Monteggia Fracture
What is a Monteggia Fracture?
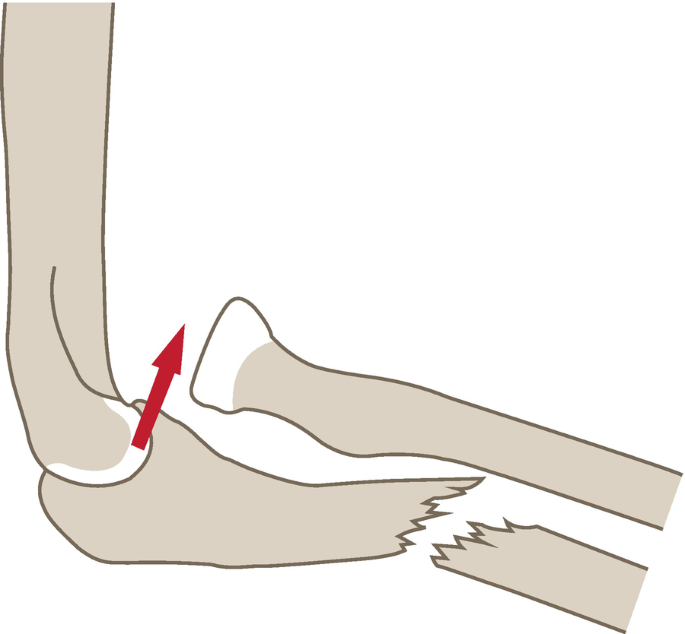
A Monteggia fracture is a severe injury involving a fracture of the proximal third of the ulna, along with a dislocation of the radial head.
Giovanni Battista Monteggia is credited with the term’s origins; he characterized it in 1814. The essential anatomy of the body is the forearm. Significant short- and long-term disability can result from forearm fractures. The development of technology has made it easier to recognize these fractures and has improved the definition, classification, and direction of conservative and surgical management as well as rehabilitation.
Anatomy
The radius and ulna combine to generate two radioulnar joints in the forearm. The radius is located in close proximity to the radial notch of the ulna below and the capitulum of the humerus. The proximal radioulnar joint is the name of this articulation.
The distal radius links medially with the lunate and is articulated at its lateral half with a scaphoid. The ulna is articulated with the trochlea of the humerus proximally, the ulna notch of the radius distally, and the triangular articulate disc of the wrist distally. The distribution of axial load force to the forearm is carried out via the interosseous membrane, which joins the two bones.
Causes of Monteggia Fracture
The most frequent cause of monteggia fractures is a direct blow to the forearm while the elbow is extended and the forearm is hyper pronated. The radio-capitellar joint is disrupted when the proximal quadrate and annular ligaments rupture as a result of the energy from the ulnar fracture traveling along the interosseous membrane.
Together with the bimodal distribution, diaphyseal forearm fractures in young men are typically caused by high-energy trauma, such as falls from a height, sports injuries, and car crashes, whereas fractures in older women are typically caused by low-energy trauma, such as a fall from a ground level.
EPIDEMIOLOGY [incidence]:
- more common in children, with a peak incidence between the ages of 4 and 10;
- uncommon in adults
About 1% to 2% of all forearm fractures are Monteggia fractures. Compared to midshaft forearm fractures, which happen in roughly 1 to 10 out of every 10,000 persons annually, distal forearm fractures occur significantly more frequently.
The post-menopausal phase, osteoporosis, and sports (wrestling and football) are the main risk factors for midshaft forearm fractures. These risk variables are associated with a bimodal occurrence, where the highest prevalence is found in young males (10:10,000) and old females (5:10,000).
