Fracture Displacement
Overview
When your bone broke, the fragments migrated so far that a space developed surrounding the fracture, which is known as a displaced fracture. Although the fragments were not dislocated sufficiently during the break to be out of alignment, non-displaced fractures are nonetheless shattered bones.
Fracture displacement is described as the aberrant location of the distal fracture fragment relative to the proximal bone.
FRACTURE: A fracture, often known as a crack or break, is a broken bone. There are numerous ways in which a bone can break, either whole or partially (crosswise, longitudinally, or in multiple parts).
DISPLACEMENT: The ends of the bone become misaligned when a fracture is displaced. In such circumstances, realigning the fractured bone is necessary for optimum healing.
Types Of Fracture Displacement
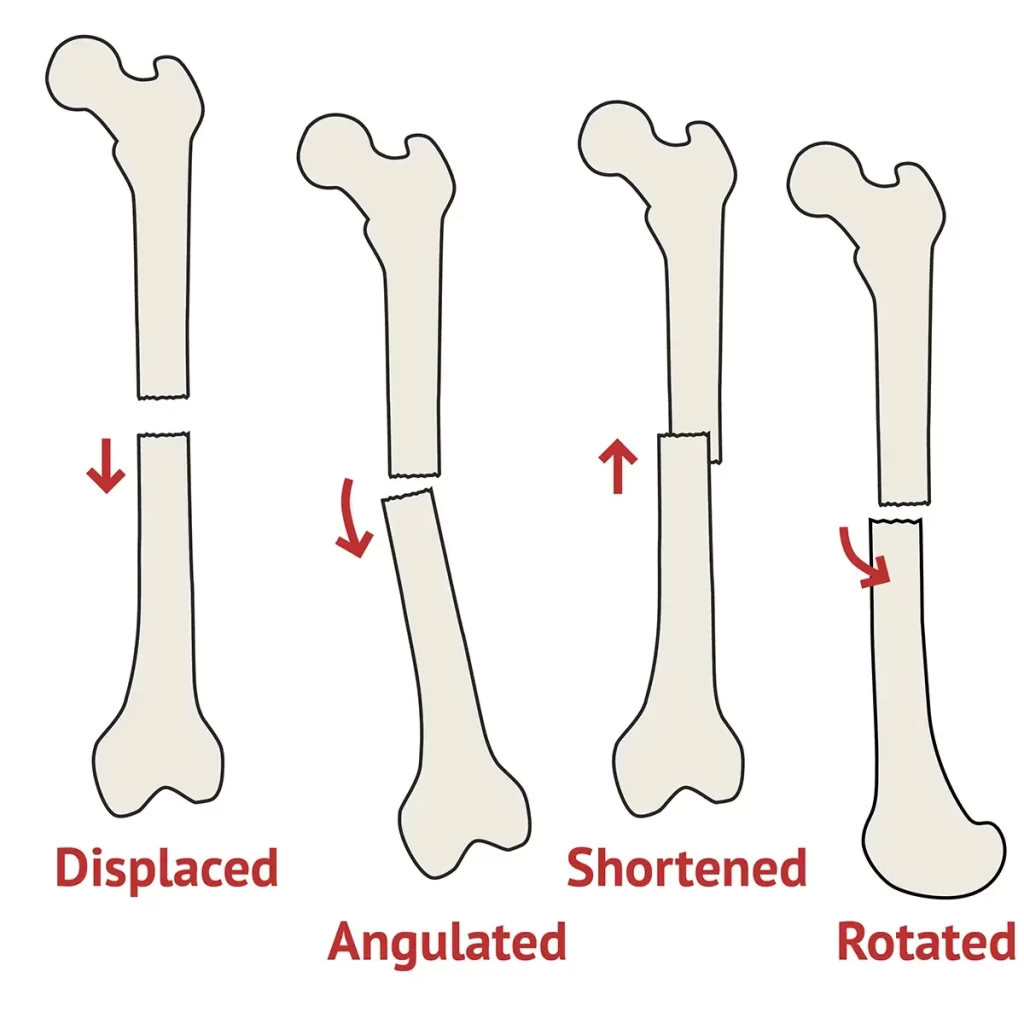
Fracture displacement can take several forms, such as angulation, rotation, change in bone length, and alignment loss.
