

Teres Major muscle
What is Tere major muscle?
One of the seven scapulohumeral muscles is attached to the scapula and humerus. It is a muscle that is thick and somewhat flattened.
The humerus is supported in its medial rotation and extension by the teres major muscle, which means “rounded” in Latin. It is located above the latissimus dorsi muscle. This muscle is often mistaken for the rotator cuff muscle because, unlike the teres minor muscle, it does not attach to the capsule of the shoulder joint.
Origin of Teres Major muscle
The scapula’s dorsal surface inferior angle
Insertion
The humerus’s medial lip is in the intertubercular groove.
It is related to the muscle called the latissimus dorsi, which wraps around the teres major’s lower border. A bursa separates the teres’ major tendon from the latissimus dorsi tendon, which is located posteriorly.
Relations
The teres minor and infraspinatus muscles cover the posterior aspect of the scapular portion of the teres major. The subscapularis muscle connects the teres major’s anterior aspect.
The latissimus dorsi muscle’s superior border is parallel to the inferior margin of the teres major. In some people, the fibers of these two muscles that are next to each other may fuse. The teres major muscle, alongside the teres minor muscle, makes the posterior axillary fold. Sometimes even their insertion tendons or muscle bellies blend.
Innervation
The lower subscapular nerve (C5-C7), which is a branch of the brachial plexus, supplies the innervation of the teres major muscle.
Blood supply
The posterior circumflex humeral artery and the thoracodorsal branch of the subscapular artery vascularize the teres major muscle.
Function of Teres Major muscle
Teres major is primarily responsible for causing the humerus to move at the glenohumeral joint; it pulls the foremost surface of the humerus medially towards the storage compartment (inward revolution). The arm can also be extended from the flexed position.
When its humeral attachment is fixed, the teres major, pectoralis major and latissimus dorsi muscles can pull the trunk superiorly (through adduction). It is also known as the climbing muscle because of this. Furthermore, it adds to the adjustment of the shoulder joint.
Clinical aspects
The development of teres’ major injuries is connected to stretch or impact injuries to the teres’ major muscle, which can be caused by sports, motor vehicle accidents, or falls onto the lateral scapula.
Myofascial pain in the teres major muscle can also develop as a result of repeated microtrauma caused by reaching up and behind (such as injuries sustained while overhead throwing, picking up a briefcase from the backseat of a car, and in other sports).
Major injuries cause pain and difficulty with activities that require arm movements in the side or back.
Baseball and cricket players, particularly pitchers and bowlers, may experience isolated tears of the teres major, which are uncommon.
Sudden, sharp pain in the armpit, upper arm, and shoulder is the primary symptom of a teres major tear. This typically occurs when the muscle is not given rest or treatment.
The pain is usually dull and gets worse when you do things with your hands behind your back, like reaching in a back pocket, doing the downward freestyle stroke, pitching in baseball, or playing tennis.
Swelling may occur in the affected muscle region as a result of inflammation. Although the swelling is not visible from the outside, it can be felt when you touch the area (near the scapula’s bottom).
The sufferer’s arm range of motion is limited as a result of pain and discomfort in the upper arm.
A typical symptom is also an involuntary withdrawal of the stimulated muscle known as the jump sign.
When proper warm-up is not performed before workouts, teres major strain frequently occurs.
The teres major is overactive and small in individuals with upper-crossed syndrome (UCS).
One of the four rotator cuff muscles that are involved in numerous shoulder disorders, including quadrangular space syndrome, is the teres major.
Assessment
Palpation
While the patient is lying down and your arm is off the side of the table, grasp the latissimus dorsi with your fingers and thumb. Move your fingers and thumb medially to the lateral border of the scapula. Follow these fibers up towards the axilla, where they blend with the latissimus dorsi.
Length Tension Testing
Stabilize the scapula along the lateral border with the other hand and externally rotate the arm with the hand holding the forearm while the patient is in a supine position. The scapula-stabilizing hand and the moving hand are used to measure muscle tension and barrier.
Teres major stretching exercise
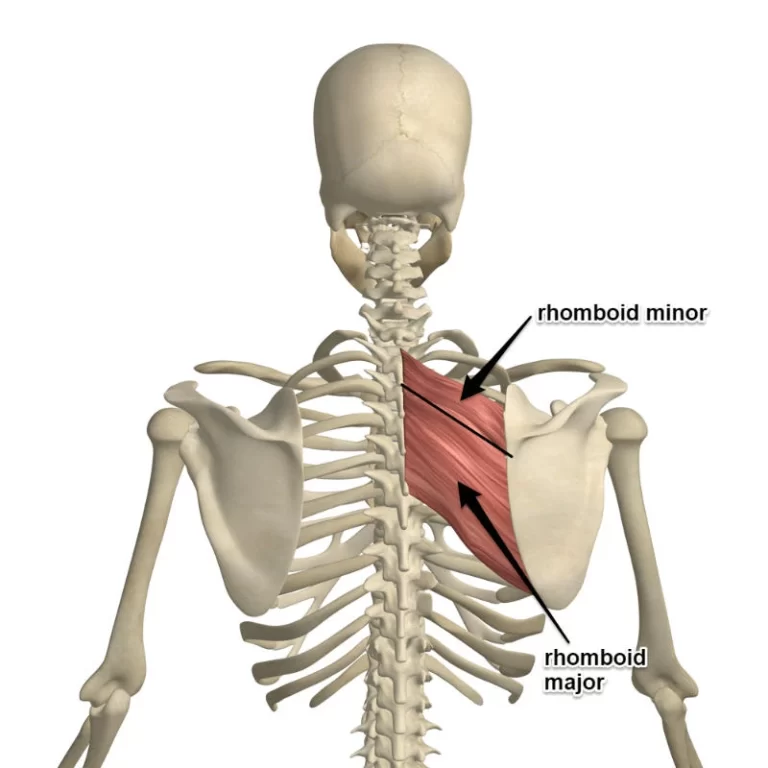
Shoulder Blade Squeeze
The Shoulder Blade Squeeze can help you improve your posture, increase your flexibility, and alleviate pain in the upper back by strengthening your Teres Major muscle. Not only will you be able to move around more easily, but you’ll also feel less pain in your shoulders!
To start, stand erect with your arms loosened up before you at shoulder level.
The next step is to squeeze together your shoulder blades and hold for five to ten seconds.
Relax and go through this sequence a few times, lengthening each squeeze as you get more used to the exercise.
This exercise can help you stretch your upper back and relieve tension in the teres major muscle consistently.

