent tendinitis
- Contralateral biceps tendon rupture
- Rheumatoid arthritis
- Age older than 40 years
- Poor conditioning
How to Diagnosis of Bicipital Tendinitis?
SLAP LESION :
- If a patient has a feeling of popping, catching, or locking in the shoulder, a SLAP lesion may be present.
- This usually occurs after trauma, such as a direct blow to the shoulder, a fall on an outstretched arm, or repetitive overhead motion in athletes.
The most common finding of biceps tendon injury is bicipital groove point tenderness.
Special test :
- Many provocative tests Yergason, Neer, Hawkins, and Speed tests) have been developed to isolate the pathology of the biceps tendon.
- However because these tests create impingement underneath the coracoacromial arch, it is difficult to rule out concomitant rotator cuff lesions.
The Yergason test :
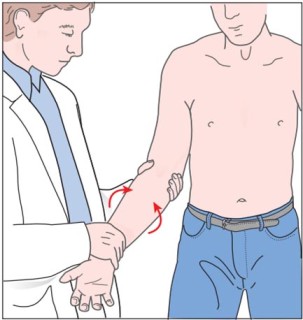
- The patient should be seated or standing in the anatomical position, with the humerus in a neutral position and the elbow in 90 degrees of flexion in a pronated position.
- The patient is asked to externally rotate and supinate their arm against the manual resistance of the therapist produced by wrapping the hand around the distal forearm (just above the wrist joint).
- Yergason’s Test is considered positive if the pain is reproduced in the bicipital groove and the biceps.
- SLAP lesion is suspected If a “clicking” sensation familiar to the patient is produced during the test.
- Damage to the transverse humeral ligament (which overlies the inter tubercular sulcus) should be suspected too.
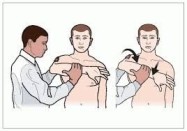
The Neer test :
- The examiner should stabilize the patient’s scapula with one hand, while passively flexing the arm while it is internally rotated.
- If the patient reports pain in this position, then the result of the test is considered to be positive.
Hawkins test :
- the patient flexes the elbow to 90 degrees while the physician elevates the patient’s shoulder to 90 degrees and places the forearm in a neutral position.
- With the arm supported, the humerus is rotated internally. The test is positive if bicipital groove pain is present.
Speed test :

- The patient tries to flex the shoulder against resistance with the elbow extended and the forearm supinated.
- A positive test is a pain radiating to the bicipital groove.
- If any of these tests is positive, it indicates that impingement is present, which can lead to biceps tendinitis or tendinosis.
Imaging study with Arthrography:
Used with MRI or CT to visualize the joint capsule and glenoid labrum
ADVANTAGES :
- CT arthrography shows biceps tendon subluxations, ruptures, dislocations, and SLAP lesions
- MRI arthrography is preferable for diagnosing biceps lesions and SLAP lesions14 because the agreement between MRI and arthroscopy for biceps lesions is only 37 percent and 60 percent for rotator cuff lesions
DISADVANTAGES :
- Invasive
- Filling of the biceps tendon sheath is unreliable
- Sharp images of the tendon may be lost
Ionizing radiation :
- Bicipital groove view radiography.
ADVANTAGES :
- Shows the width and medial wall angle of the bicipital groove, spurs in the groove, and supertubercular bone spur or ridge.
- Inexpensive.
DISADVANTAGES
- Does not show possible intra-articular disorders of the labrum (soft tissue injuries).
MRI:
ADVANTAGES:
- Excellent evaluation of the superior labral complex and biceps tendon
DISADVANTAGES:
- Partial tears of the biceps tendon are more difficult to detect than complete ruptures
- Expensive
- Poorly
Treatment of Bicipital Tendinitis:
Medical Treatment:
- Biceps tendinitis or tendinosis may respond to pain relieving medicine most commonly prescribed are nonsteroidal anti-inflammatory drugs (NSAIDs) such as Aceclofenac, and Diclofenac.
- Rest with the use of an Ice pack and a Hot Pack.
Physiotherapy Treatment in Bicipital Tendinitis:
- Ice, rest from overhead activity, or physical therapy
- Rehabilitation of an athlete’s shoulder involves four phases:
- Taping Over Biceps Muscle For Stabilising Purpose And Helps to Relieve Pain-Free Movement.
- rest; stretching exercises of the scapula, rotator cuff, and posterior capsule;
- The goal of stretching is to regain a balanced range of motion without stiffness or pain in any position.
- strengthening and a progressively difficult throwing exercise program.
- The patient may start exercises after the shoulder is pain-free.
