Hip Bone
Overview
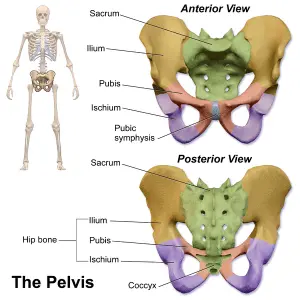
The hip bone, also called the innominate bone, pelvic bone, or coxal bone, is an unevenly shaped, both sides of bone of the bony pelvis. It is a compound structure comprising the three smaller bones of the pubis, ischium, and ilium.
The ischium is situated posteroinferiorly, the pubis or pubic bone creates the anterior portion of the hip bone, and the ilium is the biggest and most superior portion of the bone.
In children, the three parts of the hip bone only have a cartilage connection between them after developing independently. During puberty, they fully fuse to form the compact and complex hip bone.
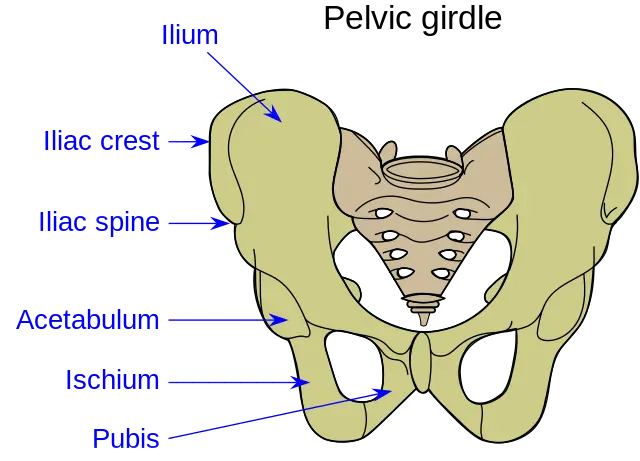
The acetabulum, a cup-shaped and deep socket upon the lateral surface of the bone that articulates at the femoral head at the hip joint, is the focal point of this union.
The large obturator foramen is located anteroinferior to the acetabulum. The pelvic girdle is composed of the left and right hip bones. The sacrum and coccyx make up the pelvic spine, which completes the bony pelvis posteriorly. As a weight-bearing structure, the bony pelvis joins the axial bone network to the lower limbs.
Structure
The pubis, ischium, and ilium combine to form the hip bone.
Hyaline cartilage separates these three parts at birth. They connect in the acetabulum at a Y-shaped cartilage segment. The three parts will have merged by the time adolescence ends and will have solidified by the time a person is 25 years old.
The pubic symphysis is where the two hip bones join. The hip bones make up the pelvis, together in order with the sacrum and coccyx.
Ilium
The most superior part of the hip bone is the ilium, a blade-shaped bone. The body and wing are its two main components (wing).
The wing is the superior expanded portion of the bone with four borders and three surfaces, whereas the body is the more tiny, inferior portion that aids in the formation of the acetabulum.
Borders
There are four distinct borders to the ala of the ilium: the superior (iliac crest), anterior, posterior, and medial.
- Superior border
Many muscles along with fascia of the abdominal wall, back, and lower limbs attach to the prominent iliac crest, which forms the superior border. It terminates at the posterior superior iliac spine and the anterior superior iliac spine, respectively.
The inguinal ligament attaches to the anterior superior iliac spine, which can be felt with ease. Although it cannot be felt, the posterior superior iliac spine is typically visualized as a dimple over the medial gluteal region (buttock).
The inner and outer lips of the iliac crest are divided by an intermediary zone. The iliac tubercle, a prominence on the outer lip, is located close to the anterior end of the crest.
- Anterior Border
From the anterior superior iliac spine to the acetabulum, the ilium’s anterior border is located. Just above the acetabulum, it has the anterior inferior iliac spine.
The proximal portion of the iliofemoral ligament and the straight head of the rectus femoris muscle attach to this spine.
- Posterior Border
Starting at the posterior superior iliac spine, the posterior border of the ilium extends to the posterior border of the ischium. The superior portion of the greater sciatic notch is influenced by this border, which also houses the posterior inferior iliac spine. The ischial spine and posterior ischial border complete this notch inferiorly. The greater sciatic notch forms the great sciatic foramen, an enclosure that is formed by the sacrotuberous and sacrospinous ligaments.
