
Sternocleidomastoid Muscle (SCM Muscle)
Introduction
The sternocleidomastoid muscle is one of the largest and most superficial cervical muscles.
The primary actions of the muscle are rotation of the head to the opposite side and flexion of the neck.
The sternocleidomastoid is innervated by the accessory nerve.
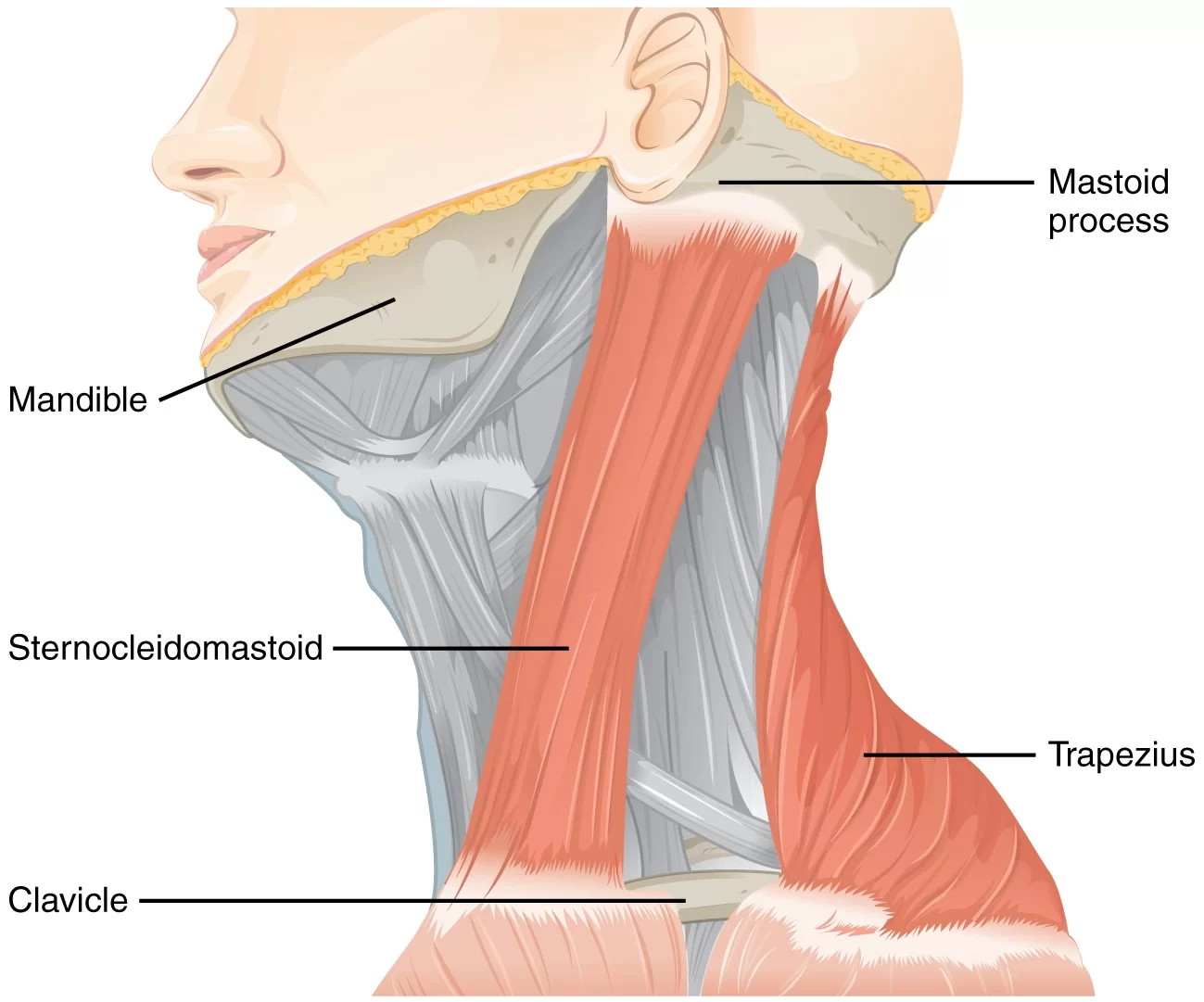
It is given the name sternocleidomastoid because it originates at the manubrium of the sternum (sterno-) and the clavicle (cleido-), and has an insertion at the mastoid process of the temporal bone of the skull.
It is a long, bilateral muscle of the neck, which functions to flex the neck both laterally and anteriorly, as well as rotate the head contralaterally to the side of contraction.
The muscle is closely related to certain neurovascular structures that pass through the neck on their way either to the head or to the periphery of the body.
Anatomy
The sternocleidomastoid muscle (SCM) divides the neck area into an anterior triangle and a posterior triangle.
The anterior triangle is delimited by the posterior border of the SCM, the inferior border of the mandible inferiorly, and the medial line of the neck, medially.
In the anterior triangle, we find the suprahyoid and infrahyoid muscles.
The posterior triangle is delimited by the SCM anteriorly, by the clavicle inferiorly, and by the trapezius muscle posteriorly.
Scalene muscles reside in the posterior triangle. The SCM is a large and easily recognizable and palpable muscle.
