
ABDUCENS NERVE
INTRODUCTION :

ABDUCENS NERVE
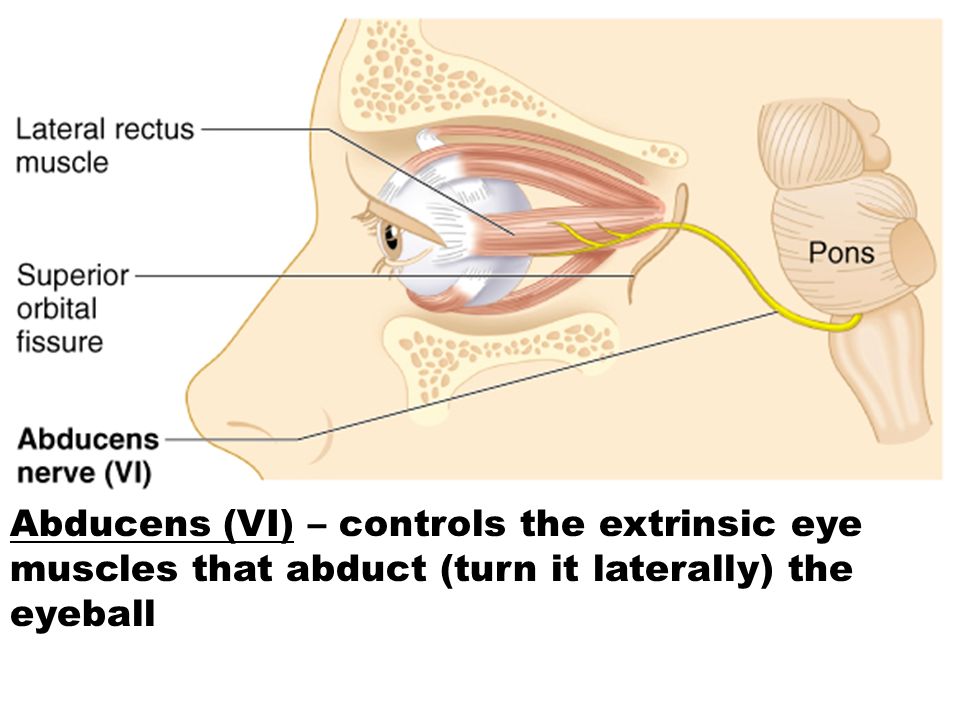
The abducens nerve (or abducent nerve) is the sixth cranial nerve (CNVI), in humans body that controls the movement of the lateral rectus muscle, responsible for outward gaze.
It is a somatic efferent nerve.
ANATOMY OF ABDUCENS NERVE :

