

Below Knee Amputation
Introduction
A below-knee amputation (“BKA”) is a transtibial amputation that involves removing the foot, ankle joint, distal tibia, and fibula with related soft tissue structures. In general, a BKA is preferred over an above-knee amputation (AKA), as the former has better rehabilitation and functional outcomes.
The rates of lower extremity amputation have declined in recent years. This surgical operation carries significant morbidity, yet it remains a treatment modality with vital clinical and often life-saving significance given appropriate indications
Anatomy and Physiology
There are 4 fascial compartments in the lower leg, containing muscles to the leg and foot and important neurovascular structures.
Bones:
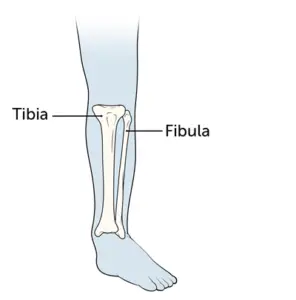
- tibia
- fibula
The lower leg contains two major long bones, the tibia, and the fibula, which are both very strong skeletal structures. The tibia (also called the shinbone) is located near the midline of the leg and is the thicker and stronger of the two bones. The fibula, also called the calf bone, is significantly smaller and is situated on the lateral (farther from the midline) side of the tibia
Muscles
Muscles in the Anterior Compartment of the Leg
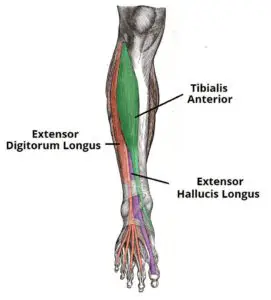
There are four muscles in the anterior compartment of the leg: tibialis anterior, extensor digitorum longus, extensor hallucis longus, and fibularis tertius.
Collectively, they act to dorsiflex and invert the foot at the ankle joint. The extensor digitorum longus and extensor hallucis longus also extend the toes. The muscles in this compartment are innervated by the deep fibular nerve (L4-S1), and blood is supplied via the anterior tibial artery.
Muscles in the Lateral Compartment of the Leg
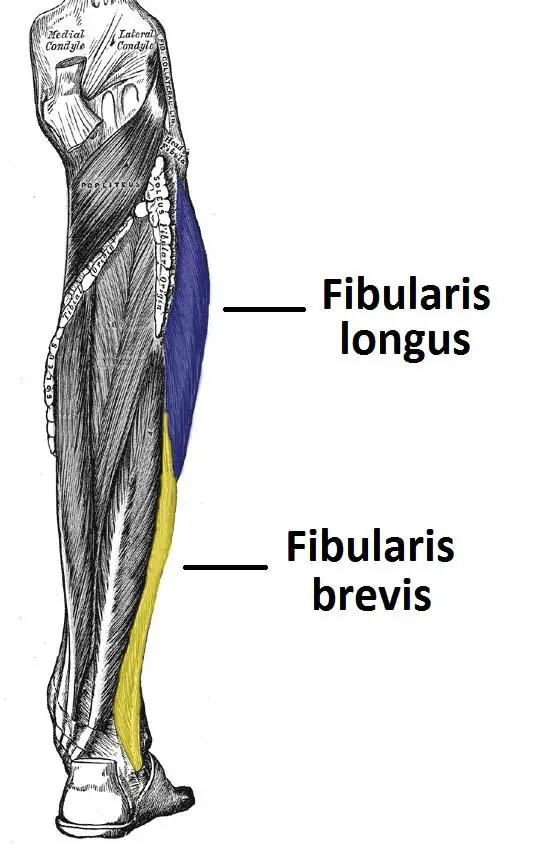
There are two muscles in the lateral compartment of the leg; the fibularis longus and brevis (also known as peroneal longus and brevis).
The common function of the muscles is eversion – turning the sole of the foot outwards. They are both innervated by the superficial fibular nerve.
Muscles in the Posterior Compartment of the Leg
The posterior compartment of the leg contains seven muscles, organized into two layers – superficial and deep. The two layers are separated by a band of fascia.
The posterior leg is the largest of the three compartments. Collectively, the muscles in this area plantarflex and invert the foot. They are innervated by the tibial nerve, a terminal branch of the sciatic nerve.
