
Upper Cross Syndrome
What is an upper cross syndrome?
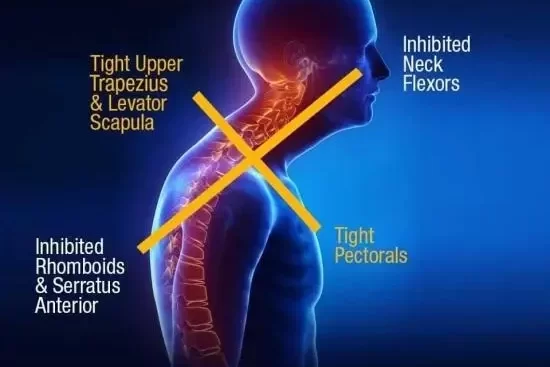
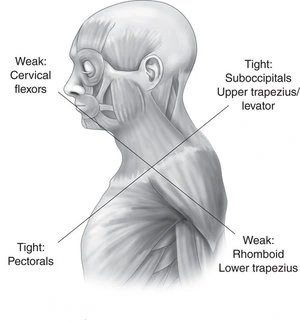
- Upper crossed syndrome is the muscles of the shoulders, neck & chest have become deformed. Specifically, the back muscles of the neck & shoulders (upper trapezius, and levator scapula) become extremely overactive & strained. The muscles in the front of the chest (the major and minor pectoralis muscles) become shortened & tight. As a result of these overactive muscles, the surrounding counter muscles become underused & weakened. In upper crossed syndrome, this causes weak muscles in the front of the neck (cervical flexor muscles) & in the lower shoulders (rhomboid and lower trapezius muscles). The condition gets its name from the “x” shape that develops when regions of overactive & underactive muscles overlap.
Mechanism of Injury / Pathological Process
- Muscle imbalance usually occurs before functional dysfunction also describes this muscle imbalance as a condition in which some muscles become inhibited & weak and others become short & stiff. Such imbalance can bring changes in tissues, which may cause inappropriate motion patterns in the individual. Such conditions can eventually cause side effects such as pain & inflammation and attribute these predicted patterns to a large extent, due to the immobile conditions & repetitive tasks. Muscle balance can be defined as the relative equality of muscle length or strength between an agonist & an antagonist; this balance is necessary for normal movement & function.
- In this syndrome, mainly the posterior superior muscles in the neck & the anterior neck, which are tonic, are short & the anterior deep muscles of the neck & posterior shoulder girdle, which are mainly phasic, are inhibited & weakened. This condition is caused by the changes in the elevation, protraction & abduction of the shoulder by increasing the angle of the forwarding head & hyperextension of the upper part of the cervical spine, which is often associated with forwarding head, round shoulder, protracted scapulae & thoracic kyphosis. These muscle imbalances & movement dysfunctions may have a direct effect on joint surfaces, thus potentially leading to joint degeneration. In some cases, joint degeneration may be a direct source of pain, but the actual cause of the pain has been often secondary to muscle imbalance.
- Muscles may become imbalanced as a result of adaptation or impairment. some muscle unbalance can be either pathological or functional.
- Functional muscle imbalances occur in response to adaptation to complex movement patterns, including imbalances in the strength or flexibility of antagonistic muscle groups. The structural approximate focuses on actual injuries to musculoskeletal structures such as rotator cuff tendonitis or a ligament injury. The functional approximate examines factors that contribute to structural lesions. This approximation is most useful for physical therapy management of chronic ‘dysfunctions’ such as persistent joint pain & tendonitis.
- Pathological muscle imbalance typically is associated with dysfunction & pain, although its cause may or may not result from an initial traumatic event. The pathological unbalance may also be insidious; many people have this muscle unbalance without pain. Ultimately, however, pathological muscle unbalances leads to joint impairment and altered movement patterns, which in turn lead to pain. Note that this muscle unbalance continuum may progress in either direction; muscle unbalance may lead to altered motion patterns & vice versa. Some damages cause muscles to unbalance, while others may result from muscle unbalance. Sometimes pathological unbalances are functional compensation for an injury. For example, unbalanced biomechanical joint stresses that result from muscle imbalance may lead to joint damage, setting up a vicious cycle of pain & inflammation. The structural inflammation then affects the neuromuscular system of the joint, creating further impairment. Eventually, the body adapts the motor program for movement to compensate for the impairment. The functional cause of the problem is muscle imbalance, while the symptom is pain & inflammation resulting from a structural lesion. Therefore, it is possible to have both a structural & a functional lesion, but for accurate diagnosis & treatment, the clinician must decide which lesion is the actual cause of dysfunction.