Mechanism of injury
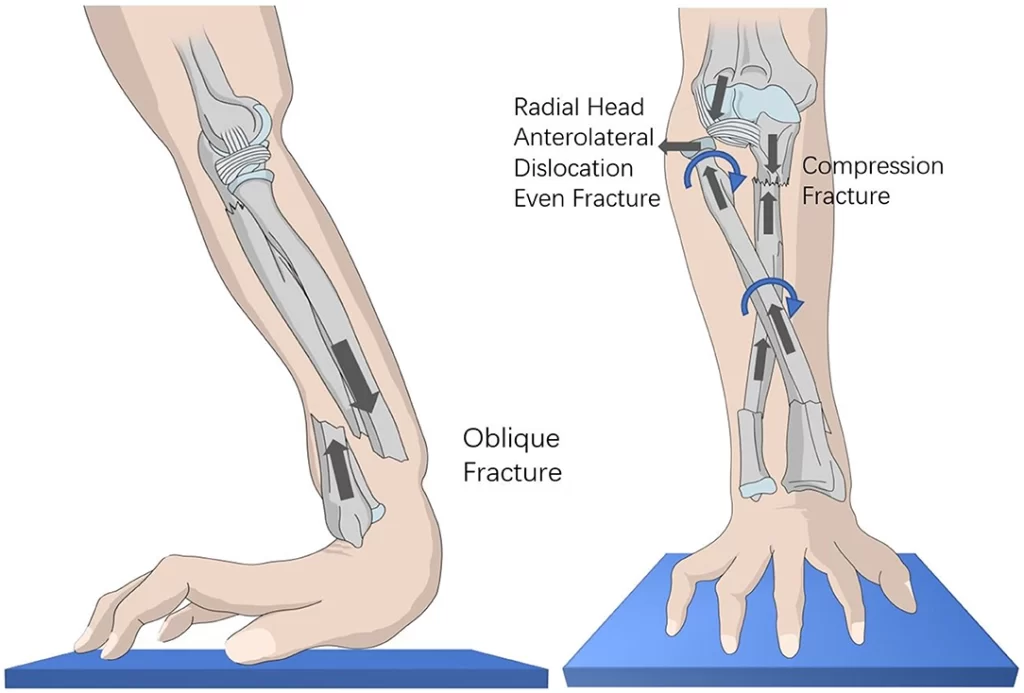
Overextended arms with a hyperpronated forearm are the most common cause of Monteggia fractures. The injury may also arise from a direct impact on the forearm when the forearm is hyperpronated and the elbow is extended.
Some typical causes of this fracture are falls from heights, injuries sustained in contact sports, motorcycle accidents, and osteoporosis.
Mechanisms include are as follows:
- A fall-outstretched hand causes a hyperpronation injury because the forearm is inclined too much. As a result of severe dislocation, the ulna fractures in the proximal third of the shaft. Open soft tissue may or may not occur, depending on the impact and pressures delivered in each direction, pattern, and radial head involvement. The degree of energy absorption also influences these factors.
- A direct impact to the upper forearm’s back would be extremely rare. In this situation, solitary fractures of the ulnar shaft are most frequently observed as a defensive mechanism against blunt trauma (e.g., nightstick injury). A fracture of the ulnar shaft that is isolated like this is not a Monteggia fracture. It is known as a ‘nightstick fracture’.
Pathophysiology
Both the radius and ulna bones make up the osseous forearm. As the humerus rotates during pronation and supination, the proximal radial head articulates with the capitellum (radiocapitellar joint). The radius joins the wrist’s scaphoid and lunate bones distally. At the wrist, the triangular fibrocartilage complex (TFCC) is supplemented by the ulnar head. The coronoid and olecranon are located in close proximity to the ulna.
The interosseous membrane, the annular ligament, and the TFCC are the three ligamentous structures that provide the alignment and stability of the radius and ulna. The radiocapitellar joint receives 60% of the axial load force, the glenohumeral joint receives 40%, and the forearm receives 40% thanks to the interosseous membrane. Forearm stabilization is mostly provided by the radiocapitellar joint, whereas the distal forearm is principally supported by the TFCC.
Classification of Monteggia Fracture
Monteggia’s initial fracture-dislocation was examined by Jose Louis Bado, who further divided it into four categories. This characterizes a group of traumatizing wounds that are similar in that they involve a Monteggia fracture and radial head dislocation in either the anterior or late orientation.
Based on how much the radial head is displaced, there are four types:
Monteggia Fracture in the Bado Classification System is as follows:-
- 1) Extension type (60%): The radial head dislocates anteriorly and the ulna shaft angulates anteriorly. 15% of cases in adults and 70% of cases in children are of the most prevalent type.