Teres major strengthening exercise
Isometric shoulder extension
This is a work-based isometric constriction practice that utilizes a wall. With your elbows straight, stand against a wall with your back to it. Press backward into the wall with your palms facing the wall for three seconds by gradually increasing your strength. Maintain your maximum tolerable contraction for 5-7 seconds before gradually decreasing your strength to rest (again over a count of three seconds).
Banded shoulder internal rotation
This is a shoulder inner pivot practice that is finished in shoulder flexion. To begin, hold the other end of a band close to the anchor point and anchor it beside you at about eye level. Pull the band into the internal rotation as you raise the elbow to 90 degrees of flexion. To complete a repetition, hold the end range for up to two seconds and then reverse the motion.
Childs pose sliders
This is an exercise for shoulder stability. Put your hands on a slider disc or a towel to start. Lean down with your torso from a quadrupedal position and slide your hand to an overhead position on the ground at the same time. To lift the torso off the ground, press down into the floor and draw the hand back down.

Prone press slider
The internal rotators of the shoulder are the primary targets of this dynamic shoulder stability exercise. To begin, lie on your stomach with your forearm supporting your head. To press the target arm against the floor, press it into a sliding disc or hand towel. While keeping up with the descending tension, slide your hand over your head to the extent that you can endure. Then slide it back down so your hand is generally following your shoulder.

