
Shoulder Impingement Syndrome and Physiotherapy Management
- Shoulder impingement is a common cause of shoulder pain. It’s also known as impingement syndrome or swimmer’s shoulder since it’s common in swimmers. It’s also common in other athletes who use their shoulders a lot, such as baseball or softball players.
Anatomy related to Shoulder impingement
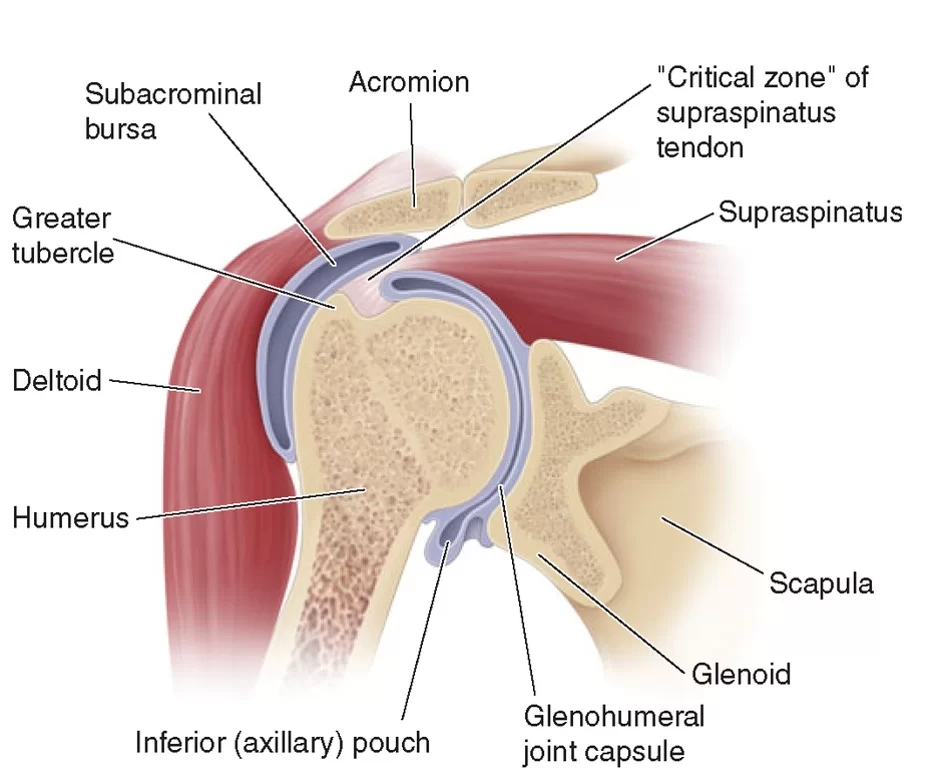
- The actual cause of shoulder impingement is the narrowing of subacromial space.let’s know about subacromial space.
- The subacromial space lies below the coracoacromial arch and above the humeral head and greater tuberosity of the humerus. The coracoacromial arch consists (lateral to medial) of the acromion, the coracoacromial ligament (anterior to the acromioclavicular joint), and the coracoid process.
- Within the subacromial space run the rotator cuff tendons, the long head of the biceps tendon, and the coracoacromial ligament, all surrounded by the subacromial bursa which helps to reduce friction between these structures.
- Your rotator cuff is a group of muscles and tendons that attach your upper arm bone to your shoulder. They help you lift and rotate your arm. The rotator cuff sits under the top of the shoulder.
- If you have shoulder impingement, your rotator cuff catches or rubs against the acromion. When you lift your arm, the space (bursa) between the rotator cuff and acromion narrows, which increases pressure. The increased pressure irritates the rotator cuff, leading to impingement.
Causes of Shoulder impingement
- Mostly shoulder impingement is caused by overuse. Repeated use of the shoulder can make the tendons in your shoulder swell. leading to the narrowing of subacromial space and irritation of subacromial bursae as well as rotator cuff muscle tendons.
- Intrinsic mechanisms involve pathologies of the rotator cuff tendons due to tension, including:
- Muscular weakness: Weakness in the rotator cuff muscles can lead to muscular imbalances resulting in the humerus shifting proximally towards the body and narrowing subacromial space.