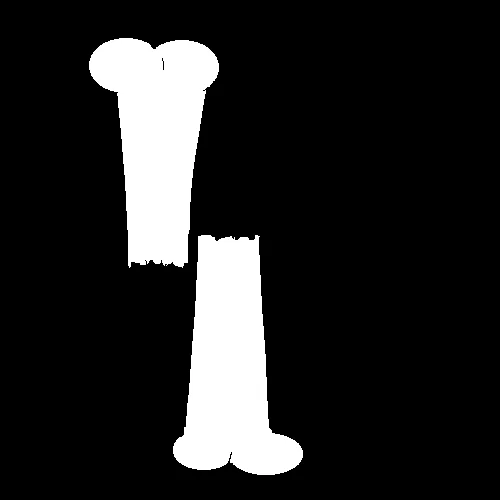
Loss of alignment -‘displacement’ Of Bone
The loss of alignment along the long axis of a bone is commonly referred to as “displacement.” There is typically some degree of angulation, rotation, or alteration in bone length that goes along with displacement, or loss of alignment.
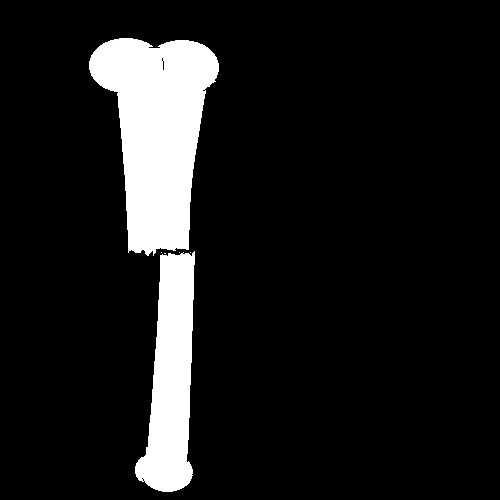
Shortening Of Bone
The distal fracture component migrates proximally, resulting in a reduction in the total length of the bone. Compared to a transverse fracture, which must first be completely “off-ended,” an oblique fracture can be shortened more easily.
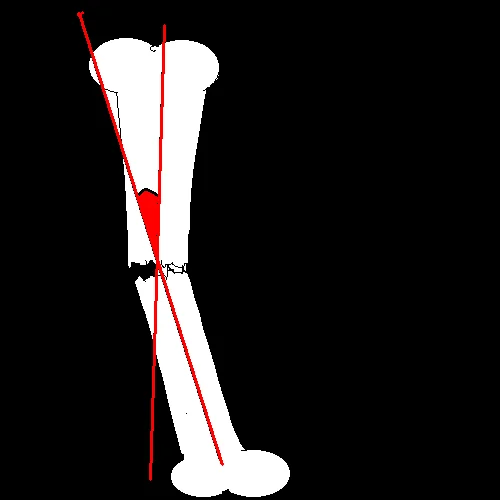
Angulation Of Bone
The orientation of the distal bone and the degree of angulation to the proximal bone should be mentioned to explain fracture angulation.
One might refer to lateral angulation as “valgus” and medial angulation as “varus.”
Rotation Of Bone
An external or internal rotation may result from a lengthy bone fracture.
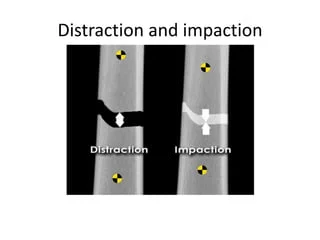
Distraction and Impaction Of Bone
Distraction (widening) of the parts of the bone causes a fracture that increases total bone length.
The fracture is impacted if the bone shortens without becoming misaligned. Each component’s bone material is pressed into the other.
Different B/W Displaced & Undisplaced Fracture
The way that bones shatter in displaced and nondisplaced fractures is different. Displaced fractures are out of alignment, although nondisplaced fractures do not always result in a complete fracture of the bone. Surgery is more likely when there is bone misalignment.