- Mechanism of Injury :
- (1) direct hit to the posterior elbow
- (2) hyper-pronated force on an outstretched arm,
- (3) tensed biceps impede forearm extension, inducing dislocation and followed by impact resulting in ulna fracture.
- 2) Flexion type (15%): The radial head dislocates posteriorly and the ulna shaft angulates posteriorly. An axial stress applied with the elbow slightly bent up the forearm is the mechanism of injury. accounting for around 80% of cases, this type is most prevalent in adults. linked to the high incidence of radial head fractures, posterior interosseous nerve damage, and glenohumeral joint instability.
- 3) Lateral type (20%) – dislocation of the radial head to the side and ulna shaft angulation laterally (bent to outside). Greenstick fracture of the ulna is the mechanism of injury caused by a varus force applied to an extended elbow. observed in kids more often.
- 4) Combined type (5%): the radial head is displaced, usually anteriorly, and both the ulna and radial shafts are fractured. Rarest type and poorly understood mechanism.The most primitive kind with an obscure mechanism.
Classification of Type II Monteggia Fracture-Dislocations on Jupiter:
- Type IIA corresponds to the coronoid level;
- Type IIB is the metaphyseal-diaphyseal junction;
- Type IIC is the Distal to coronoid;
- Type IID is a fracture that extends to the distal half of the ulna.
In contrast to fractures of the forearm, these fractures are less prevalent. Ages 4 to 10 are when the incidence peaks.
The most common cause of type I fractures is falling onto an outstretched hand that has the forearm hyperextended or hyperpronated.
History and Physical
Pain at the site of injury is typically reported by patients with diaphyseal forearm fractures. Observing the skin and soft tissue with a keen eye for any obvious bone deformities, muscle contusions, skin lacerations, tendon injury, and neurovascular deficiencies should be the first step in any evaluation. Finding wounds covering fracture sites (open fractures) is crucial because they need to be surgically repaired right away. It is recommended to use a gentle touch to feel for any abnormalities and focused pain.
To find concurrent injuries, a proximal and distal joint examination should be done. Do not poke open wounds. A thorough neurovascular examination is necessary for high mechanism crush injuries, and recurrent serial exams are recommended to check for acute compartment syndrome symptoms.
Ask about weakness, numbness, paresthesias, and discomfort that radiates. Examining the distribution of the radial and median nerves is crucial in recognizing nerve damage, even though it is less prevalent. Ulnar nerve damage is not common.
Examination and Evaluation
Patients typically report pain and swelling at the fracture site when they first arrive. The first step in an examination is a visual assessment of the skin, soft tissue, visible bony deformity, cuts on the skin, contusions in the muscles, and injury to the nervous system. The area surrounding the fracture site may be gently palpated to determine its level of tenderness. It is recommended to use radiographs. The type of fracture can be determined with the use of lateral and anteroposterior images. Additionally to rule out additional fractures and injuries, an x-ray of the wrist and distal radioulnar joint should be obtained.
Radiographs are recommended if a forearm fracture and/or dislocation are suspected. The injury can generally be identified using a lateral and anteroposterior view. A second, oblique view could aid in the injury’s classification. If there is even the slightest possibility that there may be concurrent injuries, further radiographs of the proximal elbow and distal wrist should be taken.
Usually, an initial examination does not reveal the need for advanced imaging. Computed tomography (CT) can be used for pre-operative planning to test for non-union, and magnetic resonance imaging (MRI) can help evaluate for interosseous membrane disruption and TFCC rips.
How do they appear on an x-ray?
It is recommended to order lateral and anteroposterior (AP) x-rays of the forearm, which should encompass the elbow and wrist. To evaluate the radio-capitellar joint, a real AP and lateral view of the elbow is also required, not only a forearm view.