- Middle border
The sacropelvic surface and the iliac fossa are separated by the medial border. This border includes the curved line, which extends through the auricular surface to the region of the acetabulum anteroinferiorly. It is rounded and smooth. It designates the split between the ilium’s body and wing.
Surface
The iliac fossa, sacropelvic surfaces, and gluteal surfaces are the three bony surfaces that the ilium’s borders encircle.
- Gluteal surface
There are multiple points of attachment for the gluteal and thigh muscles on the posterolateral surface of the gluteus. Its borders are as follows: the anterior and posterior borders, the iliac crest, and the upper portion of the acetabular margin on the inferior side.
The anterior, posterior, and inferior gluteal lines are three curved ridges on this surface. From the iliac crest tubercle toward the greater sciatic notch, the anterior gluteal line moves obliquely along the gluteal surface.
The posterior inferior iliac spine is anterior to the posterior gluteal line, which descends from the crest’s external lip.
The acetabular margin is inferior to the inferior gluteal line. The supraacetabular groove, which is the attachment point for the reflected head of the rectus femoris muscle, is located between the inferior gluteal line and the acetabular margin.
- Sacropelvic surface
The sacropelvic surface, which consists of the iliac tuberosity, auricular, and pelvic surfaces, is located posterior to the iliac fossa on the medial aspect of the ilium.
The sacroiliac joint is formed by the articulation of the auricular surface, an ear-shaped surface, with the sacrum. The posterior part of the sacropelvic surface, known as the iliac tuberosity, is an elevated, roughened region that serves as a point of attachment for the sacroiliac joint’s ligaments.
Anteroinferior to the auricular surface, the narrow pelvic surface forms part of the lateral wall of the lesser pelvic cavity.
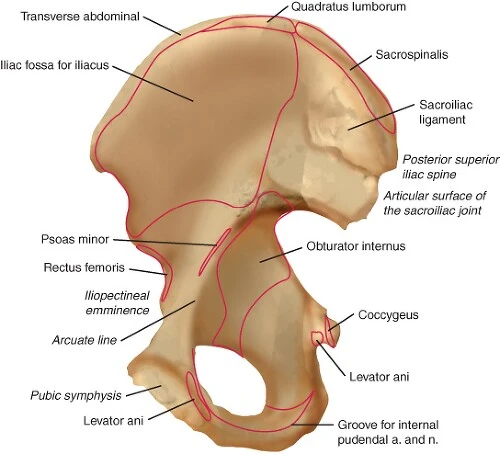
- The iliac fossa
The large curved anteromedial surface of the ilium’s wing is known as the iliac fossa.
This fossa, which forms a smooth posterolateral wall that covers the greater pelvis, is bordered by the iliac crest’s inner lip on the superior side, the arcuate line on the inferior side, the ilium’s anterior border on the anterior side, and the medial border, which divides it from the sacropelvic surface, on the posterior side.
The ischium
The inferior and posterior portion of the hip bone is called the ischium. The body and the ramus are its two main sections.
Body
The biggest part of the bone is called the ischium’s body. It contributes to the acetabulum and extends superiorly to connect the ilium as well as the superior ramus of the pubis.
Ramus
The ischium’s ramus joins the inferior pubic ramus anteromedially after extending from the inferior aspect of the body. The ischiopubic ramus, the inferior border of the obturator foramen, is made up of these bony rami combined.
Ischial tuberosity
The ischial tuberosity, the most noticeable characteristic of the ischium, is located on the posteroinferior aspect of the ischial ramus. It supports the body’s weight when seated and serves as an attachment point for the sacrotuberous ligament, the adductor magnus muscle, and the posterior thigh muscles (semimembranosus, semitendinosus, and long head of biceps femoris).
Ischial spine
The ischial spine, a conical prominence pointing posteromedially, is visible on the posterior margin of the ischium. It is where the sacrospinous ligament attaches. The lesser sciatic notch is a tiny “C” shaped concavity located directly below the ischial spine.
The sacrotuberous and sacrospinous ligaments transform the lesser sciatic notch into the less sciatic foramen.
Pubic
The pubis, or pubic bone, is the anterior and inferior portion of the hip bone. The smallest part of the hip bone is this one. It is separated into the superior ramus, inferior ramus, and body.
The two rami expand posterolateral from the body, which is located anteromedially. The inferior ramus keeps going inferiorly to connect to the ischial ramus, while the superior ramus expands superiorly to the acetabulum.
