Radial Head Dislocation
What is Radial Head Dislocation?
Radial head dislocation, also known as a pulled elbow or nursemaid’s elbow, is a common injury primarily affecting young children. This injury occurs when the radius bone in the forearm slips out of its normal position at the elbow joint. It is often the result of a sudden yank or pull on a child’s forearm, typically when an adult or caregiver pulls on the child’s hand or wrist.
As a result of this sudden traction, the annular ligament around the head of the radius can become entrapped, leading to the dislocation of the radial head. While it is not usually a severe injury, it can cause immediate pain and discomfort for the child. Prompt medical attention is necessary to ensure proper treatment and to prevent further complications.
Although they can happen at any age, radial head dislocations are more frequent in children and young adults. A radial head dislocation can cause elbow joint deformity, discomfort, and edema. The elbow may also be restricted from fully moving and locked in a particular position.
Usually, radial head dislocations may be treated without surgery using closed reduction, which involves manipulating the radial head back into place. Surgery, however, could occasionally be required to fix the dislocation and stabilize the elbow joint.
Anatomy:
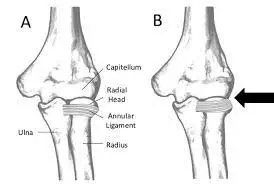
The ulna and radius are both of the bones which make up the forearm. Both of these bones join the humerus, the upper arm bone, at the elbow. These three bones combine to create the elbow joint. The top, or head, of the radius, is surrounded by the flexible, fibrous annular ligament, which joins the radius to the rest of the elbow joint.
Radial head subluxations occur when a portion of the annular ligament moves over the radial bone’s head and gets stuck in the radiohumeral joint. The signs and symptoms of radial head subluxation are due to displacement of the annular ligament.
When the bone still makes some contact with the ligament, a partial dislocation, or subluxation, develops. When there is a complete dislocation, the radius bone has been totally moved out of position.
Stabilizers—both static and dynamic—provide stability to the elbow.
- Static stabilizers (primary)
- glenohumeral joint
- the anterior bundle of the MCL
- LCL complex (includes the LUCL)
Static stabilizers (secondary)
- radiocapitellar joint
- joint capsule
- discussed flexor and extensor tendon origins
Dynamic stabilizers
- elbow-crossing muscles that provide compressive (stabilizing) force
- anconeus
- brachialis
- triceps
Causes of Radial Head Dislocation
The radial head is held stable by the annular ligament. An axial force on an extended, pronated forearm in children with subluxation causes the annular ligament to slide across the radial head. On the other hand, both children and adults can have a full radial head dislocation. The annular ligament is typically damaged in such injuries from high-force trauma. Less frequently, the radial head will slide under the annular ligament since it is still intact and attached to the lateral collateral ligament and the ulna.
Pathophysiology:
The radius and ulna are joined at both ends by the properly named proximal and distal radioulnar joints. Similar to the mandible and pelvis, it is difficult to cause damage to one side of the band without damaging the other. The separation of a radial head dislocation from an ulna fracture, commonly known as the Monteggia fracture-dislocation, must be confirmed.
The bones of pediatric patients usually have progressive changes. The ulnar bending sign can be used to evaluate if the ulna develops a bending fracture rather than a transverse ulna fracture as a result of radial head dislocation. Although uncommon in children, Monteggia fracture-dislocation does occur occasionally.
Radial head dislocation can also occur in people with neuromuscular conditions and contractures, such as cerebral palsy and brachial plexus injuries.
A complete radial head dislocation happens as a result of a high-force injury, such as a fatal vehicle crash or a fall onto an extended arm. Rarely does the radial head move on independently without resulting in more damage. The following injuries can develop from a radial head dislocation:
- Monteggia fractures
- Elbow dislocations
- Elbow fractures
- The painful trio of elbow injuries (radial head fracture, ulnar coronoid process fracture, and elbow dislocation)
- Congenital dislocation of the head of the radial bone may be present combined with other congenital defects, such as:
- Ehlers-Danlos syndrome
- Nail-Patella syndrome
- Ulnar dysplasia
- Radioulnar synostosis
- Dyschondroplasia
What is the difference between radial head dislocation and subluxation?