Clinical Presentation
- Individuals who present with the upper crossed syndrome will show a forward head posture (FHP), hunching of the thoracic spine as well as changed function in the shoulder girdle, elevated & protracted shoulders, scapular winging & decreased mobility of the thoracic spine. FHP, round shoulder, and kyphosis are postural deviations including excessive neck protraction & thoracic spine flexion, anterior tilt, and downward rotation of the scapula with an inclining tendency & internal rotation of the shoulder. FHP is related to thoracic kyphosis. In addition, a relationship between the FHP & round shoulder as well as round shoulder & kyphosis has been reported. However, it is not possible to determine which one is the cause & which one is the effect. In upper cross syndrome, the head is laid in a forward head posture.
Weak muscles:
Lower & middle trapezius.
Serratus anterior, decreased SA activity will be accompanied by a reduction in control of the scapula in static & dynamic states.
Infraspinatus
Deep neck flexors play a key role in supporting the neck’s posture. These muscles are weak & prolonged in people with FHP & are not properly recruited.
Tight muscles:
Upper trapezius, an increase in the UT activity increases the anterior tilt of the scapula & elevates it, leading to a decrease in subacromial space, which increases the probability of shoulder pathology.
Pectorals and tightness of the pectoralis major generate an anterior force on the glenohumeral joint with a consequent decrease in stability. A tight pectoralis minor limits scapular upward rotation, external rotation & posterior tilt, thereby reducing subacromial space.
Levator scapulae, shortness of the levator scapulae may affect muscle coordination and increase shear force and compressive load in the cervical spine
What is a diagnosis of upper cross syndrome?
- In clinical practice, it is advisable to begin muscle evaluation by analyzing upright standing posture & gait. The clinician is given an overall view of the patient’s muscle function through posture & gait analysis & is challenged to look overall at the patient’s entire motor system & not to limit observation to the local level of the lesion
- Muscle analysis of standing posture: posterior, anterior, and lateral view
- Evaluation of balance.
- Hypermobility.
- Evaluation of muscle unbalance in a patient with acute severe pain syndrome, however, is unreliable and must be undertaken with precaution. A precise evaluation of tight muscles & motion patterns can be performed only if the patient is pain-free or almost pain-free. Its usefulness is considerable in the chronic phase or in patients with repeated pain after the acute episode has subsided.
Upper-Quarter Muscles
- The muscles of the upper quarter involve those of the cervical spine, shoulder, and arm. The muscles prone to tightness are those included in a protective flexor response. Tightness of the upper trapezius, pectoral muscles & suboccipital, in particular, is a hallmark sign of Janda’s UCS.
- The upper trapezius muscle is tested with the patient supine, with the head passively flexed & side-bent to the contralateral side. Once the slack is taken up, the shoulder girdle is pushed distally. Normally, a sort barrier is felt at the end of the push; however, when the motion is restricted, the barrier has an abrupt firm to hard end-feel.
- Levator scapulae muscle is examined in a similar manner, except that the head is also turned to the contralateral side.
- The deep posterior neck of muscles can be tested only by thorough palpation. Evaluation of the sternocleidomastoid is not dependable because it crosses too many parts segment.
- Pectoralis major muscle is tested with the patient in a supine position. The trunk must be secured before the arm is placed into abduction because a possible rotation of the trunk might mimic the normal range of motion. The arm should reach the horizontal level. To estimate the clavicular portion, the arm is allowed to hang down loosely & the examiner applies a posterior glide to the shoulder. Normally, only a slight soft barrier is noticed. The different portions of the pectoralis major are tested individually and the clinician is able to target specific parts by exchanging the amount of shoulder abduction.