Flexion and Extension exercise :
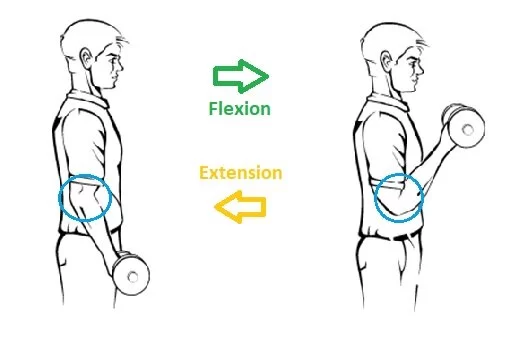
- Flex and extend the elbow on your injured side by gently bringing the palm of your hand up to the shoulder.
- Be sure to bend the elbow as much as possible. Then straighten your arm and elbow.
- Complete 15 repetitions.
- Rest, and then complete another set of 15 reps.
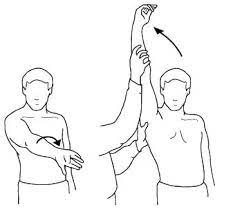
Vertical Shoulder Flexion :
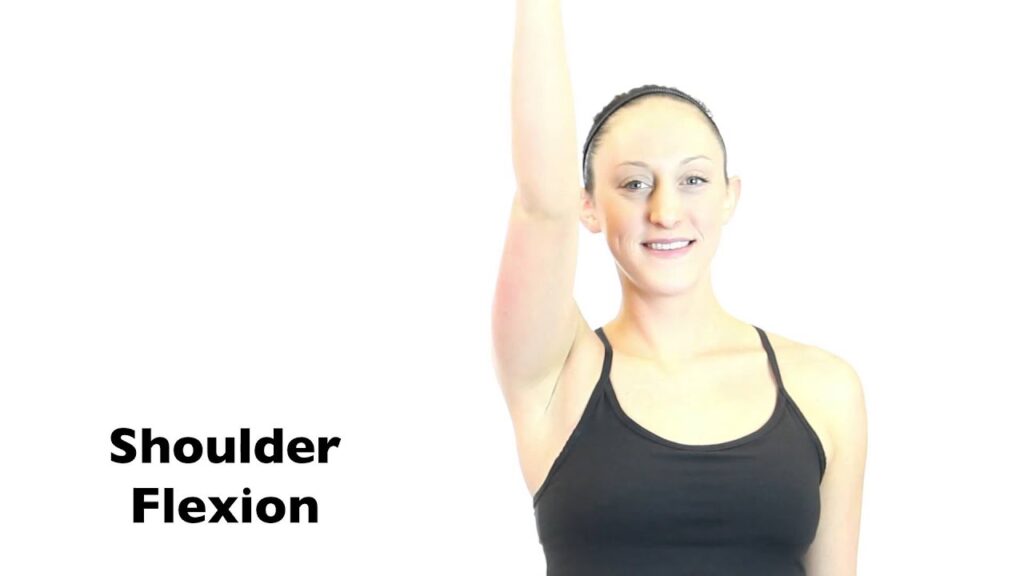
- This exercise helps you maintain your vertical range of motion while your tendon heals.
- Step 1: Stand upright with your injured arm hanging loose at your side.
- Step 2: Slowly raise your arm by bringing it in front of your body until it’s vertical over your head. Make sure to keep your elbow straight.
- Step 3: Hold your arm over your head for five seconds, then lower it back to your side.
- You can repeat this ten times per set, and complete three sets per day.
Biceps Curls :

- Biceps curls help maintain the flexibility of your elbow and maintain the strength of your biceps.
- Step 1: Stand upright with your injured arm hanging at your side, palm facing out.
- Step 2: Gently bend your injured arm at the elbow, bringing your palm toward your shoulder.
- Step 3: Hold this bend for thirty seconds, then slowly release it back to the starting position.
- You can do this twice per set, and complete two sets daily. As the exercise begins to feel easier, you can add weight to your hand.
Biceps Stretch :
- Stretching your biceps can help keep them from tightening and making tendonitis feel worse.
- Step 1: Stand six inches in front of a wall, and hold your injured arm out horizontally just below shoulder height.
- Step 2: Place the side of your thumb against the wall, keeping your hand palm-down.
- Step 3: Gently turn away from the wall in the opposite direction from your arm until you feel a stretch, then hold for fifteen seconds.
- You can repeat this three times daily.
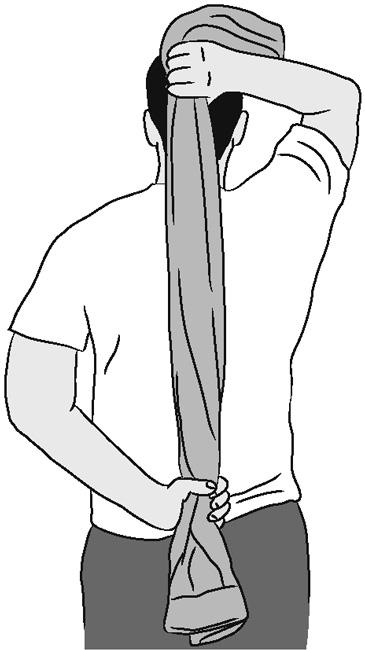
Internal Rotation Stretch :

- Internal rotation is the movement of your arm in the shoulder socket when your hands turn from facing from front to back, and it heavily involves your biceps tendon. This exercise helps maintain that rotation.
