Semitendinosus Muscle

Semitendinosus muscle is one of four posterior thigh muscles that are responsible for extending the hip and one of three muscles that are part of the Hamstring group.
The other three muscles that belong to the hip extensor group are the semitendinosus, biceps femoris, and gluteus maximus, while semimembranosus, semitendinosus, and biceps femoris are referred to as the hamstring muscles.
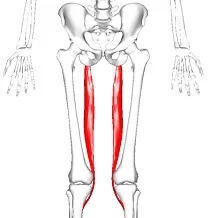
The Semitendinosus muscle (along with the Semimembranosus) occupies the medial aspect of the posterior thigh. It is a relatively long muscle that spans the full length of the thigh – from the hip to the knee.
Origin and insertion
Semitendinosus is a relatively large muscle that originates from a small facet on the rough superolateral surface of the ischial tuberosity. The tendon of the semimembranosus appears at the level of the mid-thigh and continues caudally toward the point of insertion at the medial condyle of the tibia.
There are interesting structural details of semimembranosus that help in identifying the muscle grossly. The muscle begins as a flat and membranous structure that develops a fleshy belly about midway down the thigh. The fleshy component is medially related to its tendon and the fibers are oriented inferomedially. The tendon actually trifurcates distally to give:
the main part that inserts on the medial tibial condyle, a second part that fuses with the popliteal fascia, and a third part that becomes the oblique popliteal ligament.
Another important feature of the semimembranosus is that its lateral border forms the superomedial Wall of the popliteal fossa.
Relations
The semimembranosus muscle has numerous adjacent muscular and neurovascular structures along its course. Semimembranosus is deep to semitendinosus, superficial to adductor magnus, and medial to biceps femoris along its entirety. The proximal part of the muscle is covered by the gluteus maximus and medial to adductor minimus. Distally, semimembranosus crosses over and becomes medially related to the medial head of gastrocnemius before inserting on the medial tibial condyle. The distal portion of the semimembranosus is also medial to the adductor canal (hiatus), which accommodates the vessels of the lower limb.
There is a U-shaped bursa that encompasses the semimembranosus tendon. It separates the tendon from the medial tibial plateau, medial head of gastrocnemius, semitendinosus, and the medial cruciate ligament.
Innervation
Semitendinosus is innervated by the L5, S1, and S2 nerve roots. These fibers access the muscle through the tibial division of the sciatic nerve.
Blood supply
The femoral and popliteal arteries give off deep perforating branches that supply the semimembranosus muscle. Occasionally, the inferior gluteal artery supplies the proximal part of the muscle.
Venous Drainage
The profunda femoris vein’s perforating veins, which empty into the femoral vein, are responsible for the semitendinosus muscle’s venous drainage.
Palpation
Semitendinosus lies deep to Semimembranosus and is difficult to palpate, but can be felt easier when the knee is flexed.
Functions
Semitendinosus extends across both the hip and knee joints and is consequently responsible for multiple movements about the joints. However, semimembranosus works in conjunction with the other hamstring muscles to carry out its function. When the feet are firmly planted on the ground, semimembranosus causes extension at the hip, which pulls the upper torso to go into an erect position.
Semimembranosus (along with semitendinosus) can also cause internal rotation of the thigh when the hip is fully extended. When the legs are suspended off the ground, it causes flexion of the knee and internal rotation of the leg on the thigh.
The Semitendinosus muscle and the other posterior thigh muscles are inactive whenever an individual is standing symmetrically. However, once the individual tilts too far forward, the Semitendinosus muscle is activated and counteracts the forward movement; thus stabilizing the hip.
Embryology
The germ layers of the embryo are called ectoderm, endoderm, and mesoderm during the gastrulation stage. The skeleton, with the exception of the skull, and striated skeletal muscle are uniquely developed from the paraxial mesoderm. Thus, the muscle that makes up the semitendinosus and its bony insertions originate from the mesoderm.
The lower limb starts to take shape as a whole toward the conclusion of the fourth week of the embryonic stage. As the embryo moves from the prenatal to the fetal stage during the eighth week, the limb keeps growing and becomes well-differentiated.
Anatomical Variations
Case studies have documented differences in the semitendinosus muscle’s anatomy. In one such instance, the semitendinosus muscle released an extra tendinous connection during the graft harvesting process during anterior cruciate ligament reconstruction surgery.
In addition to its original insertion, the gracilis tendon was attached to the muscle’s additional tendinous slip at the semitendinosus muscle’s insertion location. The semitendinosus tendon received a second tendinous insertion from the gracilis, who did the same.
There was a “double” pes anserinus as a result. The semitendinosus tendon has also been observed to insert into the leg’s crural fascia as opposed to the superior anteromedial tibia.
Stretching of Semitendinosus muscle
‘The Forward Bend’. Standing, (perform all of these movements in a relaxed way. There is no need to over-reach or force this stretch initially). Keeping the knees ‘locked out’ and the spine flat bend forward at the hips and just relax towards your toes, gently lengthening your hamstrings. To increase the intensity of the stretch, gently contract your quadriceps and reach for your toes or try To place your hands upon the floor.
Hamstring Stretch
Standing upright, facing a bench, table, or horizontal bar, flex your hip and ‘locking out’ your knee, and place this straight leg upon the anchor point. To increase this stretch, lean forward at the hip and reach toward the toes.
Functional movements
Stand from sitting
Walking upstairs
Standing jump forwards
Standing jump upwards
Hamstring Syndrome
This pathology commonly affects athletes who present with localized pain near the ischial tuberosity. The pathophysiology is thought to be that of an insertional tendinopathy at the ischium but there may also be involvement of sciatic nerve compression. The pain in hamstring syndrome radiates down the posterior thigh or popliteal region and is exacerbated when the hamstrings are on tension. This is often seen in sprinters or hurdlers. On examination there is exquisite tenderness over the ischial tuberosity and percussion in that region may reproduce the sciatic distribution of pain. Treatment involves rest, anti-inflammatory agents, and steroid Injections.
Baker’s cyst
The bursae that separate the muscle from the medial head of the tibia and the medial head of The Gastrocnemius may at times become enlarged with distended fluid. This swelling is termed ‘Baker’s cyst’ (described by Morrant Baker in the 19th century as a cystic mass in the popliteal fossae of children
Straight leg raise
The patient is positioned in supine with the hip and knee extended. One hand is placed over the anterior thigh to maintain full extension throughout the movement. The hip is flexed until firm muscular resistance to further motion is felt. A goniometer can then be aligned as follows:
Stationary arm: Lateral midline of the trunk
Axis: Greater trochanter of the femur
Moving arm: Lateral epicondyle of femur
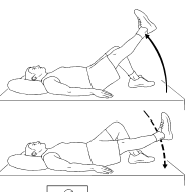
Knee extension test
The patient is positioned in supine with the hip to 90o and the contralateral limb should be placed on a supporting surface with the knee extended. The knee is then extended through full range of motion whilst the hip is maintained in 90o flexion.
Active test: the patient performs active knee extension of the knee until myoclonus is observed in the hamstring
Passive test: the knee is passively extended until firm muscular resistance to further motion is felt.