1. Lower sternal fibers. The therapist abducts the patient’s arm to 150° with slight external rotation. The normal length of these pectoral fibers allows the patient’s arm to relax in a horizontal position; slight overpressure produces end-feel resistance. The therapist should also touch the sternal fibers medial to the axilla for tenderness. Shortness of hypertonicity of the muscle is indicated by an inability of the arm to reach horizontal or a touchable tenderness in the muscle.
2. Midsternal fibers. The therapist abducts the patient’s arm to 90° & palpates the muscle fibers at the second rib interspace. The normal length of these fibers allows the patient’s arm to relax below the horizontal motion. There is gradual end-feel resistance when the therapist applies slight overpressure. Palpation does not produce tenderness.
3. Clavicular fibers. The therapist places the patient’s arm in an extended position close to the body & allows the arm to come to a rest. The normal length of these fibers allows the patient’s arm to relax below the horizontal. The therapist applies gentle anteroposterior & caudal pressure through the glenohumeral joint as well as touches the fibers just inferior to the clavicle. Resistance to this pressure should be gradual & fibers should not be tender to palpation.
- Pectoralis Minor muscle is tested with the patient supine. The therapist views the mark on the patient from a superior view. The normal distance between the acromion & the table is 1 inch. The horizontal levels of the anterior aspects of the acromion process can be compared with each other. The two acromions process should be on the same level. the higher acromion indicates possible pectoralis minor tightness.
- Latissimus Dorsi muscle is tested with the patient supine. The therapist stands beside the arm being tested. The therapist passively elevates the patient’s arm toward the head of the table. The normal length of the latissimus dorsi allows the arm to relax horizontally on the table with the lumbar spine flat on the table. The tightness of this muscle is indicated by the arm relaxing above the horizontal and by the lumbar spine going into the extended position.
What are the causes of upper cross syndrome?
- Typically, poor posture causes the syndrome, including the forward head posture, which occurs when people use electronic devices, read, and drive. Those with the upper crossed syndrome usually have the same or similar set of postural irregularities that people may describe as slouching.
- Different motions can cause the upper crossed syndrome, but most cases develop through poor and weakened posture, specifically for sitting or standing with the head forward for prolonged periods.
Activities that promote this postural position include:
- computer and laptop use
- driving
- watching TV
- cellphone browsing, texting, app, or game use
- reading
- biking
- In some cases, injury or congenital disorder may also contribute to the occurrence or creation of the condition.
What are the symptoms of upper-crossed syndrome?
Common characteristics of upper crossed syndrome include:
- The head is continuously or often in a forward position. Inward curvature in the part of the spine containing the neck (increased cervical lordosis). Outward curvature in the portion of the spine that includes the upper back, shoulders, and chest (increased thoracic kyphosis).Elevated, protracted, or rounded shoulders, where the muscles are in a constant state of being pulled or stretched forward. The visible portion of the shoulder blade sits out instead of laying flat (scapular winging). The deformed muscles associated with upper cross syndrome put stress on the surrounding muscles, tendons, bones & joints, causing most people to develop symptoms that include:
- headache
- neck pain
- strain in the back of the neck & often a weakness in the front
- chest pain & tightness
- pain in the upper back, especially in the shoulder joint
- sore shoulder blades
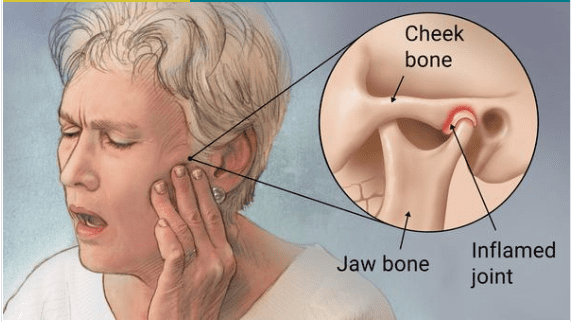
- pain in the jaws
- tiredness
- difficulty sitting, reading, and watching TV
- driving for more than a short period because of pain or muscle tightness or soreness in the muscle
- restricted range of motion in the neck or shoulders
- numbness, tingling & pain in the upper arms
- pain & reduced range of motion in the ribs
- lower back pain
Physiotherapy treatment
Pain management:
Electrotherapy can effective for pain management.