Note that although this is not in line with the Terminologia Anatomica, some sources regard the body of the pubis as the superolateral portion of the bone that aids in the formation of the acetabulum.
Body
There are three surfaces on the pubic body: anterior, posterior, and symphysial (medial). The pubic crest refers to the rounded upper border. The pubic tubercle, which serves as an attachment point for the medial end of the inguinal ligament, is where this crest ends laterally. The body’s symphyseal surface articulates with its counterpart within the pubic symphysis by facing medially.
Superior pubic ramus
The superior pubic ramus connects the ischium and ilium at the acetabulum, extending posterolaterally from the body.
Its cross-section is triangular, and its three surfaces and three borders are all the same.
- The anterior/pectineal surface
From the pubic tubercle up to the iliopubic eminence (where the pubis and ilium converge), the anterior/pectineal surface of the superior pubic ramus is located.
The pecten pubis, or pectineal line, is located posteriorly, and the round obturator crest, located anteriorly, limits this surface.
The pubic crest and the arcuate line of the ilium are both continuous anteromedially with the pecten pubis and posteromedially with it.
- Obturator surface
The obturator crest and the acute inferior border surround the posteroinferiorly facing obturator surface. The obturator groove crosses this surface.
- Pelvis surface
The pubis’s smooth pelvic surface faces posterosuperiorly. Its boundaries are the inferior border of the superior pubic ramus below and the pecten pubis above.
Inferior pubic ramus
The inferior pubic ramus joins the ischial ramus by projecting laterally and posteroinferiorly from the pubic body. Adductor magnus/minimus/brevis and gracilis are two of the thigh’s adductor muscles that attach to it.
Acetabulum
The acetabulum, one of the hip bone’s most noticeable landmarks, is located on its lateral aspect. It has an anteroinferior socket-shaped articular surface that articulates with the femur head to form the hip joint.
The three elements that make up the hip bone unit at the acetabulum, each having a role in its development.
There are several anatomical characteristics of the acetabulum itself. The articular surface of the femur head that resembles a moon is called the lunate surface. The non-articular part of the acetabulum located centrally is called the acetabular fossa.
The “C” shaped acetabular margin, which ends inferiorly at the acetabular notch, serves as the acetabulum’s border.
The transverse acetabular ligament completes the acetabular margin inferiorly and the cartilaginous acetabular labrum highlights the acetabular margin.
The obturator foramen
The obturator foramen is a large opening situated anteroinferior to the acetabulum, which is bordered by the pubis and ischium.
The obturator membrane, a flat connective tissue membrane, covers the majority of this foramen.
The obturator nerve, artery, and vein travel between the pelvic cavity and the medial compartment of the thigh via a narrow obturator canal that is located superiorly between the membrane and neighboring bone.
Pelvic crest
A continuous oval ridge of bone, the pelvic brim runs along the sacral promontory, sacral alae, pubic crests, arcuate lines, and pubic symphysis.
Pelvic inlet and false pelvis
The area above the pelvic brim is known as the false pelvis, and it is surrounded by the sacral promontory and lumbar vertebrae posteriorly, as well as the ilia’s alae laterally.
The area below the pelvic brim that is nearly totally encircled by bone is known as the true pelvis.
The opening that the pelvic brim defines is known as the pelvic inlet. The pelvic inlet’s broadest dimension runs along the frontal plane, from left to right.
The edge of the actual pelvis is known as the pelvic outlet. The pubic arch forms its anterior boundary, the ischia its lateral border, and the sacrum and coccyx its posterior boundary.
Development and sexual dimorphism
Eight centers make up the ossified hip bone:
Three primary, one for each of the ischium, pubis, and ilium; five secondary, one for the iliac crest; the anterior inferior spine (in males more often than in females), the ischium’s tuberosity; the pubic symphysis (in females more often than in males); and a few for the Y-shaped piece exactly at the bottom of the acetabulum.
The locations of the centers are as follows:
approximately the eighth or ninth week of fetal life, in the lower part of the ilium, right above the greater sciatic notch; approximately the third month, in the superior ramus of the ischium; and between the fourth and fifth months, in the superior ramus of the pubis.
The crest, the base of the acetabulum, the ischial tuberosity, and the inferior rami of the ischium and pubis are still cartilaginous at birth, making the three main centers relatively distinct.
The inferior rami within the pubis and ischium are nearly entirely fused by bone by the seventh or eighth year.