- Overuse of the shoulder: Repetitive microtrauma can result in soft tissue inflammation of the rotator cuff tendons and the subacromial bursa. leading to friction between the tendons and the coracoacromial arch.
- Degenerative tendinopathy: Degenerative changes of the acromion can lead to tearing of the rotator cuff, which allows for proximal migration of the humeral head.
- Extrinsic mechanisms involve pathologies of the rotator cuff tendons due to external compression, such as:
- Anatomical factors: Congenital or acquired anatomical variations in the shape and gradient of the acromion.
- Scapular musculature: A reduction in the function of the scapular muscles, particularly the serratus anterior and trapezius. that normally allows the humerus to move past the acromion on the overhead extension. may result in a reduction in the size of the subacromial space
- Glenohumeral instability: Any abnormality of the glenohumeral joint or weakness in the rotator cuff muscles can lead to superior subluxation of the humerus, causing increased contact between the acromion and subacromial tissues.
Symptoms of Shoulder Impingement
- The main symptom of shoulder impingement is sudden pain in your shoulder when you lift your arm overhead or backward. Other symptoms include:
- minor but constant pain in your arm
- pain that goes from the front of your shoulder to the side of your arm
- Shoulder pain that gets worse at night
- shoulder or arm weakness
- difficulty in reaching out overhead
- pain while dressing, undressing
- The pain is classically exacerbated by abduction in the affected shoulder and relieved by rest and may be associated with weakness and stiffness secondary to the pain.
Risk of impingement
- Playing sports that require using your shoulders for overhead or forceful motion is the biggest risk factor for developing shoulder impingement. Common activities that could cause this include:
- swimming
- tennis
- baseball
- Occupations that require lots of heavy lifting or arm movement also increase your risk.
- These include:
- construction work
- moving boxes
- painting
- Both old age and previous shoulder injuries, such as a dislocation, are also risk factors for shoulder impingement. Some people also have an unusually shaped acromion that increases their risk.
Differential Diagnoses
- Muscular tear (e.g. rotator cuff tear, long head of biceps tear) – the weakness will persist despite the shoulder pain being relieved
- Neurological pain (e.g. thoracic outlet syndrome, cervical radiculopathy, brachial plexus injury) – any weakness will likely be associated with paraesthesia and/or pain, yet the weakness will persist despite the shoulder pain being relieved
- Frozen shoulder syndrome (adhesive capsulitis or calcific tendinitis) – Stiffness will persist even if the pain is relieved. Restriction of active as well as passive range of motion.
- Acromioclavicular pathology (e.g. acromioclavicular arthritis, glenohumeral arthritis) – presents with more generalized pain, also with weakness and stiffness related to pain known cause.
Diagnosis of Impingement syndrome
- Your doctor may start by asking you some questions about any previous injuries as well as your exercise habits. Next, they may ask you to do a series of motions using your shoulder while they check for any unusual movement. This will also help your doctor rule out other conditions, such as a pinched nerve.
- In some cases, you may also need an X-ray to rule out arthritis or check for bone changes. such as a spur, that could lead to impingement.
- If your doctor thinks that you have a more serious rotator cuff injury or they still can’t diagnose you, they might use an MRI scan to get a better look at your shoulder.
Treatment of impingement
- There are many types of treatment available for shoulder impingement, depending on how severe your case is.
Physiotherapy management
Electrotherapy modalities will provide pain relieve

- Ultrasound: ultrasound is a therapeutic modality that generates ultrasound that causes deep heat, and provides micro-massage to soft tissue. It increases flexibility, promotes the healing of tissue, and improves localized blood supply to the area. and ultimately pain relief.
- TENS: transcutaneous electrical nerve stimulation is an electrical modality that provides pain relief by providing pain modulation.TENS closes the gate mechanism at the anterior grey horn in the spinal cord. also stimulates the endogenous opioid system which prevents the release of substance p at the anterior grey horn.
- LASER: Low-level laser therapy is a form of medicine that applies low-level lasers or light-emitting diodes to the surface of the body. it decreases nerve sensitivity by decreasing bradykinin; a pain eliciting chemical. It normalizes ion channels [cellular gatekeepers] and releases endorphins [body’s natural pain reliever] and enkephalins [related to endorphins] that produce an analgesic effect. It also has a pain-blocking effect on certain nerve fibers.