What is Electrotherapy?
Electrotherapy is a term for using mild electrical pulses to stop the pain in a point area of the body. Generally, all of these therapies use a device with electrodes to supply a low-voltage electrical current to pain areas.
The main goal of electrotherapy is pain management.
TENS (Transcutaneous Electrical Nerve Stimulation)
One of the most common electrotherapy devices use for pain relief. Small and sticky pads with electrodes are placed over or near the area where you sense pain. Your physiotherapist will decide the area of placement for electrodes. A series of low-voltage electrical currents send by the battery-operated unit to the area.
IFT (Interferential therapy):
interferential therapy is a pain-relieving modality without side effects.
Ultrasound therapy:
It is effective in neck pain patients who have trigger points over the trapezius muscle or are associated with myofascial pain syndrome. Ultrasound therapy inactivates the trigger points and decreases the tension of soft tissues.
Cervical traction:
Cervical traction help to relieve pain. It involves using weights to increase space between the cervical joints and also relieve the pressure on the cervical discs and nerve roots.
Exercises of the upper cross syndrome
Isometric exercises for the UCS:
You can perform these exercises while sitting, standing, or lying on your back.
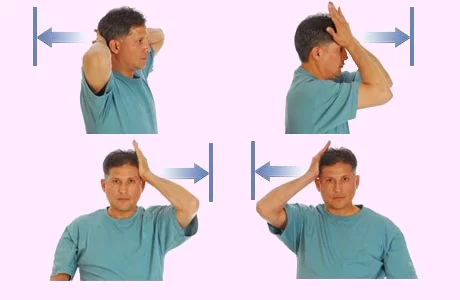
1. Cervical flexion:
Flex your neck slightly forward and place your hand on your forehead.
Try to flex your head forward while pressing back with your hand.
2. Cervical extension:
Keep your neck straight and put your hands at the back of your head.
Try to press your head backward while pressing forward with your hands.
3.Cervical side flexion:
Keep your neck straight and place your right hand on the right side of your head.
Try to carry your head down to your right shoulder while pressing up with your right hand.
Repeat the side flexion on both sides but for the left side press with your left hand.
4. Cervical rotation:
Put your right hand at chin level and turn your head slightly to the left.
Put your left hand on the left side of your face.
Turn your head to the left while pressing it back with your left hand.
Repeat the rotation on both sides but the right side of your face with your right hand. With specific exercises and stretches, your symptoms may relieved.
Physiotherapist focuses on stretching and strengthening your muscles and also correcting your posture.
Your physiotherapist will advise how long and how often you should practice these exercises, based on your individual symptoms and condition.
strengthening Exercises of the upper cross syndrome
- Assessment results can now be applied to design a program. The four-step corrective exercise process for UCS starts by inhibiting or resting the possible overactive muscles (usually through foam rolling) and lengthening these same muscles, followed by strengthening the complementing underactive muscles & finally, integrating the involved muscles to reestablish functional synergistic movement patterns.
- This four-step process of establishing a more ideal posture is a way of re-educating the body & in this case, the upper body. Generally, this corrective strategy works to increase the range of motion, improve local strength & assist the client in learning to better control the newfound range of motion. Added benefits also include a possible decrease in pain & discomfort, stability of the upper torso & improved physical performance in training & play. When the head, neck & shoulders are functioning better, so does the rest of the body.
STEP 1: Inhibit/Self myofascial release of overactive muscles
Upper Trapezius, Levator Scapulae & sternocleidomastoid hold pressure on tender spots for 30 seconds.

STEP 2: Lengthening lengthen/ static stretch
Upper Trapezius – Tuck the chin & slowly draw the left ear to the left shoulder.
Levator Scapulae – The rotating of the chin downward until a normal stretch is felt on the right side.
SCM – Same as above, except rotating chin upward.
Perform the sequence on both sides, holding each stretch position for 30 seconds

STEP 3: Activate / strengthen
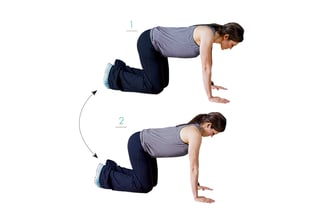
Chin Tucks – Get on hands & knees with back straight & head in line with the spine. Extend your chin toward the floor.