ANATOMY OF ABDUCENS NERVE
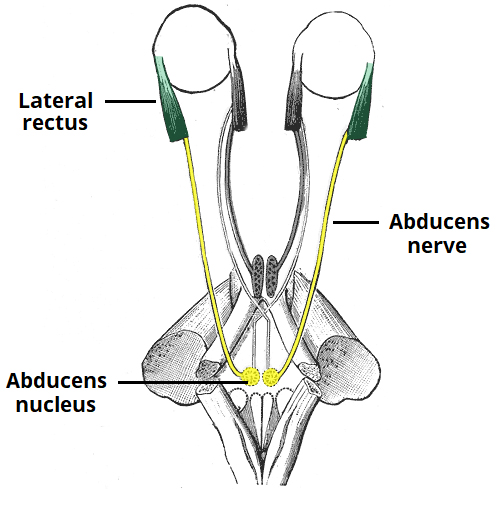
The abducens nerve arises from the abducens nucleus in the pons of the brainstem. It exits the brainstem at the junction of the pons and the medulla.
It then enters the subarachnoid space and pierces the dura mater to travel in an area known as Dorello’s canal.
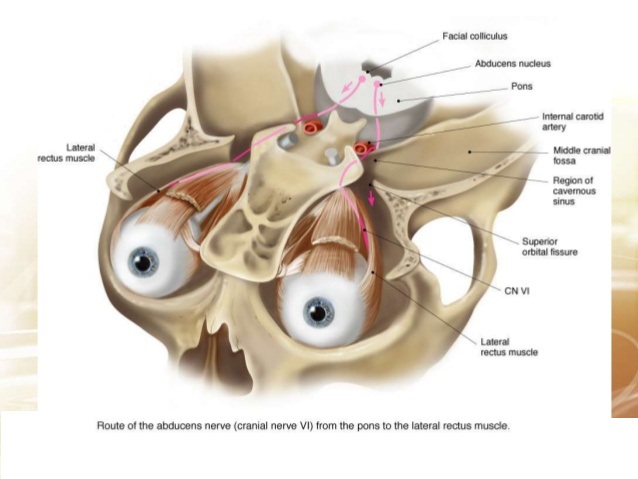
At the tip of petrous temporal bone, the abducens nerve leaves Dorello’s canal and enters the cavernous sinus (a dural venous sinus).
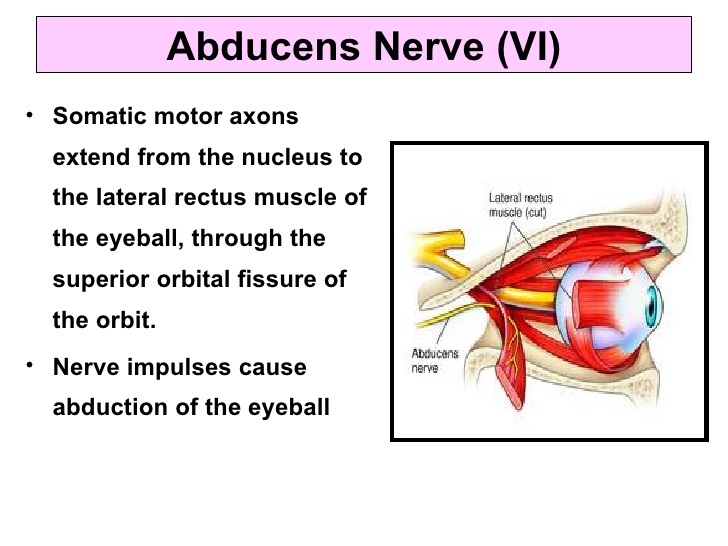
It travels through the cavernous sinus and enters the bony orbit via the superior orbital fissure.
Within the bony orbit, the abducens nerve terminates by innervating the lateral rectus muscle.
STRUCTURE AND FUNCTION :

STRUCTURE OF ABDUCENS NERVE
NERVES :
- The nerve itself can be divided into four distinct portions :
The nucleus, the cisternal portion, the cavernous sinus portion, and the orbital portion.
Nucleus :
- The abducens nucleus is a small nucleus situated at the upper part of the rhomboid fossa beneath the colliculus facialis within the pons.
Cisternal portion :
- It is the most medial of the nerves emerging immediately below the pons (facial nerve and vestibulocochlear nerve lateral to it) at the pontomedullary junction into the prepontine cistern.
- It courses anteriorly towards the clivus where it runs superiorly along the clivus enclosed within a fibrous sheath called Dorello canal and pierces the dura inferior to the posterior clinoid process.
- It then courses over the medial petrous apex towards the cavernous sinus.
- Its oblique course and relatively anchored position in Dorello canal make it prone to stretching when raised intracranial pressure from a space-occupying lesion causes transtentorial herniation (a sixth nerve palsy is the classic lateralising sign of an extradural haematoma).
Cavernous sinus portion :
- Within the cavernous sinus, the abducens nerve is located inferolateral to the internal carotid artery, medial to the lateral wall of the sinus.
Orbital portion :
- Having entered the orbit through the superior orbital fissure within the tendinous ring it supplies the lateral rectus.
- It is the most inferior nerve passing through the tendinous ring, inferior to the inferior division of the oculomotor nerve.
Motor Function :