There are four main types of broken bones: nondisplaced, displaced, open, and closed. Depending on the damage, these categories are followed by many kinds of breaks. Fractures to the hands, wrists, and arms are prevalent in all ages, however, they can range in severity. Explained below are displaced and nondisplaced.
Displaced Fractures
Displaced fractures are typically more complicated because the bones are misaligned or may be fragmented. The fractured ends do not line up properly, and the broken bone snaps out of position. A fractured wrist from a violent fall might push the shattered radius closer to your body, resulting in an oblong fragment of bone pushing your skin with brute force. These fractures can be exceedingly painful because they may be visible through the skin.
Open and closed displacement fractures merely indicate that the skin is either intact or broken through. If the bone has punctured the skin, you should contact a doctor immediately. It’s crucial to look for bleeding on your wrist or arm since an open fracture has the potential to break the skin and subsequently recede into the body.
Although fractures are more common in youngsters, people’s bones become more prone to breaking as we age. Due to their weak bones, older folks are more vulnerable to falls. A comminuted fracture can happen when the bones break into several fragments after a fall. For an aged adult, this is far more problematic than it is for a toddler, who should be able to recover rather quickly.
Fractures can range in severity from very serious to dangerous complications if improperly managed, depending on the location and subtype. It is possible to sustain harm to the blood vessels, nerves, or surrounding tissue by infection. Osteomyelitis, a bone infection, is even worse. A fractured bone will mend, but complications that arise from delaying getting help cannot. If you think you may have fractured your wrist or arm, it is always preferable to get to the closest emergency facility or give a doctor a call.
Nondisplaced Fractures
Nondisplaced fractures do not shift out of alignment and are frequently closed. Because the bone cracks but does not break completely through, they are commonly referred to as incomplete fractures. Broken bones can fracture parallel to the bone’s long axis, as in the case of linear fractures, rather than necessarily through the side.
Children frequently have fractured bones, and because of their young age, they heal quickly. Children frequently suffer from greenstick fractures, which are fractures in which the bone is bent but not completely broken. Children are more vulnerable to this injury because their bones are weaker and more flexible than those of an adult. They mirror the phenomenon known as “greenstick fractures,” which occur when a small green branch on a tree is attempted to be broken but instead bends rather than breaks.
Adult and pediatric distal radius fractures are among the most common injuries. They commonly happen when someone falls on an outstretched hand because the hand will instinctively try to brace itself for the blow. This may occur during a car accident while participating in sports or during a fall. Because of the break in the wrist bone, immobilization is crucial. Treatment may be impacted by a displaced or nondisplaced break. Treatment options, which include surgery or a cast, depend greatly on whether the median nerve is painful or if the ulna is also damaged. If it is not displaced, physical therapy is usually sufficient treatment, and a cast is usually sufficient.
One crucial phase in your recuperation is physical therapy. You could have problems for the rest of your life if your joints stiffen up without it. Your wrist may be cast for roughly six weeks, which is more than enough time for general weakening and muscle atrophy. It’s typical for your arm to appear skeleton when the cast is taken off. You will be equipped with the right tools in physical therapy to strengthen your wrist and get it back to normal. You can continue to increase your range of motion with your strengthening exercises even after your therapy is over.
Causes
Traumas are nearly usually the cause of bone fractures. Anything with sufficient force can break one of your bones. Among the most typical causes are:
- Car accidents.
- Falls.
- Sports injuries.
- Fall from a height.
- Trauma.
- Motor vehicle accidents.
- Direct blow.
- Child abuse.
- Stress fractures can be brought on by repetitive stresses, like jogging.
A bone can break occasionally even in the absence of trauma. Stress fractures can result from repetitive activities like jogging or sports. Similarly, overuse syndrome in your hands and arms can result from repeatedly performing the same action for an extended length of time. You have an increased risk of developing a stress fracture if you play an instrument or use your hands in the same manner every day at work.
If you have osteoporosis, your chance of breaking a bone is significantly higher. Every year, osteoporosis results in over a million fractures.