Scoop your chin down toward the chest as far as possible (like nodding “yes”). Keeping the chin close to the body, slide back into the starting position.
Floor Cobra – Lie on the floor, arms at the side of the body (or with arms in front of the body in a “Superman” position), palms facing toward the ground. Pinch shoulder blades together & lift the chest off the floor. Hold for 2 seconds. Slowly return the body to the ground and keep the chin tucked.


STEP 4: integrate
Ball Combination – Lie with your abdomen on a stability ball, keeping your feet pointed down & legs straight. Hold a dumbbell in each hand. Lift chest off the ball, keeping back & neck in a proper straight position. Extend arms in front of the body. Squeeze glutes & lift arms, keeping thumbs up & pinching shoulder blades back & down (scaption). Move arms straight out to the side with thumbs up and (abduction). Move arms toward to the side of the body with thumbs up and retract & depress shoulder blades (cobra).
Hold at each location, then return the arms to an extended position in front of the body (position 2). Repeat 10 times, for 1–2 sets.

postural exercise of UCS
Another exercise of the upper cross syndrome
- The best way to treat upper crossed syndrome is through core stability exercise & postural changes in the body. Though some people may feel a lot of discomfort when stretching exercise to prevent deformity, it is important that they attempt some form of gentle exercise and stretching as restricting activity can cause stiffness & soreness. People must ensure they warm up their tissues before exercising, either with gradual, gentle movement or by having a warm bath or shower. Begin all exercises gently & build up slowly.
Lying down exercise
Lie down with something such as a thick pillow or towel placed about a third of the way up your back, aligned with your spine straight. Allow your shoulders & arms to roll out & release and relax & your legs to fall open naturally and relax. Make sure your head is neutral and relaxed & does not feel strained or stretched to the muscle. If it does, use a pillow or support to relax the body. Remain in this position for 10-15 minutes, and repeat the exercise several times throughout the day.
Sitting exercise
Sit with a straight spine, and back and bend your knees, and relax with your feet flat on the floor. Press your palms down into the ground behind your hips and relax the body & rotate the shoulders down & back. You should feel the tight muscles of the side neck, shoulders & chest lengthen and relax. For more of a stretch in the chest, push your palms into the floor without actually moving them and further stretch move gently and relax. Stay in this position for 5 minutes, or as long as feels comfortable. Repeat the exercise and position it several times throughout the day.
Standing exercise
Stand with your feet about 3-4 feet apart and relax. Keeping your torso where it is, turns your right foot out 90 degrees & pivot your left foot inwards to about a 30-degree angle. With palms down and relaxed, place your arms at shoulder height in line with your legs and relax. Keeping your left leg & your torso straight, turn your head to look at your right fingers & bend your right knee as far as possible, but no more than 90 degrees.
Different types of neck stretch to relieve upper cross syndrome pain.
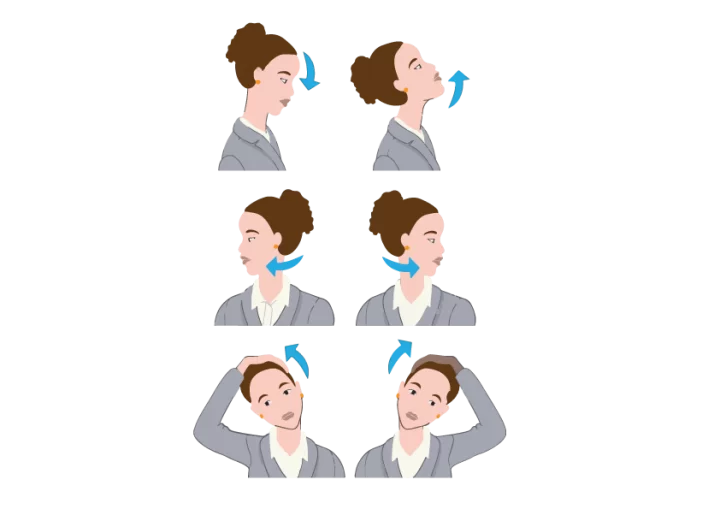
Forward and Backward Tilt
This can be done while you are seated or on your feet. Keep your movements smooth and slow.