Superficial Muscles
The superficial muscles form the characteristic ‘calf’ shape of the posterior leg. They all insert into the calcaneus of the foot (the heel bone), via the calcaneal tendon. The calcaneal reflex tests spinal roots S1-S2.
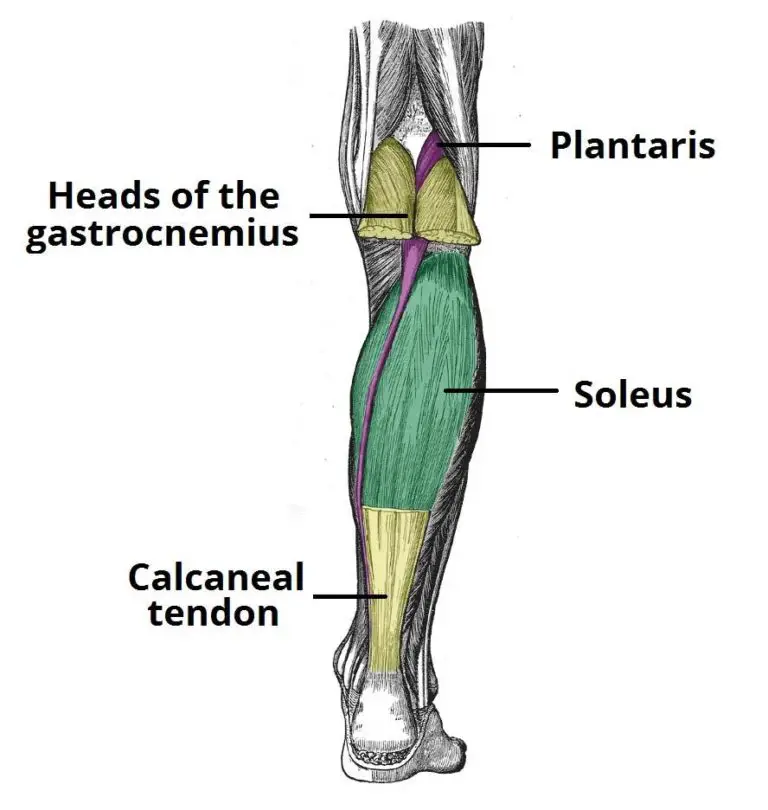
- Gastrocnemius
The gastrocnemius muscle is the most superficial of all the muscles in the posterior leg. It has two heads – medial and lateral, which converge to form a single muscle belly.
- Soleus
The soleus is located deep in the gastrocnemius. It is large and flat, named soleus due to its resemblance to a sole – a flat fish.
- Plantaris
The plantaris is a small muscle with a long tendon. It is absent in 10% of people
Deep Muscles
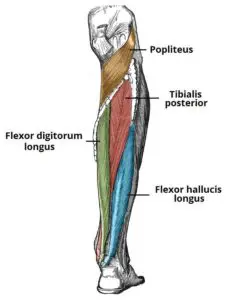
There are four muscles in the deep compartment of the posterior leg. One muscle, the popliteus, acts only on the knee joint. The remaining three muscles (tibialis posterior, flexor hallucis longus, and flexor digitorum longus) act on the ankle and foot
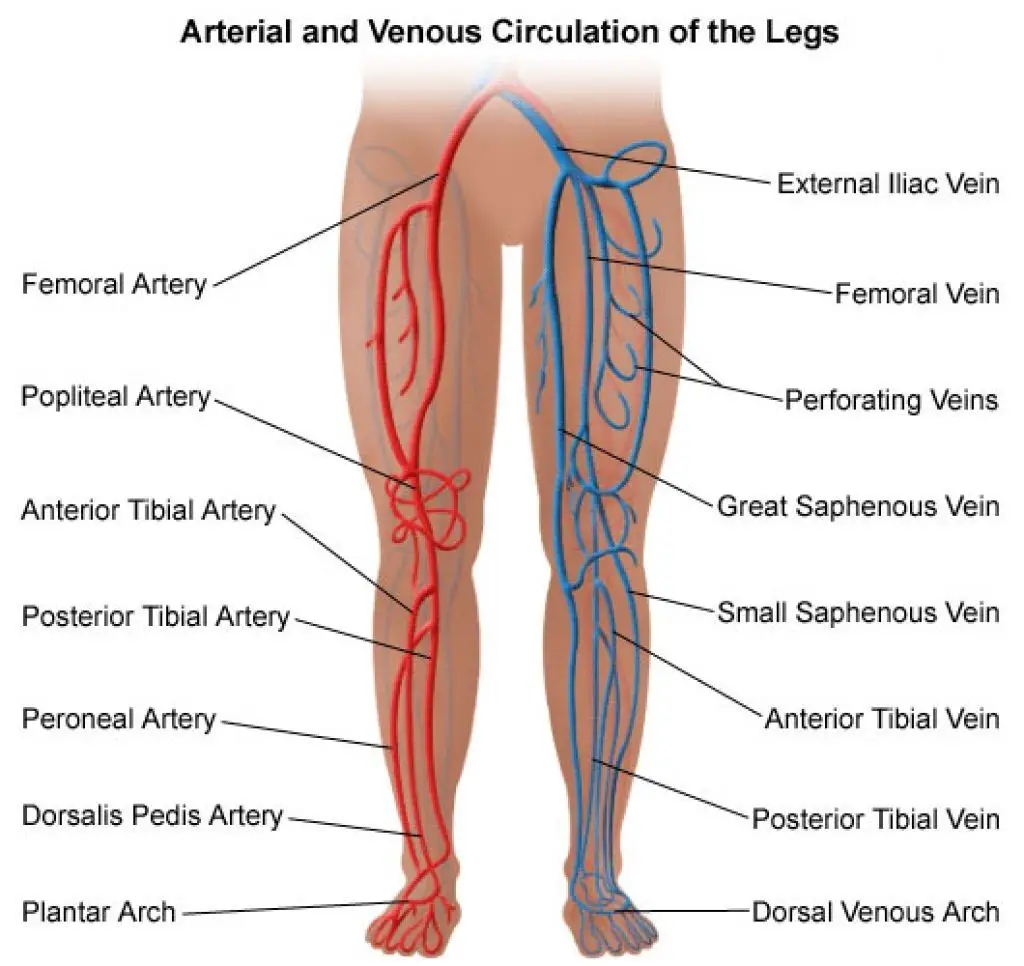
Arteries:
anterior and posterior tibial arteries
Veins:
small/short saphenous, great/long saphenous, tibial and fibular veins
Nerves:
common fibular/peroneal, tibial and saphenous nerves, branches of the sciatic and femoral nerves
Indications
- Peripheral vascular disease (PVD)
- Trauma
- Tumors
- Infections
- Congenital limb deficiency
- non-healing diabetic wounds
LEVEL OF AMPUTATION Determined by :
- Disease process
- Viability of tissues and
- Prosthesis available
Determination of adequate blood flow
Clinical:
i) lowest palpable pulse
i) skin colour and temperature
iii) bleeding at surgery
Others:
- Doppler ultrasonography:
- Ankle: brachial index > 0.5.
- Transcutaneous oxygen measurement
- Transcutaneous oxygen measurement
Contraindications
poor health that impairs the patient’s ability to tolerate anesthesia and surgery
Complications
- Oedema
- Wounds and infection
- Pain
- Muscle weakness and contractures
- Joint instability
- Autonomic dysfunction
- Osseointegration specific complications
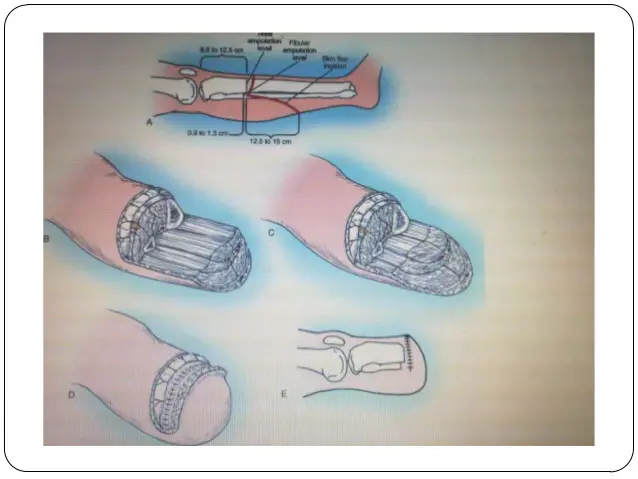
Amputations Technique
- An incision to outline a long posterior flap & a short anterior one — combined length 1 ½ times the diameter of the leg at the level of amputation.