Risk Factors
Given the risk variables, fractures are primarily caused by age and gender. Compared to men, women are significantly more likely to fracture. Throughout their lives, one in two women over 50 will suffer a fracture. This is because, even in their prime (between the ages of 25 and 30), women’s bones are typically thinner and less thick than those of males. In addition, the loss of estrogen after menopause causes women to lose more bone density than men as they age. More research on males is showing that 25% of men over 50 may experience a fracture at some point in their lives.
Additional risk factors for fractures include:
Smoking
Because smoking affects hormone levels, it is a risk factor for fractures. Smoking women typically experience menopause earlier in life. Over two decades ago, smoking was identified as a risk factor for bone loss.
Since there may be other variables at play, determining the complete effect of smoking on bone health is difficult. For instance, smokers frequently have poor diets, excessive alcohol consumption, and little exercise. In summary, the majority of research suggests that smoking raises the risk of fracture. Reducing may assist, but quitting may lower the danger.
Alcohol
Excessive alcohol use might affect bone mass and shape. Long-term heavy drinking throughout a person’s formative years might degrade bone quality and raise the possibility of bone loss and fractures even after the person has quit drinking. A formal study on the relationship between alcohol use and other factors like smoking, exercise, and diet is still lacking, however, it seems that consuming more than three drinks per day hurts vitamin D metabolism and falls risk.
Steroids
To treat chronic inflammatory diseases such as rheumatoid arthritis, inflammatory bowel disease, and chronic obstructive pulmonary disease (COPD), doctors frequently administer steroids or corticosteroids.
Regretfully, using them in greater amounts can often lead to fractures and bone loss. These unfavorable side effects are dose-dependent and linked to steroids’ capacity to reduce calcium absorption in the gastrointestinal tract, impede bone growth, and enhance calcium loss through urine. Steroid use accelerates the loss of bone.
Rheumatoid Arthritis
The body targets healthy cells and tissues surrounding the joints in this crippling autoimmune illness, which affects women two to three times more frequently than men. The outcome is severe joint and bone loss.
Prednisone is one example of a steroid that can make life easier, but as we’ll explore under “steroids,” it can also cause bone loss. To make matters more complicated, decreased activity due to pain and poor joint function speeds up bone loss and fracture risk.
Diabetes
Although the exact cause of this is unknown, people with Type 1 diabetes frequently have inadequate bone density. When a child’s bone mass is developing, Type 1 diabetes usually develops. Some patients also have celiac disease. Falls and accompanying fractures can be exacerbated by diabetes, which frequently coexists with visual issues and nerve loss.
Even though Type 2 diabetes usually develops later in life, bone density is usually higher than Type 1 diabetes; yet, high blood sugar levels can cause metabolic changes that negatively impact bone quality. Poor vision, nerve damage, and inactivity can all contribute to falls.
Other Chronic Disorders
Bone loss is frequently associated with Crohn’s disease, ulcerative colitis, and celiac disease; these conditions can accelerate bone loss if steroids are taken frequently and as needed. The gastrointestinal tract’s decreased capacity to absorb enough calcium to build and maintain strong bones is a factor shared by all of these disorders.
Thirty to sixty percent of those suffering from inflammatory bowel disease may also have reduced bone density, according to the Crohn’s and Colitis Foundation of America.
Previous Fracture
The chance of suffering another low-impact fracture is doubled in cases of prior fractures. Vertebral fractures, which affect the spine, are a reliable indicator of future fractures, however, they frequently happen gradually and don’t cause any discomfort.
When women get their yearly physicals, they should request an exact measurement of their height because a drop in height greater than 1½ inches may be a sign of spine fractures.
Symptoms
The symptoms vary depending on the site of the fracture, the age and general condition of the person, and the degree of injury.
