
Superior Oblique muscle
Introduction
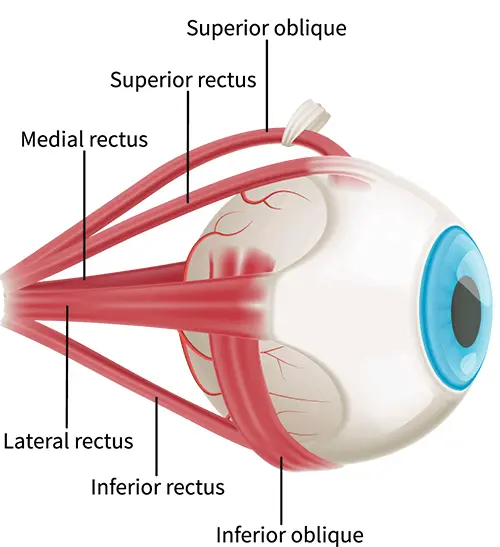
The superior oblique is one of the two significant oblique extraocular muscles. These muscles are distinctive in that they do not originate from the common tendinous ring, have an angular attachment to the eyeball, and connect to the posterior aspect of the eyeball. The superior oblique function explicitly moves the eye in the down-and-out position and/or in tort the eye.
The superior oblique muscle is situated in the upper medial part of the orbit, attaching its medial wall. The muscle is located superior to the medial rectus and medial to both the superior rectus and levator palpebrae superioris muscle.
The eyeball and all of the extraocular muscles are enveloped by a muscular fascia, emanating from the fascial sheath of the eyeball (Tenon’s capsule). This is an important clinical point because the sub-tendinous space is a common location for the injection of local anesthetics during various surgical procedures in this region.
Embryology
The superior oblique muscle arises at week 6 of development along with the medial rectus, while most additional extraocular muscles appear at week 5.
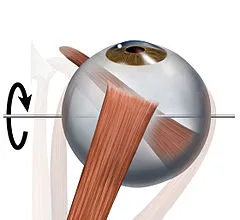
The unique pulley motion of the superior oblique along the trochlea is due to the specialized development of the muscle. Embryologic studies show that at the early stage of development, the muscles themselves, the insertion tendon, and the cartilaginous pulley travel together in a straight line. At around 12 weeks, the tendon then initiates to turn around the trochlear cartilage, creating the pulley action.
Origin of superior oblique muscle
The superior oblique muscles originate from the body of the sphenoid bone, medial to the origin of the levator palpebrae superioris muscle, and superomedial to the optic canal. In distinction to the other extraocular muscles, the superior oblique and inferior oblique do not arise from the common tendinous ring. Rather superior oblique arises externally, superomedially to the tendinous ring.
Insertion
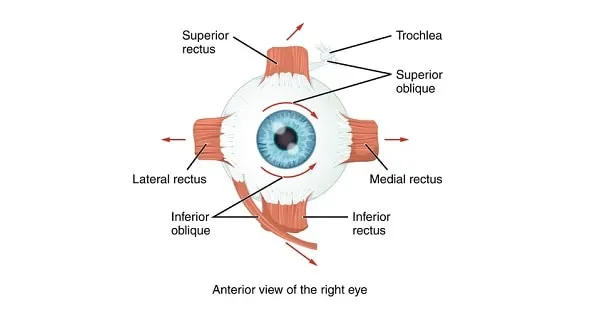
From its sphenoid attachment, the superior oblique muscles run anteriorly, parallel to the medial wall of the orbit. Around its insertion, the muscle-tendon hooks around a cartilaginous pulley named the trochlea of the superior oblique. This cartilaginous loop is found connected to the nasal part of the frontal bone. It is located between the tendon and the trochlea and is a thin separating synovial sheet.
From the trochlea, the tendon takes a sharp posterolateral turn before inserting it onto the posterior-superolateral scleral surface of the eye. This insertion is located behind the equator of the eyeball, between the attachment of the superior rectus and lateral rectus muscles.
Nerve supply
The superior oblique is the singular extraocular muscle that obtains its innervation through the trochlear nerve (CN IV). The trochlear nerve is the only cranial nerve that appears from the posterior aspect of the brainstem. It takes a fairly long route through the endocranium and enters the orbit via the superior orbital fissure to innervate the superior oblique muscle.
In clinical practice, it’s important to keep in mind the fact that except for the superior obliques and lateral rectus, all extraocular muscles are supplied by the oculomotor nerve (CN III).
Blood supply
The superior oblique is vascularized by little branches of the anterior ciliary arteries which are derived from the ophthalmic artery.