- Deepened to the bone, Periosteum raised.
- Section tibia at level of incision, bevel anterior surface. Fibular 2-3cm proximally. Smoothen round sharp margins
- Vessels isolated and double ligated, Nerves pulled. down & cut with a sharp knife & allowed to retract into the soft tissue
- Irrigation with N/S, Removal of tourniquet to meticulously secure haemostasis.
- Myoplasty or Myodesis done over a drain after trimming the Muscle to size.
- Close skin with interrupted non absorbable sutures.
- Wound dressing- soft or rigid.
COMPLICATIONS
Early
- Haemorrhage
- Haematoma
- Infection
Late
- depression
- Stump ulceration
- Flap necrosis
- Painful scar
- Phantom limb
- Phantom pain
- Joint stiffness
- Osteomyelitis
- Osteoporosis & tendency to fracture
Physiotherapy for Below-Knee Amputation (Transtibial Amputation)
Prior to Surgery
Before your surgery, your physical therapist may:
- Prescribe exercises for preoperative conditioning, and to improve the strength and flexibility of the hip and knee
- Teach you how to walk with a walker or crutches
- Educate you about what to expect after the procedure
Immediately After Surgery
Your hospital stay will be approximately 5 to 14 days after surgery. Your wound will be bandaged, and you may also have a drain at the surgery site—a tube that is inserted into the area to help remove excess fluid. Pain will be managed with proper medication.
Physical therapy will begin soon after surgery when your condition is stable and the doctor clears you for rehabilitation. A physical therapist will review your medical and surgical history, and visit you at your bedside. Your first 2 to 3 days of treatment may include:
- Gentle stretching and range-of-motion exercises
- Learning to roll in bed, sit on the side of the bed, and move safely to a chair
- Learning how to position your surgical limb to prevent contractures (the inability to straighten the knee joint fully, which results from keeping the limb bent too much)
When you are medically stable, the physical therapist will help you learn to move about in a wheelchair, and stand and walk with an assistive device.
Rehabilitation
Your physical therapist will work with you as you heal following the amputation, help to fit your prosthesis, and guide your rehabilitation to ensure you regain your strength and movement in the safest way possible. Your treatments may include:
Prevention of contractures.
A contracture is the development of soft-tissue tightness that limits joint motion. The condition occurs when muscles and soft tissues become stiff from lack of movement. The most common contracture following transtibial amputation occurs at the knee when it becomes flexed and unable to straighten. The hip also may become stiff.
It is important to prevent contractures early; they can become permanent if not addressed following surgery, throughout recovery, and after rehabilitation is completed. Contractures can make it difficult to wear your prosthesis and make walking more difficult, increasing the need for an assistive device like a walker.
Your physical therapist will help you maintain normal posture and range of motion at your knee and hip. Your therapist will teach you how to position your limb to avoid the development of contracture and show you stretching and positioning exercises to maintain a normal range of motion (ROM).
ROM exercises should be incorporated to avoid contractures, as well as prone lying to prevent hip flexion contractures, a sandbag could be placed next to the residuum to prevent a hip abduction contracture. A sandbag could also be placed on the lower part of a transtibial residuum when the patient is prone, to prevent hip flexion contractures.
Compression to reduce swelling.
It is normal to experience postoperative swelling. Your physical therapist will help you maintain compression on your residual limb to protect it, reduce and control swelling, and help it heal. Compression can be accomplished by:
- Wrapping the limb with elastic bandages
- Wearing an elastic shrinker sock
These methods also help shape the limb to prepare it for fitting the prosthetic leg.
In some cases, a rigid dressing, or plaster cast, may be used instead of elastic bandages. An immediate postoperative prosthesis made with plaster or plastic also may be applied. The method chosen depends on each person’s situation. Your physical therapist will help monitor the fit of these devices and instruct you in their use. The main goal of your care during this time is to reduce swelling.