The three main centers have grown into the bottom of the acetabulum by the thirteenth or fourteenth year, and are now separated from one another by a Y-shaped section of cartilage that shows signs of ossification, frequently by two or more centers. One of these, the os acetabuli, forms the pubic part of the acetabulum and appears between the ilium and pubis around the age of twelve.
It fuses with them at the age of eighteen. This Y-shaped part then intervenes to join the ischium and ilium and, finally, the pubis and ischium.
Ossification begins in each of the other parts at puberty and they join the rest of the bone within the ages of twenty-fifth and twenty-fifth. The pubic tubercle and ischial spine, as well as the pubic crest and angle, are often found to have separate centers.
The baby’s ease of passage during childbirth may be influenced by the proportions of the female hip bone.
Muscle attachment
All of the muscles that work on the hip joint are referred to as hip muscles. We’ll examine the inner hip muscles and the gluteal muscles in this section.
Gluteal muscles
The buttocks’ distinctive curve is a result of the gluteal muscles. The gluteus maximus, gluteus medius, gluteus minimus, and tensor fasciae latae are the four gluteal muscles, and they are situated on the posterior side of the hip bone. They are all incredibly strong hip flexors and extensors, which is why the human body’s erect posture depends on them.
- Gluteus Maximus
- Origin: Gluteal surface of the ilium (behind the posterior gluteal line), Lateroposterior surface of sacrum and coccyx, fascia thoracolumbar, The ligament of Sacrotuberous
- Insertion: Gluteal tuberosity of femur, Iliotibial tract
- Innervation: L5, S1, S2, inferior gluteal nerve
- Function: Thigh abduction (superior part), Thigh adduction (inferior part), Thigh extension, and Thigh external rotation
- Gluteus medius
- Origin: Between the anterior and posterior gluteal lines, on the gluteal surface of the ilium
- Insertion: The lateral aspect of the femur’s greater trochanter
- Superior gluteal nerve innervation (L4-S1)
- Hip joint function: stabilization of the pelvis; thigh abduction and internal rotation (anterior part);
- Gluteus minimus
- Origin: Between the anterior and inferior gluteal lines, on the gluteal surface of the ilium
- Insertion: The front side of the femur’s greater trochanter
- Superior gluteal nerve innervation (L4-S1)
- Functions include anterior thigh internal rotation, thigh abduction, and pelvic stabilization.
- Tensor fasciae latae
- Origin: The outer lip of the anterior iliac crest and the anterior superior iliac spine (ASIS)
- Placement: Iliotibial Canal
- Superior gluteal nerve innervation (L4-S1)
- Functions: Knee joint: Leg external rotation, (Weak leg flexion/extension); Hip joint: Thigh internal rotation, (Weak abduction); stabilizes the knee and hip joints
Internal hip muscles
The iliacus, psoas major, psoas minor, obturator externus, obturator internus, superior and inferior gemelli, piriformis, and quadratus femoris are the nine inner hip muscles, which are located at the anterior side of the pelvis. Although nine might seem like a lot, these muscles are crucial for producing the variety of hip motions that athletes, dancers, and music enthusiasts use.
Origin of Iliacus: Iliac fossa
- Iliacus
- Origin: Iliac fossa
- Insertion: The femur’s lesser trochanter
- Femoral nerve innervation (L2-L4)
- Hip joint function: thigh flexion and external rotation
- Psoas major
- Origin: Transverse processes of L1–L5 vertebrae, intervertebral discs between T12–L4, and vertebral bodies of T12–L4
- Insertion: The femur’s lesser trochanter
- Innervation: Lumbar plexus branches (L1-L3)
- Hip joint function: thigh/trunk flexion, external rotation of the thigh, lateral flexion of the trunk
- Psoas minor
- Origin: The T12 and L1 vertebrae’s vertebral bodies
- Insertion: Pectineal line of pubis, iliopubic eminence
- Innervation: Lumbar plexus branches (L1-L3)
- Hip joint function: thigh/trunk flexion, external rotation of the thigh, lateral flexion of the trunk
- Obturator externus
- Origin: The bone boundaries of the obturator foramen and the anterior surface of the obturator membrane
- Insertion: The femur’s trochanteric fossa
- Innervation: Nerve of the obturator (L3, L4)
- Hip joint function: thigh abduction (from a flexed hip) and external rotation; stabilizes the head of the femur in the acetabulum
- Obturator internus
- Origin: The posterior surface of the obturator membrane and the ischiopubic ramus
- Insertion: The femur’s medial surface of the greater trochanter
- Innervation: L5-S2 nerve innervates the obturator internus.