A radial head subluxation is damage to the elbow joint. The term “subluxation” refers to a partial dislocation, and the radial head is the top of the radius, one of the two major bones in the forearm. Subluxations of the radial head are injuries that result in partial separation of the radial head from the rest of the elbow.
The disease, which is also known as a pulled elbow, babysitter’s elbow, nursemaid’s elbow, RHS, or annular ligament displacement, may be caused by sudden pressure on the forearm. It is a common injury in children, especially those between the ages of one and four. This is due to this ligament being much more easily injured in youngsters, which raises the chance that it might slip over the radial head in the case of a sudden pulling force. The radial bone of the elbow is kept in place by this ligament.
People who have pulled an elbow try to keep the injured arm close to their body and avoid using it, typically supporting it with the other hand or their stomach. They can use arm pain as an excuse. To fix a radial head subluxation, a doctor will often just need to realign the joint; complications are uncommon.
In adults and children, complete dislocations of the radial head are extremely uncommon. If they occur, a congenital illness or a severe trauma are typically the causes. There may be symptoms, more severe than those of a pulled elbow. Full radial head dislocations frequently occur together with other arm injuries, such as a forearm fracture. Therefore, any associated illnesses, that may necessitate surgery, are the main focus of treatment.
Differential diagnosis of radial head dislocation:
- Pulled elbow
- Babysitter’s elbow
- Nursemaid’s elbow
- Partial dislocation of the radial head
- Annular ligament displacement
- RHS
- Pronation Dolorosa
Complication of radial head dislocation:
- Osteoarthritis
- Chronic pain
- Reduced mobility of the elbow joint
- When the dislocation is continuously ignored, radial head deformity develops.
- Early stiffness
- Early, active ROM can help avoid this from occurring as loss of terminal extension is the most frequent consequence following closed treatment of a minor elbow dislocation.
- After the inflammation is no longer static, gradual splinting may be beneficial.
- often between 6-8 weeks after surgery
Varus posteromedial instability
- LCL damage and a fractured anteromedial facet of the coronoid
- For the anteromedial facet to operate properly and to avoid arthrosis, strong fixation is essential.
Neurovascular injuries
- Rare brachial artery injuries are frequently related to open dislocations.
- Stretch is often the cause of ulnar nerve damage
- median nerve injury (rate) typically associated with brachial artery injury
Compartment syndrome
- Damage to the articular surface
- Recurrent instability
Heterotopic ossification
Excision could be required to improve the elbow range of motion.
Contracture/stiffness
correlated with immobilization beyond 3 weeks
Signs and symptoms of radial head dislocation:
Because newborns and young children are most frequently affected by pulled elbows and subluxation of the radial head, it’s important to be alert for any of the following symptoms that might point to this injury:
holding the injured arm in a close position to the body
Maintaining the injured arm in a little bend while you’re grasping it, usually between 15-20 degrees
Using the other hand to support the weight on the injured arm
Reluctance to utilize the arm
refusal to fully flex or extend the arm
Usually, poorly localized wrist, arm, or elbow pain that is dull, pushing, or painful
Although a pulled elbow usually is painful, particularly at first, pain is not always the primary sign that an injury has occurred. A child could act normally in other situations, save for aversion to utilizing the injured arm.
Notably, a pulled elbow rarely results in bruising, edema, or other types of cosmetic damage to the afflicted region.
Symptoms of full radial head dislocations are often similar to those of pulled elbows but are a little more severe. For example, the affected person could continue to flex the injured arm, but at a more acute 90-degree angle. Furthermore, they can experience more discomfort and be less inclined to use their arm.