Internal rotation pull down
Utilizing a strength band is a strengthening exercise for the internal rotation of the shoulder. Attach a band to a steady pull-up bar above you. When you raise your elbow to 90 degrees of abduction, line it up with your fist and elbow. Take hold of the band and pull it straight down without lowering your elbows. Slowly rotate back up, and do it again as necessary.

Abducted shoulder internal rotation
This is a strengthening activity for shoulder internal rotation. Position a band behind you so that it is about ear height. Keep the elbow flexed to 90 degrees and abducted to bear level. Hold the free end of the band with your fist elevated just above your elbow. Move forward to increase the band’s tension. Move your forearm down until it is parallel to the floor. Recount as required.
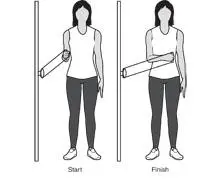
Dowel shoulder external rotation stretch
The purpose of this dowel-assisted exercise is to strengthen the shoulder joint’s passive external rotation. With your elbow flexed and shoulder flexed at 90 degrees, hold a broomstick or dowel. The stick shoulder is hung on the external part of your arm. Utilize your other hand to pull the dowel from beneath to extend the shoulder in an outside rotation.
Side lean wall slide
This is an exercise for strengthening and actively supporting shoulder abduction to resist adduction. To begin, align your body so that you are standing parallel to the wall. With your palm resting on a towel or slider disk, stand at arm’s length away from the wall. Move the hand up the wall at the same time as you slowly lean toward the wall. The body should then be brought back to a standing position by pushing the hand against the wall downward. Rely on the downward pull of the arm to move the body to an upright position rather than using the momentum from the hips to return to the standing position.
Banded walkouts
An isometric contraction of the internal rotators is the focus of this shoulder stability exercise. Position a band behind you so that it is about ear height. Keep the elbow flexed to 90 degrees and abducted to shoulder level. Hold the free end of the band with your fist elevated just above your elbow. To increase the band’s tension, step forward and hold the position for up to 10 seconds without moving. Take a step back to release tension in the band and rest for ten seconds before starting over.
Internal rotation side step
An isometric contraction of the internal rotators is the focus of this shoulder stability exercise. Place a band about elbow height in front of the target arm. Keep the elbow straight below the shoulder and flexed to 90 degrees. Grasp the free finish of the band and hold it so your clenched hand is straightforwardly before your elbow. Make a move to the side to add strain to the band and stand firm on this band without separating position for 10 seconds. To relieve the band tension, step backward and rest for ten seconds before performing the exercise again.
Banded shoulder internal rotation
A concentric and eccentric contraction of the internal rotators is the focus of this shoulder-strengthening exercise. Place a band about elbow height in front of the target arm. Keep the elbow straight below the shoulder and flexed to 90 degrees. To increase the band’s tension, grasp the free end and step to the side. Pull the band inwards until your clenched hand is before your midsection and afterward permit the band to pull your shoulder to end range external rotation.
FAQ
What signs and symptoms does a major injury have?
Pain and tenderness in the upper back and shoulder, weakness or difficulty moving the arm, and swelling or bruising in the affected area are the most common signs of a teres major muscle injury.
Teres major activation: what is it?
Findings: Teres Significant initiation adjusts both to neurotic and post-medical procedure conditions: During forward flexion or abduction, the normal activation shifts to activation. Teres’ Major transfer success after surgery seems to be due to glenohumeral stabilization rather than abduction torque.
How long is teres significant healing?
Specified two instances of separated teres significant wounds between the myotendinous intersection and the addition of the ligament on the humerus in proficient significant association baseball pitchers. The athlete was able to resume full sports participation after completing a structured, progressive rehabilitation program lasting eight to ten weeks.
Is major teres in need of surgery?
Although the significance of the teres major in upper extremity function is debatable, all known cases have been successfully treated without surgery.
What is the main adversary of the Teres major?
The teres major: agonistic: lower trapezius, serratus anterior, pectoralis major, and latissimus dorsi. antagonistic: pectoralis minor, middle deltoid, middle trapezius, and anterior deltoid.




2 Comments