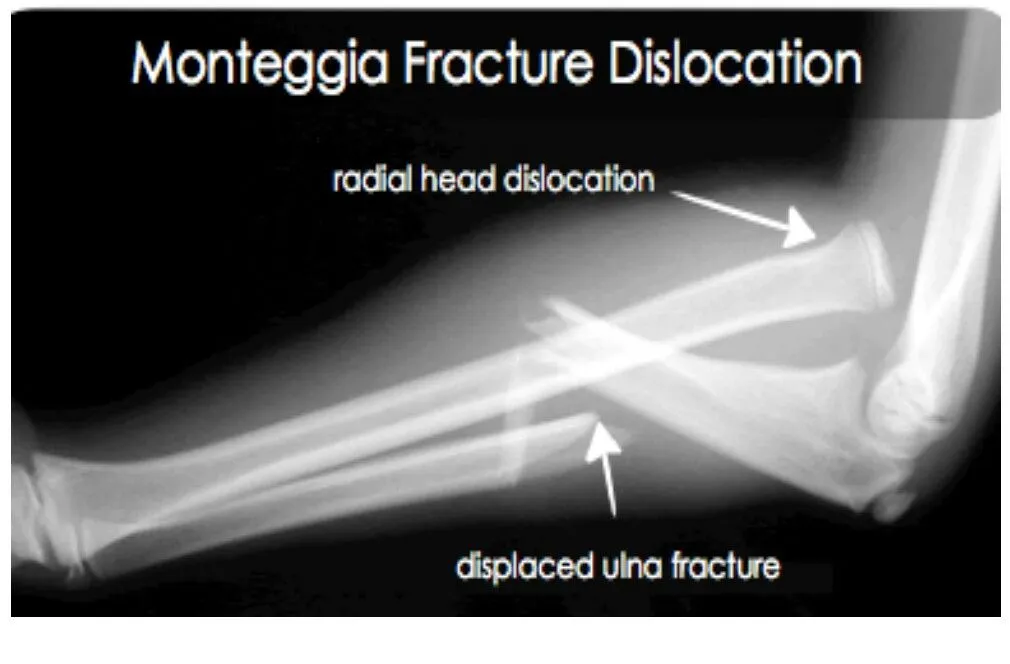
On an x-ray, Monteggia fracture dislocations are readily overlooked.
Always keep an eye out for a radial head dislocation if there is an ulna fracture. It is critical to obtain elbow and forearm X-rays in order to diagnose this ailment.
TIP: In order to rule out joint dislocation, a line drawn along the radius shaft should, in both AP and lateral X-ray images, point to the radio-capitellar line, which indicates the center of the capitellum.
It’s also important to evaluate the ulna’s posterior margin. It needs to be straight rather than curved. It denotes plastic deformation damage if it is not straight.
Prognosis
Complication risks dramatically rise if a diagnosis is postponed for longer than two to three weeks. Early treatment often yields positive outcomes in youngsters, usually returning them to normal or almost normal. Delays in diagnosis increase the need for reconstructive surgery, increase the likelihood of complications, and lower the quality of the outcome. When it comes to adults, Less time is spent healing, and the outcomes are typically less favorable.
The following are possible side effects of ORIF surgery for Monteggia fractures: non-union, malunion, muscle damage, arthritis, tendonitis, infection, stiffness and loss of range of motion, compartment syndrome, audible popping or snapping, deformity, and persistent pain related to surgical hardware like pins, screws, and plates. Since this kind of fracture is nearly always extremely difficult and calls for an experienced orthopedic surgeon—typically a specialist experienced with this kind of injury—multiple procedures may be necessary to fix it.
Complications
- The most often damaged nerves are the posterior interosseous nerve and the radial nerve in particular. Aulna A retrospective analysis of 112 patients revealed that non-union and malunion may happen with both conservative and surgical therapy through postoperative complications, however, this is uncommon.
- Nerve damage
- The majority of consequences result from failing to diagnose or postponing treatment of a Monteggia fracture.
- A more difficult and invasive surgical approach may be necessary for untreated or misdiagnosed radial head dislocations that go untreated for two to three weeks. This approach carries a higher risk of complications, such as recurrent radial head dislocations, persistent subluxations, and loss of normal elbow range of motion and function. Other issues include myositis ossificans, osteoarthritis, compartment syndrome, elbow stiffness, and wound infection.