Function of superior oblique muscle
The belly of the superior oblique muscle is situated posterior to the eyes. However, because the tendon of the muscle travels the trochlea of the orbit, the muscle-tendon approaches the eyeball from the front and connects its superior aspect. This permits the superior oblique to direct the gaze in several different movements while providing stability for the eyeball by counteracting head movements. When the eyeball is in a neutral position, the superior oblique is responsible for abduction (directed laterally from the nose), depression (inferiorly), and internal rotation (movement of the superior pole of the eye occurs medially) of the eyeball.
Note that these functions are not equally efficient in every position of the eyes; internal rotation (intorsion) of the eyeball is specifically adequate when the eyes are in the abducted position, while depression of the eyeball is strongest when the eyes are in the adducted position. The superior oblique muscle function antagonistically to the inferior oblique muscle.
By rejecting the action of the inferior rectus muscle via contraction of the medial rectus, one can isolate the action of the superior oblique.
Clinical relations
The insufficient function of the superior oblique muscle is usually driven by lesions of the trochlear nerve somewhere on its long path from the brainstem to the orbit. Isolated injury of this nerve is fairly periodic, it’s usually combined with damage to other cranial nerves. When isolated or/and combined palsy of extraocular muscles does occur, it is typically due to injury or pathological approaches within the endocranium or the orbit.
The main symptom of superior oblique dysfunction is diplopia (double vision) which happens when directing the gaze downward. Diplopia happens because this muscle functions as a depressor of the eyeball, specifically when the eye is in an abducted position. Patients usually neutralize this symptom by leaning the head anterolaterally towards the normal eye. When the superior oblique muscle is paralyzed, the movement of the inferior oblique is unopposed. For this reason, the movements of the two eyes are not synchronized when directing the gaze lowered and medially.
Superior oblique palsy is a common difficulty of closed-head trauma. Restriction of superior oblique motion due to an inelastic tendon is found in Brown syndrome, leading to a problem elevating the eye in the adducted position.
Superior oblique myokymia is an unusual neurological condition caused by vascular compression of the trochlear nerve resulting in repeated, brief, involuntary attacks of movement of the eye.
Surgical operations of the superior oblique contain tenotomy, recession, silicone expander lengthening, split tendon lengthening, tucking, and the Harada-Ito procedure.
Exercise of superior oblique muscle
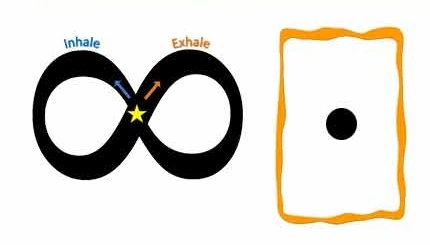
Figure eights
This exercise is great for strengthening the muscles in the eyes to enhance control and function. Sit or stand in a comfortable position. Trace an invisible figure 8 along the floor in front of you about eight to 10 feet in the distance without moving the head. Trace the lines in one direction and then switch to the other direction. Perform three to five sets of exercises daily.
Treatment:
- The treatment of fourth nerve palsy includes both non-surgical and surgical interventions.
- Many cases of acute acquired fourth nerve palsy spontaneously resolve with time.
- Observation
- Prism therapy
- Occlusion
- Botulinum toxin injection
- Strabismus surgery
FAQ
Where is the superior oblique muscle?
The superior oblique muscle is situated in the upper medial portion of the orbit, adjoining its medial wall. The muscles are located superior to the medial rectus and medial to both the superior rectus and levator palpebrae superioris muscles.
How accomplishes the superior oblique muscle move the eye?
The superior rectus muscle and inferior oblique muscle primarily move the eye upward. The inferior rectus muscle and superior oblique muscle primarily move the eye downward. The lateral rectus muscle moves the eye horizontally laterally (abduction). The medial rectus muscle moves the eye horizontally and medially (adduction).
What is the movement of the superior oblique?
The superior oblique muscle’s primary movement is eye intorsion, with secondary and tertiary movements being eye depression and abduction, respectively. Because the superior oblique assists depress the eye, trochlear nerve palsy results in upward deviation of the eye (hypertropia)
What occurs if the superior oblique muscle is damaged?
Weakness of the superior oblique muscle generates misalignment of the eyes. Misalignment is most usually vertical, but can also be horizontal and torsional. Palsy refers to the complete deficiency of a muscle while paresis is a partial weakness. This disease is mostly unilateral (one eye) but can be bilateral (both eyes).


One Comment