- Step 1: Stand upright and hold a yardstick, broom, or other stick behind your back in both hands, knuckles facing down.
- Step 2: Slowly raise the stick up your back with both hands until you feel a stretch in your injured arm.
- Step 3: Hold this position for thirty seconds, then gently release your arms back down.
- Repeat this twice in a row, twice daily, for four total repetitions.
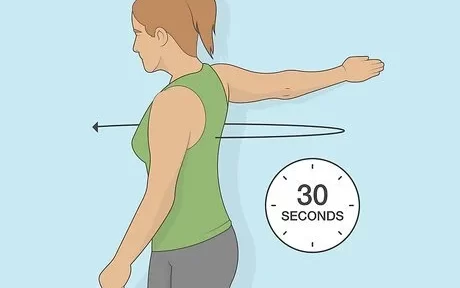
External Rotation Stretch :
- This exercise works the opposite motion of the internal rotation stretch.
- Step 1: Hold an exercise band in both hands at about waist height.
- Step 2: Gently pull it apart, keeping both elbows bent at a right angle so your arms are parallel to the floor.
- Step 3: When you feel a gentle stretch in your arm, slowly release back to a neutral position.
- You can repeat this ten times per set, and your goal should be to complete three sets.
Forearm Twists :
- Forearm twists help keep your arm flexible and help your tendon glide smoothly along the biceps muscle.
- Step 1: Allow your injured arm to hang at your side, then bend your elbow to a 90-degree angle.
- Step 2: Turn your palm so it faces upward, and hold the position for five seconds.
- Step 3: Rotate your palm so it faces downward, and hold the position for five seconds.
- Repeat this ten times per set, and aim for three sets per day.
Sleeper Stretch :
- Lie on the injured side.
- Use a pillow for your head, and bend your knees for comfort and stability.
- Bend the elbow of the injured arm so that you fingers point toward the ceiling, then use your other hand to gently push the injured arm toward the floor.
- Resist the push to feel the stretch, and focus on keeping your shoulder blades squeezed together as you move through the exercise.
- Hold the stretch for 30 seconds, then rest and repeat twice more.
FAQs
How do you treat Bicipital tendonitis?
Treatments of Bicipital tendonitis are:
Resting the shoulder could be beneficial if some of the irritation is caused by overuse.
NSAIDs, or nonsteroidal anti-inflammatory medications. By reducing inflammation around the biceps tendon, these oral medicines help decrease discomfort.
Physical Therapy
Stretching and strengthening.
Hot and Cold pack
Kinesio Taping
Corticosteroids.
What causes bicipital tendinitis?
Overuse syndromes of the shoulder, which are very common among overhead sportsmen like baseball pitchers, swimmers, gymnasts, racquet sport enthusiasts (e.g., tennis players), and rowing/kayak athletes, are often the cause of bicipital tendinitis.
What are the signs and symptoms of bicipital tendonitis?
signs and symptoms of bicipital tendonitis are:
The front of the shoulder is sore or painful, and any exercise or lifting above makes it worse.
An aching or pain radiating down the upper arm bone.
a random shoulder cracking sound or feeling.
How do you test for bicipital tendinitis?
Yergasons test:
In order to do Yergason’s test, the patient must supinate against resistance while placing their arm at their side with their elbow bent to a 90-degree angle. If discomfort is localized to the bicipital groove, the test is considered positive.
Can I lift weights with bicep tendonitis?
Exercise for the arms is not advised if you have tendinitis in your biceps. It’s preferable to let the region rest and recover instead. You can concentrate on lower body and core activities, as well as aerobic workouts that don’t make the discomfort worse.
Can I exercise with tendonitis?
You can still work out and stay healthy by using the muscles in your lower body, even if you have tendinopathy in your elbow or wrist. For a week or two, though, it is preferable to reduce the intensity of upper body resistance exercise and instead concentrate on extending the muscles.
What are the 2 types of bicep tendonitis?
Types of bicep tendonitis
Distal bicep tendonitis:
Inflammation near the end of the tendon that connects the biceps muscle to the elbow is known as distal bicep tendonitis.
Proximal bicep tendonitis:
Inflammation near the end of the tendon that joins the biceps muscle to the shoulder is known as proximal bicep tendonitis.



8 Comments