Oblique Vein of the Left Atrium
Introduction
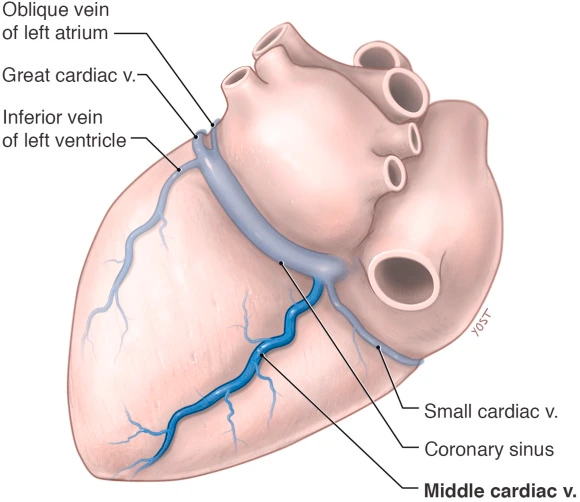
The human heart’s oblique vein of Marshall (OVM), on the odd occasion referred to as the left atrium’s oblique vein, is fascinating despite having very little internal structure. This vein, which is located in the left atrium’s posterior aspect, is valuable for both clinical cardiology and embryological development.
The correspondingly small “oblique vein of Marshall,” which usually terminates close to the left atrial tip, extends diagonally across the chamber’s rear. When it meets the left vena cava ligament, it becomes the remains of the left Cuvierian duct; because it is continuous above, it frequently goes by the other name in the structure of human beings. The oscillations in the myocardial perfusion in this unknown region near the SA node, both in systole and/or diastole, may also have an influence on cardiac autonomic innervation. Many observers feel that this channel ought to be closed.
Anatomy of oblique vein of Marshall
- Location: On and indeed the posterior border of the left atrium, the Marshall oblique vein is established near beyond the left pulmonary veins left atrial appendage. Also known as the oblique sinus of the pericardium, it passes through the region of the human heart’s left side between the posterior aspect of the heart and the pulmonary veins.
- Origin: The left side of the superior vena cava (SVC) remnant gives rise to the oblique vein of Marshall during fetal development in the structure of the human body. In most cases, the left superior vena cava recedes and/or forms the ligament of the Marshall, leaving the Marshall oblique vein smaller in the human anatomy structure.
- Course: The vein typically courses in a curving manner along the posterior left atrium. It may vary in size and can sometimes be found as multiple small veins or channels rather than a single distinct vessel.
Structure oblique vein of Marshall
- Dimensions and Characteristics: The oblique vein of Marshall is generally small in diameter, ranging from a few millimeters to around a centimeter in some cases. Its size can vary between individuals, and its structure can sometimes be complex, with multiple branches or tributaries.
- Connections:
- Coronary Sinus: In the atrioventricular groove, which is set apart of the left ventricle from the left atrium, and also the Marshall oblique vein which chooses to unite with the coronary sinus, a larger vein of the human body. This connection serves as a pathway through which blood from the left atrium can drain into the systemic circulation.
- Left Atrial Appendage: It also has connections to the left atrial appendage, contributing to the venous drainage of this region of the heart.
- Clinical Significance:
- Arrhythmias: Atrial fibrillation and other arrhythmias are believed to be linked to the pathophysiology of the Marshall oblique vein. It can harbor arrhythmogenic foci and may serve as a conduit for abnormal electrical impulses, contributing to the initiation and maintenance of irregular heart rhythms.
- Interventional Procedures: In clinical practice, the oblique vein of Marshall can be targeted during procedures such as catheter ablation for atrial fibrillation. Disrupting its role in arrhythmia propagation can be part of therapeutic strategies to restore normal heart rhythm.
Research and Future Directions: Ongoing research continues to elucidate the precise anatomical variations and functional implications of the oblique vein of Marshall. Insights gained from these studies may inform novel therapeutic strategies and improve outcomes for patients with cardiac arrhythmias.
In a nutshell, the Marshall oblique vein, which is sometimes obscured by more substantial cardiac structures is an essential conduit connecting embryology, anatomy, and clinical cardiology. It presents opportunities as well as obstacles for future research in the field of cardiovascular medicine.
What Specific Function Does the Left Atrial Oblique Vein Serve?
A vast array of functions, including both potential adult physiological roles and vestiges of embryology, are associated with the oblique vein of Marshall and/or the oblique vein of the left atrium (OVM).