- To Start this exercise your head should be squarely over your shoulders and your back should be straight.
- Lower your chin toward your chest and hold for 20-30 seconds. Go to the initial position, and slowly elevate your head back up.
- move your chin up toward the sky and bring the base of your skull toward your back. Hold for ten seconds, then return to the initial position.
- Repeat this maximum number of times. Do it in your daily activities.
Side Tilt
How to do it?
- This exercise can be performed in a standing position, with your hip-foot width apart and arms down by your sides.
- Smoothly tilt your head toward your left shoulder and try to touch it with your ear.
- Stop when you feel the stretch.
- Do not elevate your shoulder.
- Hold the stretch for five-ten seconds, then return to the initial position.
- Repeat on your right side. You can do several sets and work your way up to ten repetitions.
- To feel more stretch, put the hand on the same side of your tilted head on top of your head, and press lightly with your fingertips.
Side Rotation
How to do it?
- You can perform this in a sitting or standing position.
- Your head should be squarely over your shoulders and your back should be straight.
- Slowly turn your head to the left until you feel a stretch in the side of your shoulder and neck.
- Hold this stretch for thirty seconds, and then slowly move your head forward again.
- Repeat on your right side.
- Do up to ten sets.
Shoulder Roll
How to do it?
- You can perform this in a sitting or standing position. move your shoulders straight up and move them in a circle going forward.
- Do it six times. Return to the initial position, and make another six circles, this time you have to go backward.
Neck Flexion (Forward Bending)
How to do it?
- To perform this exercise you have to move your neck slowly toward the chest and look downward while only moving the head.
- Once the head has been flexed forward as much as it can comfortably go, hold this stretch for five seconds before returning to the initial position.
- The neck flexion stretch is felt throughout the posterior part of the neck.
Lateral Neck Flexion (Bending Side to Side)
How to do it?
- You can perform this in a sitting or standing position. Slowly flex the head to any one side, such as by bringing the right ear toward the right shoulder.
- While this stretch, the shoulders, and back remain steady while the neck bends laterally to the side.
- Once the head has flexed as much as it can comfortably go to the side, try to hold this stretch for five seconds before returning the head to the initial position. This same stretching is repeated on the left side.
- When the lateral neck flexion is performed with the head bending toward the right shoulder, the stretch is felt along the right side of the neck.
Neck Rotation (Turning Side to Side)
How to do it?
- To perform this exercise your back should be straight and your shoulders steady, slowly turn the head to the right as much as it can naturally go without increasing pain.
- Once the head has reached its rotation limit, hold the stretch for five seconds before bringing it back to the neutral position.
- This same stretching is repeated on the left side.
These all stretches are noted for a stiff neck, and rotation is often the most challenging, especially on one side or the other. it is only done with no pain, you have to rotate your neck in a comfortable position.
Neck Retraction
How to do it?
- Neck retraction can be performed in a sitting or standing position. Initiate this exercise by looking straight ahead and allowing yourself to relax.
- Your chin should be tucked down slightly and move your head smoothly backward until it is pulled back as much as you can without straining or feeling any pain.
- Continue looking straight ahead, being careful not to tilt the head forward or backward while doing this stretch.
- Maintain this position for three to five seconds and then return to the starting position.
- Repeat this stretch ten to fifteen times.
Seated Clasped Neck Stretch
How to do it?
- To perform this exercise you have to Sit comfortably on the ground or in a chair, making sure your body is in proper alignment your head should be stacked above your ribs and your pelvis. hold your hands and bring both palms to the back of your head.
- Gently press your hands down toward the floor, tucking your chin into your chest.
- Hold for at least thirty to forty seconds, or 7-8 deep, diaphragmatic breaths in and out.
- Seated clasped neck stretch targets your upper back and trapezius muscles. If you feel more stretched then pull with only a single hand in the middle of your head instead of both hands.
What is the prevention of upper cross syndrome?