The most common side effect is a delayed diagnosis. After a delayed diagnosis, care is far more complicated, and results are far less fulfilling. This explains why lawsuits are frequent.
Treatment of Monteggia Fracture
Every Monteggia fracture is a moment to it’s unstable and requires medical attention. If there is vascular compromise or open fractures, immediate orthopedic consultation is necessary. In the event of neurologic impairments without vascular compromise, immediate orthopedic consultation is an alias.
The first steps in treating a suspected fracture are elevation, immobilization, ice, and rest. The majority of the time, closed reduction wants to exist. It is impossible to reduce the annular ligament if it is set inside the joint. When someone finds out with a Monteggia fracture, they need to put in a sugar-tong splint and refer to an orthopedist right away.
Pediatrics
Overall, children typically fare better than adults. Some of the factors a moment possibly responsible for this include the general solidity of Monteggia fractures in children, the remodeling ability of small angle deformities, and a quicker healing time. The features of the ulna fracture dictate the course of treatment. If the ulna has experienced either an incomplete fracture (greenstick) or plastic deformation (bending or bowing without fracture), non-operative therapy is effective in this population.
For six weeks, the elbow is fully supinating and flexes at about 110 degrees while wearing a splint to treat this fracture. A closed reduction is necessary. Operative care is necessary for complete ulnar fractures. It is telling to use elastic intramedullary titanium nail fixation to stabilize short, oblique fractures. By ORIF, fractures of the ulna that are comminute or long oblique are repaired with plates and screws.
Adults
- Most adult Monteggia fractures require careful attention during operations. Despite closed reduction procedures, adults are more susceptible to persistent angulation and shortening. An ORIF is the most popular type of surgical repair. Six cortical screws are usually necessary to position one compression plate, and they secure it both proximally and distally.
- The realignment of the ulna fracture frequently results in an easy reduction of the radial head dislocation. Following surgery, the affected extremity is placed in a long-arm splint with elbow flexion at approximately 100 degrees and complete supination for Bado types 1, 3, and 4 fractures. Elbows with Bado type 2 fractures need to get a splint at 70 degrees.
- Like other fractures, the extent of recovery is contingent upon a number of factors, such as the degree of damage sustained, the anticipated use of the affected extremity, and the healing capacity of the patient. Typically, two weeks following surgical fixing is when rehabilitation starts.
- Regaining a complete range of motion and fine motor abilities in the absence of discomfort is the aim of rehabilitation. The extent of the damage and the patient’s anticipated usage of their upper extremities will determine when they can resume their full range of activities.
- Rehabilitation times may need to be extended for athletes and manual laborers. In individuals with low physical demands, a typical return to full activity can happen in eight to twelve weeks. Rehab may be necessary for up to 12 to 16 weeks for patients with high-demand activities, such as manual laborers and athletes.
- Less than 10% of patients require the removal of surgical hardware, which is typically left in place permanently. There is always an urgent need for reduction. Under a general anesthetic, this is typically performed in a theater.
- Medical care for Monteggia fractures must be provided right away. To rule out any neurological deficiency and for the purpose of diagnosis and treatment, an orthopedic consultation is necessary. The RICE protocol—rest, icing, immobilization, and elevation—is a part of early care.
- Depending on how severe and extensive the fracture is, a closed reduction can usually help to cure it. Open reduction and internal fixation with screws and plates are necessary surgical interventions for open fractures, comminuted fractures, and long oblique fractures.
- A single compression plate is typically positioned using six cortical screws that are fastened both proximally and distally. Closed reduction is performed for incomplete fractures with stable length and green stick ulna fractures, and an intramedullary pin fixation is an option for transverse and short oblique fractures. It is possible to reduce the radial head dislocation after the ulna fracture is completely rectified.
- The recovery depends on a number of variables. The period of rehabilitation varies depending on the type of fracture, the degree of the injury, the treatment plan, and the health of the individual. The healing process for a fracture can often take up to six weeks, and rehabilitation starts immediately following the cast’s removal.
