
Femoral Nerve: Anatomy, Course, Pathways, Function
The femoral nerve is one of the major peripheral nerves of the lower limb.
Descriptions:
Nerve roots: L2-L4
Motor functions:
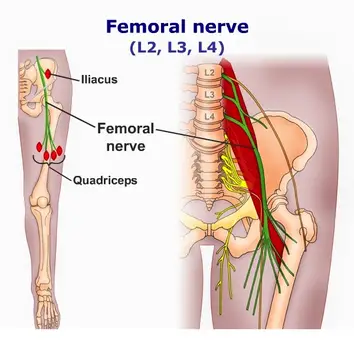
Innervates the anterior thigh muscles that flex the hip joint (pectineus, iliacus, sartorius) and extend the knee (quadriceps femoris: rectus femoris, vastus lateralis, vastus medialis, and vastus intermedius).
Sensory functions:
Supplies cutaneous branches to the anteromedial thigh (anterior cutaneous branches of the femoral nerve) and the medial side of the leg and foot (saphenous nerve).
Anatomy of Femoral nerve:
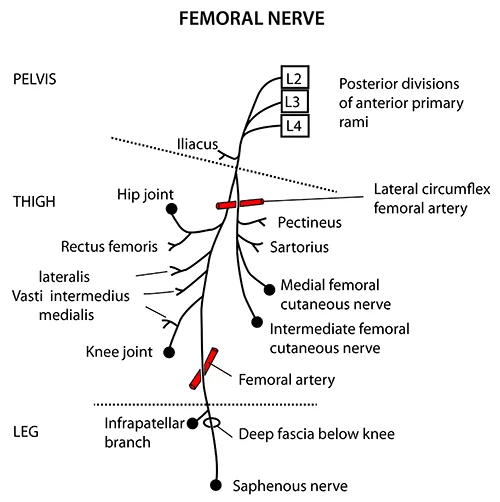
The nerve is the largest branch of the lumbar plexus. It is derived from the anterior rami of nerve roots L2, L3, and L4.
After arising from the lumbar plexus, the nerve travels inferiorly through the psoas major muscle of the posterior abdominal wall. It supplies branches to the iliacus and pectineus muscles prior to entering the thigh.
The nerve then passes underneath the inguinal ligament to enter the femoral triangle. Within this triangle, the nerve is located lateral to the femoral vessels (unlike the nerve, the femoral artery and vein are enclosed within the femoral sheath).
Anterior division:
- Anterior cutaneous branches
- Branch to sartorius
- Branch to pectineus
- Posterior division of the femoral nerve:
- Saphenous nerve
- Branches to quadriceps femoris
- The terminal cutaneous branch of the femoral nerve is the saphenous nerve.
- It travels through the adductor canal (accompanied by the femoral artery and vein) and exits prior to the adductor hiatus.
- The saphenous nerve innervates the medial aspect of the leg and the foot.
Motor Functions:
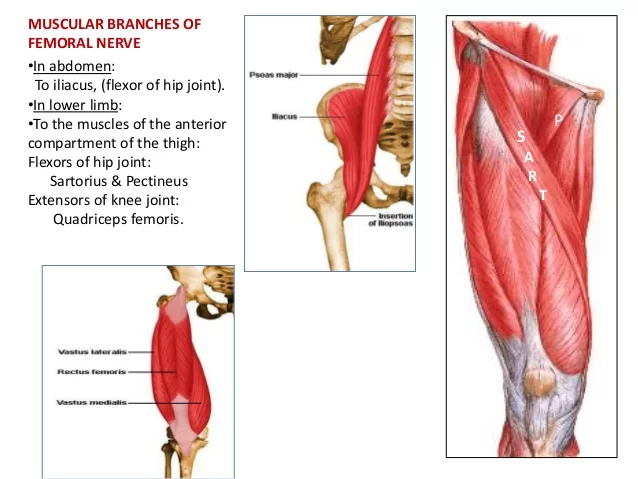
The nerve supplies the muscles of the anterior thigh.
Hip flexors:
- Pectineus – adducts and flexes the thigh, and assists with medial rotation of the thigh.
- Iliacus – acts with psoas major and psoas minor (forming iliopsoas) to flex the thigh at the hip joint and stabilize the hip joint.
- Sartorius – flexes, abducts, and laterally rotates the thigh at the hip joint. Flexes the leg at the knee joint.
Knee extensors:
- Quadriceps femoris (rectus femoris, vastus lateralis, vastus medialis, and vastus intermedius) – extends the leg at the knee joint.
- Rectus femoris also steadies the hip joint and assists iliopsoas in flexing the thigh.
Sensory Functions:
There are two main sensory branches that arise from the femoral nerve:
- Anterior cutaneous branches – derived from the anterior division of the femoral nerve. They supply the skin of the anteromedial thigh.
- Saphenous nerve – a continuation of the posterior division of the femoral nerve. It supplies the skin of the medial leg and foot.
Articular branches:
- The hip joint is supplied by the nerve to the rectus femoris.
- The knee joint is supplied by the nerves to the three vasti.
- The nerve to the vastus medialis contains numerous proprioceptive fibres from the knee joint, accounting for the thickness of the nerve.
- This is in accordance with Hilton’s law: Nerve supply to a muscle that lies across a joint, not only supplies the muscle but also supplies the joint beneath and the skin overlying the muscle.