- Hip joint function: thigh abduction (from a flexed hip) and external rotation; stabilizes the head of the femur in the acetabulum
- Superior gemellus
- Origin: Ischial vertebrae
- Insertion: Greater trochanter’s medial surface (through the obturator internus tendon)
- Innervation: L5-S2 nerve innervates the obturator internus.
- Hip joint function: thigh abduction (from a flexed hip) and external rotation; stabilizes the head of the femur in the acetabulum
- Inferior gemellus
- Origin: tuberosity in the schia
- Insertion: Greater trochanter’s medial surface (through the obturator internus tendon)
- Quadratus femoris nerve innervation (L4-S1)
- Hip joint function: thigh abduction (from a flexed hip) and external rotation; stabilizes the head of the femur in the acetabulum
- Origin: Gluteal surface of the ilium (close to the posterior inferior iliac spine), Anterior surface of sacrum (between S2 and S4) The ligament of Sacrotuberous
- Insertion: The top of the femur’s greater trochanter
- Innervation: Piriformis nerve (S1–S2)
- Function: external rotation of the thigh; stabilizes the head of the femur in the acetabulum
Thigh muscle
The area between the hip and knee joints is called the thigh. These particular leg muscles are extremely well-defined in soccer players; they resemble a walking anatomy atlas for thigh muscles. There are three compartments in the thigh muscles:
Flexors of the hip joint and extensors of the knee joint are examples of anterior thigh muscles.
Extensors of the hip joint and flexors of the knee joint are examples of posterior thigh muscles.
Hip joint adductors are the muscles of the medial thigh.
The sartorius and the four quadriceps muscles—rectus femoris, vastus medialis, vastus lateralis, and vastus intermedius—make up the five muscles of the anterior thigh compartment.
- Sartorius
- Origin: Superior iliac anterior (ASIS)
- Insertion: via Pes anserinus, on the medial surface of the proximal tibia
- Femoral nerve innervation (L2-L4)
- Functions of the hip joint include thigh flexion, abduction, and external rotation; those of the knee joint include leg flexion and internal rotation.
Quadriceps femoris
- Rectus femoris
- Origin: Superior margin of acetabulum, Anterior inferior iliac spine
- Insertion: via the patellar ligament, the tibial tuberosity
- Femoral nerve innervation (L2-L4)
- Functions: Knee joint: Leg extension; Hip joint: Thigh flexion
- The vastus medialis
- Origin: Medial supracondylar line of femur; intertrochanteric line; spiral line; and linea aspera.
- Insertion: Medial condyle of femur via patellar ligament to tibial tuberosity
- Innervation: Femoral nerve (L2-L4)
- Function: The leg extension is the knee joint
The biceps femoris, semimembranosus, and semitendinosus muscles are the three posterior compartment muscles, commonly referred to as the hamstring muscles.
- Semimembranosus
- Origin: Ischial tuberosity’s medial impression
- Insertion: Tibial medial condyle
- Innervation: Sciatic nerve’s tibial division (L5-S2)
- Function: Knee joint: Leg flexion, Leg internal rotation, Pelvis stabilization; Hip joint: Thigh extension, Thigh internal rotation
- Semitendinosus
- Origin: Ischial tuberosity’s medial impression
- Insertion: Via the pes anserinus, the proximal end of the tibia is inserted below the medial condyle.
- Innervation: Sciatic nerve’s tibial division (L5-S2)
- Function: Knee joint: Leg flexion, Leg internal rotation, Pelvis stabilization, Thigh extension, Thigh internal rotation
- Biceps femoris:
- Origin: Long head: Ischial tuberosity’s medial impression Short head: Lateral supracondylar line of the femur, Linea Aspera of the femur (lateral lip).
- Insertion: Fibula head
- Innervation: Long head: sciatic nerve’s tibial division (L5-S2) Short head: Sciatic nerve’s common fibular division (L5-S2)
- Functions: of the knee joint are leg flexion and external rotation; hip joint functions are thigh extension and external rotation.
The six muscles that make up the medial compartment of the thigh are the obturator externus, adductor longus, adductor brevis, adductor magnus, and gracilis.