Radial head subluxations do not result in apparent elbow swelling, although full dislocations usually occur. This is a crucial sign that differentiates the two illnesses.
Risk factors of radial head dislocation:
The radial bone can sublux quite fast in young children because the annular ligament that supports the elbow bones in place is smaller in children than in adults. A sudden tug on the child’s arm, which forces the bone to rupture out of its usual position, is the most prevalent reason for this injury.
There are a number of possible risk factors for radial head subluxation or a stretched elbow.
pulling a youngster by the arm and moving forward
Retaining a child’s arm as they withdraw
holding the arm of a youngster or catching them as they fall
using one’s arms to swing or lift a child
The arm of a youngster being inserted through a sleeve
It’s important to know that falls are more likely to result in fractures or breaks than they are to result in pulled elbows.
By the time a child is five years old, the annular ligament in the elbow is usually powerful and tight enough to prevent radial head subluxations from occurring frequently.
Whole radial head dislocations frequently occur in either an accident or a congenital condition that occurs from birth.
Imaging of radial head dislocation:
Radiographs
recommended views
AP and lateral views
check the alignment of the joints, especially following reduction attempts.
oblique views
assess for associated periarticular fractures
CT scan
indications
suspicion of complex injury pattern
useful to identify associated periarticular fractures
The primary diagnostic procedure for radial head subluxation or dislocation is a clinical examination performed by a clinician. Typically, this evaluation consists of:
Examining the afflicted arm physically
Discussion of the signs and symptoms
Review of medical background
Before evaluating if a partial or total dislocation of the radial head is the origin of the symptoms, a doctor must rule out other disorders that may present with similar symptoms. These circumstances include:
Broken radial head:
various fractures that might affect mobility in the upper limbs including those to the ulna, clavicle, wrist, hand, and various areas of the elbow.
Hand soft tissue injuries
Other conditions, such as arthritis or bone diseases like osteomyelitis may restrict the range of motion in the arm.
Neurological causes:
If the patient shows normal clinical signs of subluxation or pulled elbow, an X-ray is often not required. This is because a subluxation is just a partial dislocation and is rarely seen on an X-ray. Although a radiograph might be taken,
Suspected is a complete radial head dislocation.
A fracture and various associated injuries are suspected.
Unusual or unclear symptoms
The initial attempts to correct the subluxated joint are unsuccessful.
An ultrasound examination might also be carried out in particular conditions to accurately assess the damage and avoid misunderstanding. Ultrasounds can be a useful diagnostic tool when diagnosing young children who might not be able to communicate their problems clearly.
MRI scans:
MRI scans can also be used to assess ligament damage in the region and confirm the diagnosis. The only persons to whom this is frequently advised are those who have repeatedly dislocated their elbows and may thus have significant tissue damage.
Plain radiograph:
In almost every single traumatic dislocation case, the radial head is displaced anteriorly. The line that should always cross the capitellum when drawn along the radial neck, the radiocapitellar line, is misplaced in lateral projection and is the most obvious. Where this is missing, radial head dislocation has taken place. If it is still intact, the ulna is probably twisted.
It is essential to assess the elbow swelling areas in young children to ensure that no further fractures, such as lateral condylar or epicondylar fractures, have happened. The shorthand CRITOE might be used to recall the ossification centers.
In those with contracture-related dislocation (such as cerebral palsy), the pronator teres muscle shortens, causing the forearm to pronate and the radial head to dislocate posterolaterally.
Depending on which muscles are implicated, brachial plexus palsy-related dislocations can happen either anteriorly or posterolaterally.
Treatment of radial head dislocation and subluxation:
Several factors, such as the following, may affect the precise course of treatment for radial head subluxation or dislocation.
Whether the injury is a complete dislocation or a subluxation
Any possibility of injuries, such as fractures, that may exist
Whether it impacts a child or an adult
Whether something serious or a congenital problem caused the sickness
Non-operative therapy:
The first step in treatment for individuals without any associated injuries is frequently an effort to manually guide the radial head back into the joint (closed reduction). Especially when there are pulled elbows, doctors can commonly perform closed reductions quickly and effectively.