- Shoulder impingement usually responds well to exercise therapy, which uses gentle exercises to rebuild strength and range of motion.
- In the initial stage, pain-free active exercise will provide relaxation to shoulder muscle.
- isometric shoulder exercise to maintain the power of shoulder muscles
- stick exercise or active assisted exercise will help to maintain an available range of motion
- strengthening exercise will help to regain normal power and endurance.
- strengthening exercise of the shoulder girdle and shoulder blade muscle.
- stretching exercises
Strengthening/Stretching Exercise :
- sit on the table with your arm at the side and squeeze your shoulder blade and hold it for 5 sec, repeat 10 to 20 times.
- Lie on your unaffected side and bend your top arm at a 90-degree angle. Keep your elbow on your hip and rotate your lower arm up toward the ceiling. Repeat 10 to 20 times.
- sit on the table put your both hand in your lap and now shrug your shoulder.
- shoulder depression
- Stand in a doorway, holding the side of the frame with your arm slightly below shoulder height. Turn your upper body away from that arm until you feel a slight stretch, and hold.
- Anterior and posterior capsular stretching.
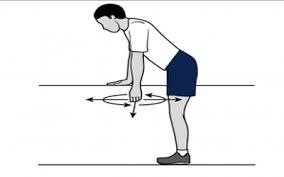
- pendulum exercise with lightweight.
- If any of these exercises cause pain, stop doing them or try holding them for a shorter period of time.
- Plyometric shoulder strengthening using theraband.
- Isokinetic exercises for Supraspinatous, infra Spinatous, Teres minor, and Subscapularis.
- Taping for scapular abnormal movement or scapular dyskinesis
- manual therapy approach: mobilization of the glenohumeral and scapulothoracic joint.
- stability and postural correction exercise for forwarding head posture or kyphosis.
Medication for Shoulder impingement
- Taking non-steroidal anti-inflammatory drugs, such as ibuprofen (Advil, Motrin), can help reduce swelling and shoulder pain. If these medications, along with ice and rest, don’t reduce your pain. your doctor might prescribe steroid injections to reduce swelling and pain.
Surgical management of Shoulder impingement
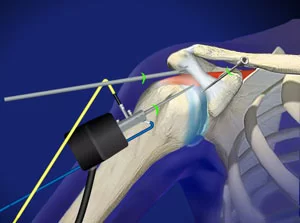
- If other treatments don’t seem to work, you may need surgery to widen the space around your rotator cuff.
- This allows it to move freely without catching or rubbing on your bone. This can usually be done with minimally invasive arthroscopic surgery, though more severe cases may need traditional open surgery. A recent study has questioned the benefit of removing the bone just for impingement.
- In rare, advanced cases of shoulder impingement, your rotator cuff can tear. If this happens, you’ll likely need surgery to repair the tear.
- Following any type of shoulder surgery, you may need to briefly wear an arm sling. Your orthopedic surgeon will determine when you can remove the sling.
Recovery time
- Shoulder impingement usually takes about three to six months to heal completely. More severe cases can take up to a year to heal. However, you can usually start returning to your normal activities within two to four weeks.
- Just make sure you regularly check in with your doctor to make sure you aren’t overdoing it. This can increase your recovery time or lead to other injuries.
Exercise do’s and don’ts
- Avoid any activities that involve throwing, especially with your arms overhead, such as tennis, baseball, and softball.
- You should also avoid certain types of weightlifting, such as overhead presses or pull-downs. If you’re a swimmer, you should take some time off from training to allow the recovery process to progress.
- Rest is very important when it comes to treating shoulder impingement. Avoid strenuous exercise or any movements that make the pain worse. This is especially important if you’re an athlete.
- Try placing an ice pack on your shoulder for 10 to 15 minutes at a time, a few times a day, to reduce pain and any swelling you might have.
Living with shoulder impingement
- While shoulder impingement can be painful and affect your daily activities, most people make a full recovery within a few months. In many cases, you’ll just need some rest and physical therapy. If those don’t provide relief, you may need surgery, which can add a few months to your recovery time.
- While shoulder impingement can be painful and affect your daily activities, most people make a full recovery within a few months
- In many cases, you’ll just need some rest and physical therapy. If those don’t provide relief, you may need surgery, which can add a few months to your recovery time.


13 Comments