However, individuals with a bone fracture frequently experience the following symptoms:
- Anguish
- Bloating
- Bruising
- Skin discoloration surrounding the afflicted area
- Abnormally angled protrusion of the afflicted area
- Not being able to bear weight on the wounded area
- Unable to relocate the impacted area
- A painful feeling in the afflicted joint or bone
- If there is an open fracture, bleeding
- A malformed or displaced limb or joint
- Gushing blood
- Severe pain
- Tiring and numbness
- Bone sticking out of broken skin
- Inability to move a limb or bear weight on the leg, or limited mobility
In more serious situations, an individual might:
- Nausea
- Faintness or Lightheadedness
- Dizziness
Diagnosis
- X-rays: An X-ray will demonstrate the extent of your bone damage and confirm any fractures.
- MRI: To obtain a comprehensive image of the damage to your bones and the surrounding tissue, your physician may perform an MRI. On an MRI, the ligaments and cartilage that surround your bones will also be revealed.
- CT-Scan: Compared to an X-ray, a CT scan will offer your doctor or surgeon a more precise image of your bones and the surrounding tissue.
- Bone scan: Physicians utilize a bone scan to detect fractures that are not visible on an X-ray. This scan can assist in locating some fractures, but it takes longer—usually requiring two visits spaced four hours apart.
Treatment
The type of fracture, its etiology, and the extent of bone injury all influence the course of treatment.
Non-Surgical Treatment
Managing pain and any swelling in the affected area may be part of the initial treatment for a fracture. The majority of fractures are treated by realigning the fractured bone and keeping it there until it heals. Possible course of treatment:
- Analgesic drugs
- Immobilization with a cast or splint
- A useful brace or cast that permits a restricted range of motion for neighboring joints
Before splinting or casting, the fractured bones may need to be corrected in the case of a displaced fracture. In a hospital setting, patients with more serious fractures might be sent to an orthopedic specialist for care.
External fixation, which holds the bone or bones in place until they heal using an outside metal rod and pins, may be necessary for severe or many fractures. It is also possible to utilize internal fixation tools, such as screws, rods, or plates, to keep the bone in its ideal position while it heals.
Depending on the severity of the damage, fractures can heal in a few weeks to a few months. Physical therapy is frequently advised to restore normal muscle strength, range of motion, and flexibility during the recovery process.
Immobilization
You may only require a splint or cast if your fracture is minor and your bones have not moved significantly out of place. The typical duration of splinting is three to five weeks. You’ll probably need a cast for a longer period—six to eight weeks, if necessary. You’ll probably want more X-rays in both situations to ensure that your bones are healing properly.
Closed Reduction
A closed reduction is necessary to fix (realign) more severe breaks in your bones. Your healthcare professional will physically push and pull on the outside of your body to realign the fractured bones inside of you during this non-surgical process.
One of the following will be given to you to keep you from experiencing discomfort during the procedure:
- To make the region around your fracture numb, apply a local anesthetic.
- Sedatives to help you unwind overall.
- During the procedure, you will be put to sleep using general anesthesia.
Your healthcare practitioner will place you in a cast or splint following the closed reduction.
Surgical Treatment
Surgery is necessary for certain bone fractures. The method your surgeon uses will depend on the kind of fracture you have and the extent of the damage to your bones.
Internal Fixation
Your surgeon will realign (set) your bones to their correct position and then secure them there to allow them to heal and grow back together. Usually, they perform an internal fixation, which is a procedure where your surgeon inserts tiny metal pieces into your bone to stabilize it as it heals. To allow your bone to mend completely, you will need to minimize how much you use that area of your body.
Techniques for internal fixation consist of:
- Rods: A rod that extends from the bottom through the middle of your bone.
- Plates and screws: To keep the parts together in situ, metal plates are screwed into your bone.
- Pins and wires: Too-small bone fragments are secured in place by pins and wires. Usually, they are utilized in conjunction with either rods or plates.
Some people have these implants in them permanently. It may require more procedures to eliminate them.
External Fixation
Perhaps you require an external fixing. To attach the screws to a brace or bracket that surrounds the bone outside of your body, your surgeon will drill holes in your bone on either side of the internal fracture. Usually, this is a stopgap measure to stabilize your fracture and allow it to heal before receiving an internal fixation.