MOTOR FUNCTION
- The oculomotor nerve, trochlear nerve and the abducens nerve is a purely somatic nerve, meaning the nerve has no sensory function.
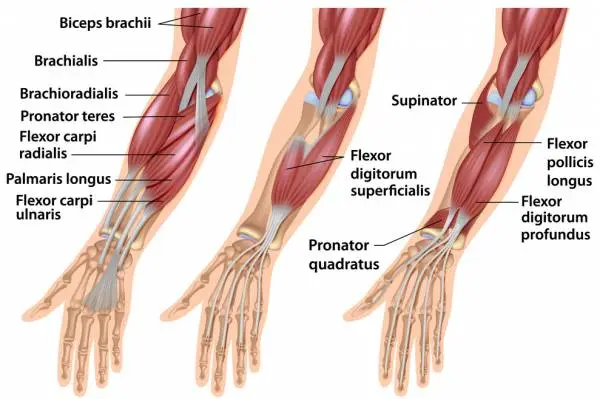
- The abducens nerve provides innervation to the lateral rectus muscle – one of the extraocular muscles.
- Its main function is to carry general somatic efferent nerve axons to innervate the lateral rectus muscle which then abducts the eye on the ipsilateral side.
- It is also secondarily involved in innervation of the contralateral medial rectus muscle by way of the medial longitudinal fasciculus so that both eyes move laterally in a coordinated manner.
- The lateral rectus originates from the lateral part of the common tendinous ring, and attaches to the anterolateral aspect of the sclera. It acts to abduct the eyeball. (i.e. to rotate the gaze away from the midline)
CLINICAL RELEVANCE :
Examination of the Abducens Nerve :
- The abducens nerve is examined in conjunction with the oculomotor and trochlear nerves by testing the movements of the eye.
- The patient is asked to follow a point with their eyes (commonly the tip of a pen) without moving their head.
- The target is moved in an ‘H-shape’ and the patient is asked to report any blurring of vision or diplopia (double vision).
Abducens Nerve Palsy :

ABDUCENS NERVE PALSY
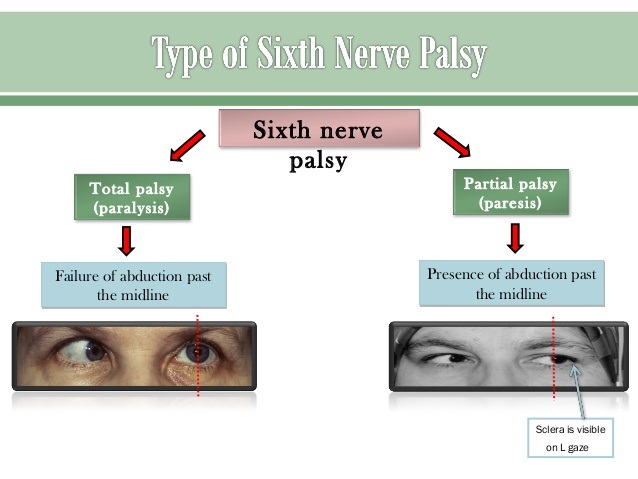
- Abducens nerve palsy can be caused by any structural pathology which leads to downwards pressure on the brainstem (e.g. space-occupying lesion). This can stretch the nerve from its origin at the junction of the pons and medulla.
- Other causes include diabetic neuropathy and thrombophlebitis of the cavernous sinus (in these cases, it is rare for the abducens nerve to be affected in isolation).
- Clinical features of abducens nerve palsy include diplopia, the affected eye resting in adduction (due to unopposed activity of the medial rectus), and inability to abduct the eye.
- The patient may attempt to compensate by rotating their head to allow the eye to look sideways.
other related posts :



One Comment