Pain management
Your physical therapist will help with pain management in a variety of ways, including:
- Manual therapy, which may include “hands-on” treatments performed by your physical therapist, including soft tissue (ie, muscle, tendon) mobilization, joint manipulation, or gentle range-of-motion exercises, in order to improve circulation and joint motion
- Stump management, including skin care and stump sock use
- Desensitization helps modify how sensitive an area is to clothing, pressure, or touch Desensitization involves stroking the skin with different types of touch to help reduce or eliminate sensitivity
- Mirror therapy and/or graded motor imagery
Approximately 80% of people who undergo amputations experience a phenomenon called phantom limb pain, a condition in which some of their pain feels like it is actually coming from the amputated limb. Your physical therapist will work with you to lessen and eliminate the sensation.
Prosthetic fitting and training
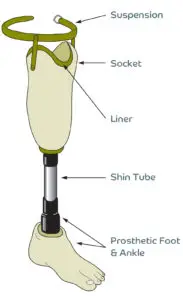
Your physical therapist will work with a prosthetist to prescribe the best prosthesis for your life situation and activity goals. You will receive a temporary prosthesis at first while your residual limb continues to heal and shrink/shape over the first 6 to 9 months of healing. The prosthesis will be modified to fit as needed over this time.
Most people with transtibial amputations learn to walk well with a prosthesis. Physicians use the following criteria to determine when you are ready for a temporary prosthesis, or your first artificial limb.
- Your incision should be almost healed or completely healed.
- Your swelling should have decreased to an acceptable amount.
- You will have regained sufficient overall strength to be able to walk safely.
After the limb has reached a stable shape, and your physician approves your condition, you will be fitted for a permanent prosthesis.
Functional training
After you move from acute care to rehabilitation, you will learn to function more independently. Your physical therapist will help you master wheelchair mobility and walking with an assistive device like crutches or a walker. Your therapist also will teach you the skills you need for the successful use of your new prosthetic limb. You will learn how to care for your residual limb with skin checks and hygiene and continue contracture prevention with exercise and positioning.
Your physical therapist will teach you how to put your new prosthesis on and take it off, and how to manage a good fit with the socket type you receive. Your therapist will help you to gradually build up a tolerance for wearing your prosthesis for increasingly longer times while protecting the skin integrity of your residual limb. You will continue to use a wheelchair for getting around, even after you get your permanent prosthesis, for times when you are not wearing the limb.
Guided rehabilitation
Prosthetic training is a process that can last up to a full year. You will begin when your physician clears you for putting weight on the prosthesis. Your physical therapist will help you learn to stand, balance, and walk with the prosthetic limb.
Most likely you will begin walking in parallel bars, then progress to a walker, and later as you get stronger, you may progress to using a cane before walking independently without any assistance. You will also need to continue strengthening and stretching exercises to achieve your fullest potential, as you return to many of the activities you performed before your amputation.
FAQ
What is the difference between BKA and AKA?
BKA stands for “Below-Knee Amputation,” involving surgical removal of the leg below the knee. AKA stands for “Above-Knee Amputation,” involving surgical removal of the leg above the knee.
What is BKA procedure?
A transtibial amputation involving the removal of the foot, ankle joint, distal tibia, fibula, and associated soft tissue components is known as a below-knee amputation (BKA).
How is BKA performed?
A cut is made below the intended amputation level. The skin and muscles of the calf are sliced to form a “flap.” A saw is used to cut the leg bones. Under a procedure known as the Ertl technique, certain surgeons may fuse the ends of the tibia and fibula together.
What is the minimum length for BKA?
Transtibial Amputation (BKA): Less than 20% of the tibial length is preserved in very short transtibial amputations. kept intact. For a prosthesis to fit as well as possible, at least 8 centimeters of tibia below the knee joint is needed. When more than 50% of the tibial length is retained, a long transtibial amputation takes place.
What is the positioning for BKA patients?
Yes, lie down on a hard couch or bed. Never place a pillow underneath your remaining limb. Place cushions outside of your thighs. Avoid crossing your legs. Avoid hanging your remaining limb over the edge of the couch or bed.
Author: Nitesh Patel - Physiotherapist
Physiotherapist in Samarpan Physiotherapy Clinic Ahmedabad Bapunagar Amaraiwadi Vastral Mobile Physiotherapy Clinic Dr. Nitesh Patel ( Physiotherapist ) : Mo No : 09898607803


One Comment