Physiotherapy Treatment
- In conservative care, the two to three weeks following surgery are dedicated to rehabilitation, which begins right away when the cast is discarded. Getting back to one’s full range of motion and fine motor skills pain-free is the aim of rehabilitation. Returning to activity is contingent upon the severity of the injury and its contributing factors. Prolonged rehabilitation may be necessary for athletes and manual laborers.
- In patients with low physical demands, a full return to activity can happen in eight to twelve weeks. Individuals with physically demanding jobs, such as manual laborers and athletes, may need more time to get back to their original field.
- After an extended period of immobilization, the joint is more likely to become stiff. Therefore, it’s time to start exercising. The purpose of the exercise is to increase the joint’s range of motion and strengthen the forearm and elbow muscles.
- After six weeks of surgery, the actual exercises and physiotherapy regimens are required to take effect. The goal of the exercises is to regain the strength of muscle and elbow joint motion. The elbow joint stiffness is the most frequent complication after the period of immobilization.
- Swelling of hands and fingers is a common complaint for which you can follow a few practical home remedies for hand swelling. Swelling in the hand or hand edema if stays for prolonged impacts the joint range of motion, soft tissue mobility, quality of scar tissue formation, function, strength, and appearance of the hand. A contrast bath is the term for this method.
- The most popular methods for treating this kind of swelling are compression, elevation, and massage. Compression is reaching success via wearing a compression glove, which keeps the hand compressed and stops the fluid from staying around. While all of these methods are significant, the advice I’m going to provide you with now is just as helpful and has long-term consequences.
- But in my clinical experience, I’ve discovered that the majority of them experience problems with frozen shoulders in the affected upper limb. Additionally, they experience stiffness in the small finger joints and wrist. Therefore, to address all of these issues when planning exercises, a holistic approach is necessary.
So let us start with the exercises right away.
1) Flexion and extension of the elbow
Simply said, elbow flexion-extension refers to bending and straightening the elbow joint. Exercise concentration is crucial for treating elbow stiffness. This exercise has to be performed right away after the slab is removed.
Initially, you should stabilize your arm during elbow flexion-extension exercises to be a little cautious because of the pain. To do this, take a seat with a table in front of you, and stabilize it by placing your injured arm flat on the surface. To allow for enough elbow movement, the elbow should ideally be at the table’s edge.
Starting from this posture, gradually move your forearm to bring your elbow into a bent or straightened position. For added stability, you could hold the arm with a different hand. Starting out with a pain-free range of motion, you should gradually increase the movement’s intensity if you progress. In due course, you will be able to perform this exercise freely without the assistance of a table.
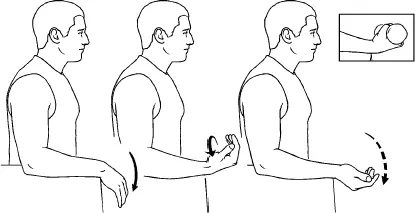
2) With the help of a wand, supine the forearm.

People ignore forearm pronation supination motion so frequently. This exercise begins with the person sitting next to a table with their forearms flat on the surface. To provide enough space for a stick to move, place the wrist at the edge of the table.
Now, rotate the stick in a range of motion that causes no pain in both clockwise and counterclockwise directions. With time, advance to a more forceful pronation-supination motion of the forearm.
3) Pendulum exercise
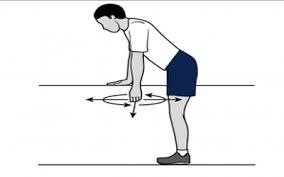
Dumbbells, weighing 1.5 to 2 kg for adults and 1 kg for children, are necessary for this exercise. With the afflicted hand, firmly stand and hold the dumbbell.
To allow the dumbbell’s weight to exert a pulling force on the elbow, loosen the muscles surrounding the elbow and arm. You have the option of swinging it back and forth like a pendulum or holding it in place for thirty seconds.
This is a very good exercise for completely extending the elbow joint.