SCM can be divided into four portions :
- Sterno-mastoid
- Sterno-occipital
- Cleido-mastoid
- Cleido-occipital
The muscle originates from the upper edge of the sternal manubrium, from the medial quarter of the upper face of the clavicle the two muscle heads merge into a single muscle belly that is directed upwards and laterally.
Insertions arrive at the mastoid process of the temporal bone and at the anterior portion of the superior nuchal line.
SCM has fibers arranged in parallel it is not a pennate muscle.
SCM expresses greater strength and thickness in men than women the sterno-mastoid portion is the muscle area that develops a greater percentage of contractile strength than the other portions.
The cleido-occipital portion is the muscular area where less force develops.
ORIGIN
It arises by two heads:
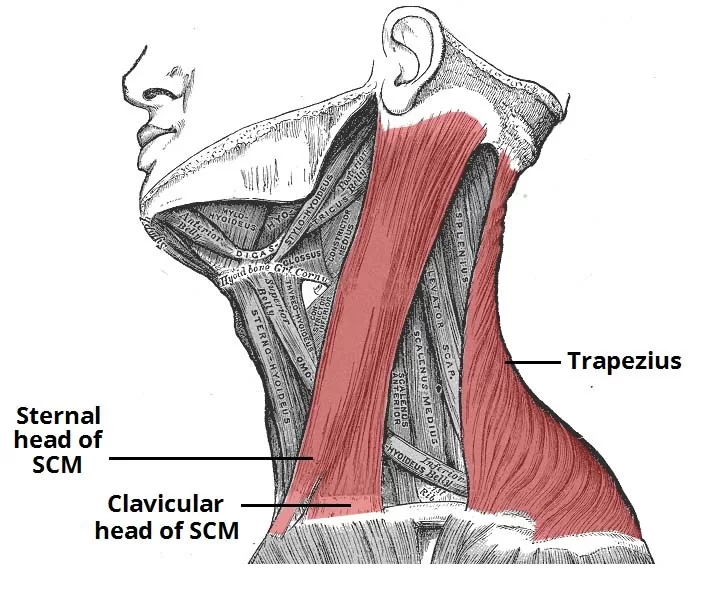
A medial rounded and tendinous sternal head (SH)
A lateral fleshy clavicular head (CH).
- They arise from the anterolateral surface of the manubrium sterni and the medial third of the superior surface of the clavicle, respectively.
- The thickness of the CH is variable.
- The two heads are separated by a triangular surface depression, the lesser supraclavicular fossa.
- As they ascend, the CH spirals behind the SH and blends with its deep surface below the middle of the neck, forming a thick rounded belly.
INSERTION
- Lateral surface of the mastoid process through a strong tendon, and to the lateral half of superior nucheal line through aponeurosis.
STRUCTURE AND FUNCTION
- The unilateral contraction of the sternocleidomastoid muscle (SCM) determines a triple movement, associating the rotation of the head on the side opposite to that of its contraction, the inclination from the side of its contraction, and extension.
- The effects of the simultaneous contraction of the two muscles depend on the state of contraction of the other muscles of the cervical spine :
- If the cervical spine is not fixed, this bilateral contraction determines a hyperlordosis of the cervical spine with an extension of the head and a bending of the cervical spine on the dorsal one.
- If the cervical spine is rigid and rectilinear due to the contraction of the paravertebral muscles, the simultaneous contraction of the SCM determines the flexion of the cervical spine on the dorsal spine and a flexion of the head forward.
- The SCM can also have inspiratory muscle action by taking a fixed point on the temporal bone and then lifting the sternum and the clavicles.
- SCM plays an important role in the posture of the neck and the body.
- It has been shown that a stimulation of the vestibular area electrically activates the
- Sternocleidomastoid with evidence of a close connection between the vestibular area and the motoneurons of the SCM.
- The movement with which the SCM expresses its maximum capacity for speed and force is the lateral inclination.
- Another important function of SCM is to allow a correct function of the temporomandibular joint (TMJ).
- During mastication a trigeminal-cervical reflex stimulates the activity of SCM, there is evidence that SCM intervention is fundamental for optimal TMJ occlusion.
- An occlusal alteration of the mandible causes an alteration of the function of the SCM, with disorders of muscular incoordination (inclinations of the neck).
- The correction of an altered occlusion or the treatment of a tooth has solved, in some cases, the problem of torticollis.
- During mastication on one side, the activity of the SCM is synchronous with the masseter muscle, while with bilateral chewing the SCM anticipates the intervention of the masseter, probably to stabilize the neck.
CLINICAL SIGNIFICANCE
- Examination of the sternocleidomastoid muscle forms part of the examination of the cranial nerves.
- It can be felt on each side of the neck when a person moves their head to the opposite side.
- The triangle formed by the clavicle and the sternal and clavicular heads of the sternocleidomastoid muscle is used as a landmark in identifying the correct location for central venous catheterization.
- Contraction of the muscle gives rise to a condition called torticollis or wry neck, and this can have a number of causes.
- Torticollis gives the appearance of a tilted head on the side involved.
- Treatment involves physiotherapy exercises to stretch the involved muscle and strengthen the muscle on the opposite side of the neck.
- Congenital torticollis can have an unknown cause or result from birth trauma that gives rise to a mass or tumor that can be palpated within the muscle.



14 Comments