- Embryological Remnant: During fetal development, the oblique vein of the left atrium represents a remnant of the left superior vena cava (SVC), which normally regresses as the heart matures. The persistence of the oblique vein of the left atrium highlights its embryological origins and its role as a vestigial structure in the adult heart.
- Venous Drainage: The posterior left atrial venous drainage gets involved in the left atrial oblique vein. Expected to give that the human coronary sinus is a larger vein that transports the blood from the heart’s muscle to the right atrium of the heart, it might also be a viable avenue for fusion in the human body. This drainage pathway helps maintain proper circulation within the heart of the human being.
- Arrhythmogenic Potential: Despite its primarily venous drainage function, the oblique vein of the left atrium has gained attention for its potential involvement in cardiac arrhythmias, particularly atrial fibrillation. It has been proposed that the oblique vein of marshall may harbor arrhythmogenic foci or abnormal electrical connections that contribute to the initiation or perpetuation of irregular heart rhythms. In some cases, interventions such as catheter ablation may target the oblique vein of the left atrium to disrupt these pathways and restore normal heart rhythm.
Ongoing research continues to explore the functional significance of the oblique vein of marshall in both normal cardiac physiology and pathological conditions. Advances in imaging and electrophysiological mapping techniques are enhancing our understanding of its role in arrhythmogenesis and guiding therapeutic strategies for managing cardiac arrhythmias.
In summary, while traditionally viewed as a remnant of fetal circulation, the oblique vein of the left atrium plays a crucial role in venous drainage within the heart and has implications for cardiac electrophysiology, particularly in the context of arrhythmias. Its complex anatomy and potential pathological involvement underscore its significance in clinical cardiology and ongoing research endeavors.
What diagnostic techniques are applied to evaluate Marshall’s oblique vein?
The oblique vein of Marshall (OVM) can be assessed using various diagnostic methods to evaluate its anatomy, function, and potential involvement in cardiac conditions. The main techniques which are used for diagnosis are as follows:
- Echocardiography:
- Transesophageal Echocardiography (TEE): Using only a specialized probe inserted into the esophagus, this imaging technique produces precise views of the heart and its structures, including the posterior left atrium, which contains the left atrium’s Oblique vein. Transesophageal echocardiography can also be used to evaluate blood flow patterns and/or find any anomalies in the Marshall Oblique vein by providing real-time images and Doppler flow data.
- Computed Tomography (CT):
- Cardiac CT Angiography: Computed Tomography Scan imaging can be used to visualize the anatomy of the heart and its surrounding structures in great detail. Cardiac CT angiography is particularly useful for assessing the spatial relationships of the oblique vein of the left atrium with other cardiac structures, identifying variations in its size or course, and evaluating for any structural abnormalities.
- Magnetic Resonance Imaging (MRI):
- Cardiac Magnetic Resonance Imaging: Utilizing radio waves and also strong magnets, magnetic resonance imaging (MRI) creates high-definition, radiation-free images of the heart and/or blood vessels. Cardiac MRI can also provide high-resolution images of the Oblique vein of a marshall, allowing for assessment of its anatomy, venous connections, and functional aspects such as blood flow dynamics.
- Electrophysiological Mapping:
- Electrophysiological Studies (EPS): In cases where the oblique vein of marshall is suspected to play a role in cardiac arrhythmias, such as atrial fibrillation, electrophysiological mapping may be performed. This involves inserting catheters into the heart to map electrical activity and identify potential arrhythmogenic foci within or near the oblique vein of the left atrium. Electrophysiological mapping helps guide therapeutic procedures like catheter ablation aimed at disrupting these abnormal pathways.
- Intracardiac Echocardiography (ICE):
- Intracardiac Echo: During catheterization procedures, intracardiac echocardiography may be used to obtain detailed images of the heart structures, including the oblique vein of the left atrium, from within the heart chambers. For interventions aimed at the oblique vein of Marshall, it offers real-time visualization and guidance.
- Angiography:
- Cardiac Catheterization and Angiography: This invasive procedure involves inserting a catheter into the heart chambers to inject contrast dye and visualize blood flow through the coronary arteries and cardiac veins. Angiography can also help assess the venous drainage patterns involving the Oblique vein of the marshall and identify any abnormalities or variations.