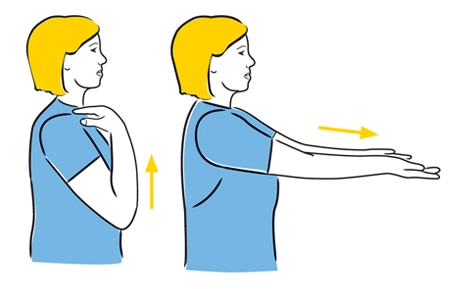
4) Elevating the shoulders
Following immobilization, Monteggia fracture patients frequently experience stiffness and shoulder pain. I would suggest starting with the shoulder elevation exercise out of all the exercises for the shoulders.
It’s very simple to do; just hold both hands together and keep your elbows straight. Now raise your shoulder as high as pain permits. Try to extend the range of elevation with each exercise repetition.
5) Flexion-extension of the wrist
Under such circumstances, wrist stiffness is also observed. Maintain a flat arm position with your forearm 90 degrees off the table while you sit with a table in front of you. To stabilize your wrist joint, place your other hand directly below the wrist joint and hold your forearm there.
Now, in a single session, bend the wrist forward and backward at least 20 to 30 times
6) Circumduction of the wrist
The beginning posture for this exercise is the same as it was for the last one; simply rotate your wrist for two to three minutes in both clockwise and counterclockwise directions.
7) Practice strengthen your grip

Numerous patients with this condition also exhibit weak grip strength and tight finger joints, choosing to ignore their affected hand during the period of immobility.
You will thus need a gel exercise ball for this activity. Grab it and squeeze it as hard as you can for as long as you can. An easy-to-do but incredibly powerful exercise.
Differential Diagnosis
- Elbow dislocation
- Elbow fracture
- Emergent management of hand dislocation
- Hand fracture management
- Wrist dislocation
- Wrist fracture
Outcome Measures
- Shoulder and Hand Questionnaire (DASH)
- Visual analog scale to assess pain
- A dynamo meter is helpful in measuring grip strength, which is created for use as an outcome measure to evaluate daily functional tasks.
- Six scales make up the Michigan Hand Outcomes Questionnaire (MHQ) is a hand-specific outcome measure:
- 1. General role of the hands
- 2. Daily living activities
- 3. Hurt
- 4. Productivity at work
- 5. Visual appeal
- 6. Contentment of the patient with hand function
FAQs
How does the Monteggia fracture differ from the Galeazzi fracture?
Monteggia fractures and their variations are set forth, similar to fractures of the proximal 1/3 of the ulna that accompanies proximal radioulnar joint (PRUJ) disruption, which presents as radio-capitellar subluxation or dislocation. Galeazzi fractures are radial shaft fractures that are accompanied by a dislocation of the distal radioulnar joint (DRUJ).
How come Monteggia fractures happen?
Falling on an outstretched hand with forceful pronation is the main cause of Monteggia fractures. The chance of an elbow flexion injury, either type II or type III, increases. Similar injuries can occasionally result from a direct hit to the forearm.
Which nerve is in danger in a fractured Monteggia?
The most frequent nerve injury linked to Monteggia fractures is posterior interosseous nerve palsy. Anatomical reduction of the radial head dislocation and ulnar fracture is necessary to achieve.
References
- Monteggia fracture. (2020, October 21). Wikipedia. https://en.wikipedia.org/wiki/Monteggia_fracture#Causes
- Monteggia Fracture. (n.d.). Physiopedia. https://www.physio-pedia.com/Monteggia_Fracture
- Clinical Practice Guidelines : Monteggia fracture-dislocations – Emergency Department. (n.d.). https://www.rch.org.au/clinicalguide/guideline_index/fractures/monteggia_fracturedislocations_emergency_department_setting/
- Jones, T. (n.d.). Monteggia Fractures – Trauma – Orthobullets. https://www.orthobullets.com/trauma/1024/monteggia-fractures
- Johnson, N. P. (2023, July 31). Monteggia Fractures. StatPearls – NCBI Bookshelf. https://www.ncbi.nlm.nih.gov/books/NBK470575/#:~:text=The%20Monteggia%20fracture%20is%20a,proper%20management%20is%20not%20instituted
- Ekka, S. S. (2022, August 29). Monteggia fracture PT management – Physiosunit. Physiosunit. https://physiosunit.com/monteggia-fracture-its-treatment/