- Pectineus
- Origin: Pectineal line of the pubis, or superior pubic ramus
- Insertion: Femur’s linear aspera and pectineal line
- Femoral nerve innervation (L2, L3)
- Hip joint function: Pelvis stabilization; thigh flexion, adduction, and external/internal rotation
- Magnus adductor
- Origin: Ischiocondylar part: Ischial tuberosity. Adductor portion: Ischial ramus, inferior pubic ramus
- Insertion: Gluteal tuberosity, Linea aspera (medial lip), and medial supracondylar line comprise the adductor part. Ischiocondylar portion: femur’s adductor tubercle
- Innervation: The obturator nerve (L2-L4) innervates the adductor part. Ischiocondylar portion: sciatic nerve’s tibial division (L4).
- Function: Pelvis stabilization; thigh flexion, adduction, external rotation (adductor part), extension, and internal rotation.
- Adductor minimus
- Origin: Public ramus inferior
- Insertion: The femur’s gluteal tuberosity
- Innervetion: Obturator nerve (L2-L4)
- Function: thigh external rotation, thigh adduction
- Adductor longus
- Origin: the pubic body’s anterior surface
- Insertion: The femur’s linea aspera (medial lip)
- Innervation: Obturator nerve (L2-L4)
- Function: external rotation, adduction, and flexion of the thigh; stabilization of the pelvis
- Adductor brevis
- Origin: The inferior ramus of the pubis and the body’s anterior surface
- Insertion: The femur’s linea aspera (medial lip)
- Innervation: Obturator nerve (L2-L4)
- Function: Pelvis stabilization; thigh flexion, adduction, and external rotation
- Gracilis
- Origin: Ischial ramus, inferior ramus of pubis, and body’s anterior surface
- Insertion: Via the pes anserinus, the medial surface of the proximal tibia
- Innervation: Obturator nerve (L2-L3)
- Function: Internal rotation, flexion, adduction, and flexion of the legs
Clinical Anatomy
Here are a few of the most typical hip issues:
Arthritis
Hip tissue deterioration most commonly results from arthritis. The hip is frequently affected by three types of arthritis:
Osteoarthritis
Additionally known as “wear and tear” arthritis. The cartilage that cushions the deteriorating hip bones is harmed by this kind of arthritis. Hip pain and stiffness result from the bones rubbing against one another as a result.
Rheumatoid arthritis
This illness results in inflammation and excessive fluid production in the synovial membrane, the tissue lining the joint. It causes cartilage damage, which results in stiffness and pain.
Traumatic arthritis
often the outcome of a fracture or other trauma.
Bursitis
The joint’s bursa, a sac filled with fluid, becomes inflamed when bursitis occurs. To lessen friction between tissues, the bursa serves as a gliding surface. The hip contains two main bursae.
Both may result in hip joint stiffness and pain:
- Bursa trochanteric
The hip bursa is located on the side of the hip and is isolated from the hip joint by bone and tissue.
- Bursa Iliopsoas
the bursa in the area of the upper buttock.
Avascular necrosis
This disease is characterized by bone loss from insufficient blood flow. Injuries and bone tumors are other possible causes. Hip joint disintegration could result from it.
Hip pointer
a rip or bruise in the muscle attaching to the ilium’s top. Located just below the waist, the ilium defines the crest of the pelvis. Hip pointers can result from falls, blows, or abrupt body twists or turns.
FAQs
What is the other name of the hip bone?
The hip bone, also known as the os coxae, innominate bone, pelvic bone, or coxal bone, is a large, flat bone that is expanded above and below and constricted in the middle.
What bodily part is the hip?
The region on either side of the pelvis is called the hip. There are three parts to the pelvis bone: Ilium. the wide, rounded part of the pelvis.
Where should the hip bone be?
The top of the thighbone, or femur bone, fits into the pelvis at the hip. The longest bone in the body, the femur, runs from the knee to the hip.
Which four types of hips are there?
the final result. Although there are many different forms of pelvis in females, there are four main types: gynecoid, android, anthropoid, and platypelloid.
References
- Ferreira, S. (2023, October 30). Hip bone. Kenhub. https://www.kenhub.com/en/library/anatomy/hip-bone
- Hip bone. (2023, October 15). Wikipedia. https://en.wikipedia.org/wiki/Hip_bone
- Vasković, J. (2023, November 3). Hip and thigh anatomy. Kenhub. https://www.kenhub.com/en/library/anatomy/hip-and-thigh-anatomy
- Hip Problems. (2021, August 8). Johns Hopkins Medicine. https://www.hopkinsmedicine.org/health/conditions-and-diseases/hip-problems