Arthroplasty
Should you break a joint (e.g., your knee, elbow, or shoulder), you may require an arthroplasty (joint replacement). The injured joint will be removed by your surgeon and replaced with an artificial joint. Metal, ceramic, or sturdy plastic might be used for the prosthetic joint. The replacement joint will move and appear just like your original joint.
Bone Grafting
If your fracture is badly displaced or if your bone isn’t mending back together as it should, you might require bone grafting. To repair your broken bone, the surgeon will introduce more bone tissue. Following that, an internal fixation is typically performed to hold the fragments together while your bone grows back. For bone grafts, there are multiple sources:
- Internally from another location within your body, typically the upper part of your hip bone.
- An outside contributor.
- A synthetic substitute component.
You will immobilize your bone following surgery. Before you can start using it as you did before your fracture, you’ll need to wear some combination of a sling, brace, cast, or brace.
Prevention
Consider the following general safety measures to assist in preventing fracture:
- When traveling in a car, always buckle up.
- Wearing the appropriate safety gear, such as helmets and other protective padding, is imperative when engaging in recreational activities like biking, snowboarding, or contact sports.
- Clear the area around stairs and walkways of anything that can trip you.
- Exercise frequently to increase your strength and balance if you have osteoporosis. This may help you fall less.
- Consult your doctor about beginning bone-building drugs and supplements (such as calcium and vitamin D).
- Make sure someone is holding the ladder when you’re on it and stay away from the top step.
FAQs
What does a bone’s displacement mean?
The loss of alignment along the long axis of a bone is commonly referred to as “displacement.” There is typically some degree of angulation, rotation, or alteration in bone length that goes along with displacement, or loss of alignment.
Will a fracture that is misplaced heal on its own?
A broken bone or fracture can truly mend itself, given the proper circumstances for the break to heal entirely. Around the fracture site, a blood clot forms. Following that, until the break heals, bone cells start to grow on the fracture line’s edges and migrate toward the break’s center.
Is surgery required for displaced fractures?
In contrast to nondisplaced fractures, which typically just require immobilization in a cast for six weeks to allow for adequate healing, displaced fractures are likely to require surgery due to the instability of the bones. In order to avoid joint stiffness and restore strength and complete range of motion, physical therapy is necessary for both treatment choices.
Is there pain associated with bone displacement?
When two bones separate at their joint, it’s called a dislocation. In addition to momentarily deforming and immobilizing the joint, this injury can be quite painful. Dislocations most frequently happen in the shoulders and fingers, although they can also happen in the elbows, knees, and hips.
Is relocating the same as displacement?
A displacement of a bone relative to the opposing bone, known as a luxation or dislocation, causes a partial loss of articulation of the opposing bone ends.
REFERENCES
- Professional, C. C. M. (n.d.). Bone Fractures. Cleveland Clinic. https://my.clevelandclinic.org/health/diseases/15241-bone-fractures
- Fractures (Broken Bones) – OrthoInfo – AAOS. (n.d.). https://orthoinfo.aaos.org/en/diseases–conditions/fractures-broken-bones/
- Introduction to Trauma X-ray. (n.d.). https://www.radiologymasterclass.co.uk/tutorials/musculoskeletal/trauma/trauma_x-ray_page3#top_1st_img
- A. (2022, November 22). Types Of Fractures: Displaced vs. Non-Displaced Fractures. Hand and Wrist Institute. https://handandwristinstitute.com/displaced-vs-non-displaced-fractures/
- FRACTURE DISPLACEMENT. (n.d.). https://emedsa.org.au/EDHandbook/trauma/Extremities/Displacement.htm
- Fracture Risk Factors – Bone Health & Osteoporosis Foundation. (2020, April 11). Bone Health & Osteoporosis Foundation. https://americanbonehealth.org/fracture/fracture-risk-factors/
- Brazier, Y. (2023, November 10). What is a fracture? https://www.medicalnewstoday.com/articles/173312#symptoms
- Fracture Diagnosis and Care | Med Diagnostics Rehab. (n.d.). https://www.meddiagnosticrehab.co/fracture-diagnosis-and-care.php