The best way to prevent & treat upper crossed syndrome is to avoid activities that require stretching the head forward for extended periods of time.
Other tips for preventing upper crossed syndrome and pain reliving include:
- limiting time spent reading, driving, watching TV, or using laptops and computers
- taking breaks every 10-15 minutes while sitting or engaging in problem activities and workload.
- getting enough cardiovascular exercise, ideally 30-35 minutes daily from low-impact activities, such as walking or swimming and cycling.
- being aware of movements, motions, or activities that worsen and increase symptoms and avoiding them for as long as the discomfort continues and relaxing.
- doing stretches that target sore muscles of the back neck, shoulders, and chest and relax the body
- doing strengthening exercises to target weakened muscles in the upper front neck, and lower shoulders, and continuing and repeating 1-2 times per day
- making sure the steering wheel, book, TV, or computer screen is sitting at eye level
- using a lumbar roll in chairs
- using a headset for long telephone calls or transcribing and use the phone eye level.
- using a single pillow that retains its shape to body position is relax
- Correcting posture or practicing proper posture is also an important part of UCS avoiding and treating upper-crossed syndrome to correct posture.
Tips for Avoiding UCS in the Future
Start by practicing good posture, correcting posture being sure to avoid positions that create discomfort or numbness. In particular, don’t give slouching and poor posture a chance to become a habit.
- Here are some other things to try for better posture and good posture:
- Watch your weight.
- Wear shoes that offer support.
- Instead of leaning to reading your head down to look at a book or screen, raise the book or screen up to eye level to get a better posture.
- Set the height of your chair or desk to relax your neck and shoulder muscles so you can attain proper posture.
- If you sit for long periods of time, remember to take a break, relax your body, and stand and stretch the muscle every so often.
- If you stand for long periods of time, support one foot on a short table, and a sturdy object.
- When in bed, support your neck and lower back with pillows or rolled towels of that size.
- Exercise the muscles around your neck, shoulders, and chest at least 2-3 times per week.
- Try to exercise the muscles of your core, back, and abdomen, every day, even if just by taking a short walk.
Do’s and don’t for the upper cross syndrome (Neck care):-
- Maintaining a good posture
- Simple exercises to relieve pressure and strain on the structures within the neck – Gently stretch your neck from side to side or up and down
- Maintain a good overall health and nutrition status
- Don’t roll your neck
- Don’t bend your head to one side while talking on the phone
- Don’t use hard pillows while sleeping
Which pillow is Best for Neck care?
- Your sleeping position and pillow may play a role in Neck pain. Prone-position sleepers have higher chances of neck pain.
- Taking an Alternate position means your neck is turned to either side and your spine is in relaxed mode.
- For Pain relief, experts recommend trying to sleep either on your back or on your one side and choosing the Best pillow that helps support the neck.
FAQ
What is an upper cross syndrome?
When the muscles of your shoulders, neck & chest are out of balance and some too weak & some too tight that’s called Upper Cross syndrome (UCS). In side views of the upper body, these muscles seem to group in the shape of an X and which has led to the name of the condition.
What are the symptoms of upper cross syndrome?
Headaches.
Neck pain or strain in the back of the neck.
Chest pain and tightness.
Pain in the upper back, especially the shoulders.
Difficulty sitting and driving for long periods of time. reading or watching television
Restricted range of motion in the neck and shoulder joints.
Can upper cross syndrome be corrected?
Often referred to as, the upper crossed syndrome occurs when there is an imbalance in the neck, upper back, chest, & shoulders muscles. It is usually a result of poor posture or incorrect repetitive motion & with the proper, consistent corrective exercise, it can be corrected
What is the best remedy for someone with the upper cross syndrome(UCS)?
Treating UCS with physical therapy has been proven to work. In one case, researchers had 40 university students with the upper cross syndrome(USC) go through a therapist, and they found that the therapist helped. Almost all of the students became better aligned & could move their upper shoulder muscles more easily and comfortably.
Which of the following is a characteristic of upper crossed syndrome (UCS)?
Common characteristics of upper crossed syndrome include: the head being consistently or often in a forward position. inward curvature of the spine containing the neck (increased cervical lordosis)

10 Comments