Vascular branches:
- To the femoral artery and its branches.
Course of Femoral Nerve:
- The nerve is the largest branch of the lumbar plexus. The nerve descends from the lumbar plexus in the abdomen, traveling down through the fibres of the psoas major.
- The nerve exits the psoas major at the lower part of its lateral border, passing behind the iliac fossa to approximately the mid-point of the inguinal ligament.
- It then travels below the inguinal ligament of about 4 cm into the thigh and splits into an anterior and posterior division. The lateral circumflex femoral artery is straddled by both sections.
- The nerve enters the femoral triangle by passing beneath the inguinal ligament, just lateral to the femoral artery. In the thigh, it lies outside the femoral sheath and gives off articular branches to the hip and knee joints.
- The terminal cutaneous branch of the femoral nerve is the saphenous nerve which continues, with the femoral artery and vein, through the adductor canal.
Blood Supply and Lymphatics
Within the femoral triangle, the femoral nerve passes across the femoral artery, vein, and lymphatics. The femoral nerve and its branches receive oxygenated blood flow from the femoral artery and some of its branches to sustain their activity.
Variations
In a case study conducted in Karnataka, India, scientists found that the left femoral nerve of a 65-year-old male cadaver had split in the abdomen as it exited the L2-L4 nerve roots. The femoral nerve was then formed by its rejoining just proximal to the inguinal canal.
Clinical Importance:
- Injury of this nerve is uncommon but may be injured by a stab, gunshot wound, or pelvic fracture.
- The nerve can be damaged during penetrating trauma to the thigh. It can also be damaged during hip operations, particularly the anterior approach (not commonly used) where the nerve can be stretched and damaged. Listed here are the characteristic clinical features:
Motor loss:
- Poor flexion of the hip, because of paralysis of the iliacus and sartorius muscles.
- Inability to extend the knee, because of paralysis of the quadriceps femoris.
Sensory decrease:
- Sensory decline over the anterior and medial aspects of the thigh, as a result of engagement of the intermediate and lateral cutaneous nerves of the thigh.
- Sensory loss on the medial side of the leg and foot up to the ball of the great toe (first metatarsophalangeal joint), because of engagement of the saphenous nerve.
Nerve is responsible for the patellar tendon reflex (tests L3-L4 spinal component)
- Femoral nerve neuropathy occurs when the femoral nerve is compressed as it passes under the inguinal ligament, anterior to the iliopsoas.
- Causes include surgery (hysterectomy, pelvic, hip, femoral artery catheterization, arterial bypass, retroperitoneal tumors, and diabetes mellitus)With the increased use of anticoagulant agents, femoral neuropathy subsequent to spontaneous hemorrhage within the iliopsoas muscle has become a serious and more frequent clinical problem.
- Femoral nerve block (in combination with sciatic nerve block) may be indicated in patients requiring lower limb surgery who cannot tolerate a general anesthetic.
- A femoral nerve block can also be used as peri- and postoperative analgesia for patients with a fractured neck of the femur who cannot tolerate particular analgesics.
Femoral and Saphenous Nerve Blocks
Because femoral nerve blocks do not have the negative effects or addictive qualities of opioids, they are frequently used to treat hip pain in individuals who have had hip fractures. To relieve hip discomfort, the pericapsular nerve group (PENG) inhibits the femoral nerve’s target articular branches.
Radiculopathy
Irritation or inflammation of a nerve root causes radicular pain. Usually, a disc herniation is the cause of this. Pain that travels dermatomal is one of the symptoms. Disc herniations have been linked to both motor and sensory impairments.
Reflexes include an afferent and efferent limb, which are damaged in radicular pain, therefore one might potentially lose their patellar reflex if a disc herniation develops on the L4 spinal nerve root.
Femoral Hernia
Compared to inguinal hernias, femoral hernias are less common, although they are more common in older women. These are femoral canal weakenings that result in the protrusion of abdominal contents. If left untreated, they cause a protrusion in the groin area and can cause strangulation and necrosis of the stomach contents. The femoral vein will be situated lateral to the hernia sac since it is situated in the femoral canal.
Psoas Abscess/Hematoma
Any hematoma or infection might result in a mass effect damage close to the iliacus or psoas muscles. The femoral nerve may be compressed by the expanding abscess or hematoma because of the connection between these muscles and the nerve. This may result in damage to the nerve, which might impact the femoral nerve’s ability to innervate the motor or sensory systems.
Testing the Patellar Tendon Reflex
The quadriceps femoris muscle reflexively contracts when the patellar tendon is tapped with a reflex hammer, which is how the patellar tendon reflex is assessed. The L2-L4 ventral principal rami and the femoral nerve are involved in this response. Tapping the patellar tendon stimulates the muscular spindle fibers of the quadriceps femoris. They are innervated by the femoral nerve, which causes activation of sensory axons with cell bodies located in the dorsal root ganglia from L2-L4. The dorsal roots allow the central processes of the dorsal root ganglion cells to reach the spinal cord, where they subsequently transfer to the ventral horn alpha-motor neurons.
The femoral nerve contains the axons of these neurons, which when stimulated cause the quadriceps femoris muscle to contract. The quadriceps femoris muscle’s tone is preserved via this response. Higher influences can modify the activity of neurons in this circuit.



22 Comments