Clinical Correlation and Integration: Diagnostic assessment of the oblique vein of marshall often involves integrating findings from multiple imaging modalities and functional studies. This comprehensive approach helps cardiologists and cardiac imaging specialists to accurately evaluate the OVM’s role in cardiac physiology and pathology, guiding appropriate management strategies for patients with related cardiovascular conditions.
In summary, the diagnostic methods used to assess the oblique vein of Marshall (OVM) range from non-invasive imaging techniques such as echocardiography, CT, and MRI to invasive procedures like electrophysiological mapping and cardiac catheterization. The choice of diagnostic approach depends on the clinical indication, patient characteristics, and the specific information needed for the effective management of cardiac conditions involving the oblique vein of the left atrium.
What are Marshall’s oblique vein’s branches and tributaries?
The oblique vein of Marshall (OVM), though a small structure, can exhibit variations in its tributaries and branches among individuals. An outline of the common connections and variations is provided below:
- Coronary Sinus Connection: The predominant tributary of the oblique vein of the left atrium is the coronary sinus. The oblique vein of marshall typically drains into the coronary sinus, which itself collects venous blood from various cardiac structures, including the left atrium and ventricle.
- Connections to Other Veins: The OVM may have additional connections or branches that can vary:
- Left Superior Vena Cava (SVC): In some individuals, remnants of the left Superior vena cava may persist and contribute to venous drainage into the OVM. This connection is more common in individuals where the left superior vena cava does not completely regress during fetal development.
- Left Atrial Appendage: The OVM can also have connections or branches that extend towards the left atrial appendage, contributing to the overall venous drainage in this region.
- Variations: The anatomy of the OVM can vary significantly among individuals. It may present as a single vessel or consist of multiple small branches or channels that collectively contribute to its function as a venous conduit.
- Clinical Significance: Understanding the anatomical variations and connections of the OVM is important in clinical settings, especially during procedures such as catheter ablation for atrial fibrillation. Mapping the oblique vein of the left atrium and its tributaries helps in identifying potential arrhythmogenic foci and planning effective therapeutic interventions.
Simply put, the main branch that feeds into the oblique vein of Marshall is the coronary sinus, but there could be different connections and branches that may affect its function in heart physiology or its potential contribution to conditions like cardiac arrhythmias.
What occurs if the patient has a compromise in the left atrium’s oblique vein?
Compromise or pathology involving the oblique vein of Marshall (OVM) can potentially impact cardiovascular function and lead to various clinical consequences. Here are some potential scenarios and implications if the OVM is compromised:
- Impaired Venous Drainage: An opening for venous drainage from the rear of the left atrium is provided by the Marshall Oblique Vein. If compromised, such as by stenosis (narrowing), thrombosis (clot formation), or compression, it may impede proper venous return from this region of the heart.
- Arrhythmias: The Oblique vein of the left atrium has been implicated in the pathogenesis of cardiac arrhythmias, particularly atrial fibrillation. Compromise of the Oblique vein of the left atrium, either through structural abnormalities and/or dysfunction, might also contribute to the initiation or perpetuation of irregular heart rhythms in the body. This can occur due to altered electrical conduction pathways or as a result of hemodynamic changes affecting atrial function.
- Thromboembolic Events: In cases where the OVM forms aneurysms or abnormal connections (fistulas), there may be an increased risk of thrombus (blood clot) formation within the vein. These clots can potentially embolize (travel) to other parts of the circulatory system, causing thromboembolic events such as stroke or pulmonary embolism.
- Hemodynamic Compromise: The OVM’s role in venous drainage contributes to maintaining optimal hemodynamics within the heart. Compromise of its function or structure may lead to hemodynamic instability, potentially manifesting as symptoms of heart failure or exacerbation of underlying cardiovascular conditions.
- Clinical Management: Diagnosis of compromised OVM typically involves imaging studies such as echocardiography, CT angiography, or MRI to assess its anatomy and function. Management strategies depend on the specific pathology identified and may include medical therapy to manage arrhythmias or anticoagulation to prevent thromboembolic events. In some cases, interventional procedures or surgical correction may be necessary to address structural abnormalities affecting the OVM.
In summary, the compromise of the oblique vein of Marshall can have significant implications for cardiovascular health, ranging from arrhythmias to thromboembolic complications. Timely diagnosis and appropriate management are crucial in optimizing outcomes and preventing potential complications associated with OVM pathology.