If a pulled elbow in a baby or child is suspected, it might not even be necessary to provide sedatives or medications before attempting to move the bone back into place. However, medications may be given throughout the closed reduction operation if the patient is an adult and if the injury is a full dislocation.
When the radial head settles into position, it could make a slight clicking sound. Within 30 minutes of being reset, it is typical for the injured person to regain mobility and normal arm function. Once the function has returned, often no more treatment is required. A sling or cast may be advised to support or immobilize the arm while it heals.
After a few days, more testing, such as X-rays, may be required if a closed reduction doesn’t work, the patient’s pain remains, or they are still unable to fully use their arm. If it doesn’t work, surgery can be required.
Surgical treatment:
It may be recommended to do an open reduction, a surgical operation to realign the radial head, on individuals with further injuries, or for whom closed reduction techniques have failed. Adults are more prone than children to require surgical therapy due to their less flexible joints and the possible difficulties in readily recovering them.
If there are further injuries, those may be treated during surgery rather than the radial head itself. For instance, the radial head frequently returns to its previous position on its own when the ulna, or forearm bone, breaks and mended. To keep the bone’s normal length and position following a fracture, plates, and screws may be used to fix the ulna in place. This reduces the possibility of radial head dislocation happening again in the future.
Because radial head subluxations and dislocations are complicated injuries that may display symptoms that are similar to those of other injuries and can give rise to a chronic condition, medical professionals can ignore or misdiagnose them. In the event that the problem goes untreated for more than three years, the radial head may develop abnormalities. This is why previously undetected radial head subluxations or dislocations are usually treated surgically.
Initial non-surgical treatment is usually used to treat radial head dislocation caused by a congenital abnormality. If surgery is required, it is often done in adulthood to alleviate pain, limitations on movement, or cosmetic concerns.
Summary:
The forearm’s upper radius bone, the radial head, can become displaced from its original placement at the elbow joint. This condition is known as radial head dislocation. It can happen due to a fall, an injury to the elbow, or an effective forearm twist.
Although they can happen at any age, radial head dislocations are more frequent in children and young adults. A radial head dislocation can cause elbow joint deformity, discomfort, and edema. The elbow may also be restricted from fully moving and locked in a particular position.
Usually, radial head dislocations may be treated without surgery using closed reduction, which involves manipulating the radial head back into place. Surgery, however, could occasionally be required to fix the dislocation and stabilize the elbow joint.
FAQ
What is radial head dislocation?
This injury includes a rupture of the interosseous membrane, a ligament-like sheet of tissue that stabilizes the bones in the forearm, a fracture of the radial head, and dislocation of the joint that connects the two forearm bones, the distal radioulnar joint.
How do you treat a dislocated radial head?
However, during adulthood, open surgery is usually required for repair. While there are a number of surgical options available to treat chronic radial head dislocation, open reduction with plate and screw fixation or intramedullary ulna fixation and annular ligament repair are the two treatments that are most frequently employed.
How do you fix a dislocated elbow?
Simple elbow dislocations are treated with initial movement exercises after 1 to 3 weeks of immobilization in a splint or sling.
What is another name for a radial head dislocation?
One of the most common upper-extremity injuries in newborns and young children who consult the emergency room is radial head subluxation, often known as pulled elbow or nursemaid’s elbow.
How long does it take for a radial head to heal?
A radial head or neck fracture may require six weeks to heal completely. Avoid lifting heavy items or holding a lot of weight at this period. After your injury has healed for at least 6 weeks, you should not start contact sports.
Does a dislocated elbow Need surgery?
Simple dislocations may generally be repaired without surgery during an emergency department visit. However, if a fracture and torn tissues are present, surgery will probably be necessary to fix the injury and reduce the likelihood of elbow instability.