Disclaimer for an oblique vein of the left atrium: A disclaimer regarding the oblique vein of the left atrium (OVM) would typically emphasize several points to ensure clarity and context in discussing this anatomical structure:
- Medical Advice: Information provided about the OVM, including its anatomy, function, and clinical implications, should not be interpreted as medical advice. It is essential to consult qualified healthcare professionals for personalized medical guidance and treatment.
- Complexity and Variability: The anatomy and/or function of the Oblique vein of the left atrium might also vary among individuals. Descriptions provided are based on general anatomical knowledge and may not apply universally to all cases.
- Clinical Relevance: Discussions about the OVM concerning cardiac conditions, such as arrhythmias, are based on scientific research and clinical observations. However, individual patient scenarios can differ, and specific medical decisions should be based on comprehensive evaluation by healthcare providers.
- Research and Updates: Medical knowledge, including understanding of the OVM, continues to evolve through ongoing research and advancements in medical science. Information provided may be subject to updates or revisions based on new findings.
- Limitations of Information: Information about the OVM presented in educational or general contexts may not encompass all potential aspects or nuances related to this anatomical structure. Specific medical inquiries should be addressed through appropriate medical channels.
- Legal Considerations: Use of information regarding the OVM for diagnostic, treatment, or procedural purposes should adhere to applicable legal and regulatory standards, including those specific to medical practice and healthcare delivery.
- Sources and References: Acknowledgement of sources and references used in discussing the OVM helps maintain transparency and credibility.
This disclaimer aims to provide a balanced perspective on discussing the OVM, ensuring responsible dissemination of information while emphasizing the importance of professional medical consultation for individual healthcare needs.
FAQs
What effects does Marshall’s oblique vein have on clinical practice?
The oblique vein of Marshall has been incriminating in cardiac arrhythmias and/or particularly atrial fibrillation. It may harbor arrhythmogenic foci or abnormal electrical pathways that contribute to irregular heart rhythms. Catheter ablation procedures may target the OVM to disrupt these pathways.
What interdependence do other cardiac compositions have with the Marshall oblique vein?
The left atrial oblique vein is located anatomically between the left pulmonary veins and the left atrial appendage within the human body structure. It connects with the coronary sinus and may have variations in its connections, including remnants of the left SVC.
Is the Marshall oblique vein anatomically different from other veins?
Yes, different people will have different OVM anatomical features. It may present as a single vessel or consist of multiple small branches or channels. Variations can impact its clinical relevance and management in cardiac procedures.
Is the oblique vein of Marshall always present in every discrete?
The OVM is typically present as a remnant of fetal development, but its size and prominence can vary. In some cases, it may not be identifiable or may have minimal clinical significance.
Do irregularities in the Marshall oblique vein negatively impact health?
Rarely, abnormalities such as dilations, fistulas, or other structural defects in the OVM can occur. These may impact venous drainage or contribute to pathological conditions, requiring specific medical evaluation and management.
How does research continue to advance understanding of the oblique vein of Marshall?
Ongoing research focuses on elucidating the precise role of the OVM in cardiac physiology and pathology, including its involvement in arrhythmias and potential therapeutic interventions. Advances in technology and/or medical imaging contribute to magnifying understanding and/or treatment proposed action.
Reference
The human heart’s oblique vein of Marshall (OVM), on the odd occasion referred to as the left atrium’s oblique vein, is very fascinating despite having very little internal structure. The left atrium’s posterior aspect holds a significant vein that is important for clinical cardiology and embryological development. If you want to explore further details about it, you can refer to the following sources:
- Gray’s Anatomy: The classic anatomy textbook provides detailed descriptions of anatomical structures, including the oblique vein of Marshall.
- Clinical Anatomy by Regions by Richard S. Snell: This textbook typically covers anatomical details comprehensively, including the veins of the heart.
- Medical Journals: Articles in journals such as the Journal of Cardiovascular Electrophysiology or the Journal of Anatomy often include discussions or studies involving the oblique vein of Marshall.
- Textbooks on cardiology, such as “Braunwald’s Heart Disease: A Textbook of Cardiovascular Medicine” book by Douglas L. Mann and other authors, and “Hurst’s The Heart” by Robert O., are highly recommended. Bonow and others, are likely to have sections discussing the anatomical and clinical relevance of the oblique vein of Marshall.
- Online Medical Databases: Websites like PubMed or Google Scholar can be searched using keywords such as “oblique vein of Marshall anatomy” or “oblique vein of left atrium” to find recent research articles and reviews.
These resources should provide a comprehensive understanding of the anatomy, clinical significance, and current research related to the oblique vein of Marshall.