
Ankle Lateral Ligament Injury and Physiotherapy Treatment
What is an Ankle lateral ligament injury?
- Lateral ankle sprains are referred to as inversion ankle sprains or as supination ankle sprains. It is usually a result of a forced plantarflexion/inversion movement, the complex of ligaments on the lateral side of the ankle is torn by varying degrees.
- Although the ankle sprain is a relatively benign injury, inadequate rehabilitation can lead to residual symptoms after lateral ankle sprain affects 55% to 72% of patients at 6 weeks to 18 months.
- The frequency of complications and breadth of longstanding symptoms after ankle sprain has led to the suggestion of a diagnosis of sprained ankle syndrome.
Anatomy-related Ankle lateral ligament injury
Bones:
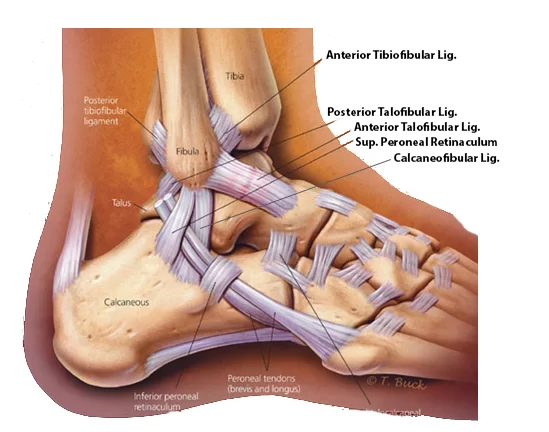
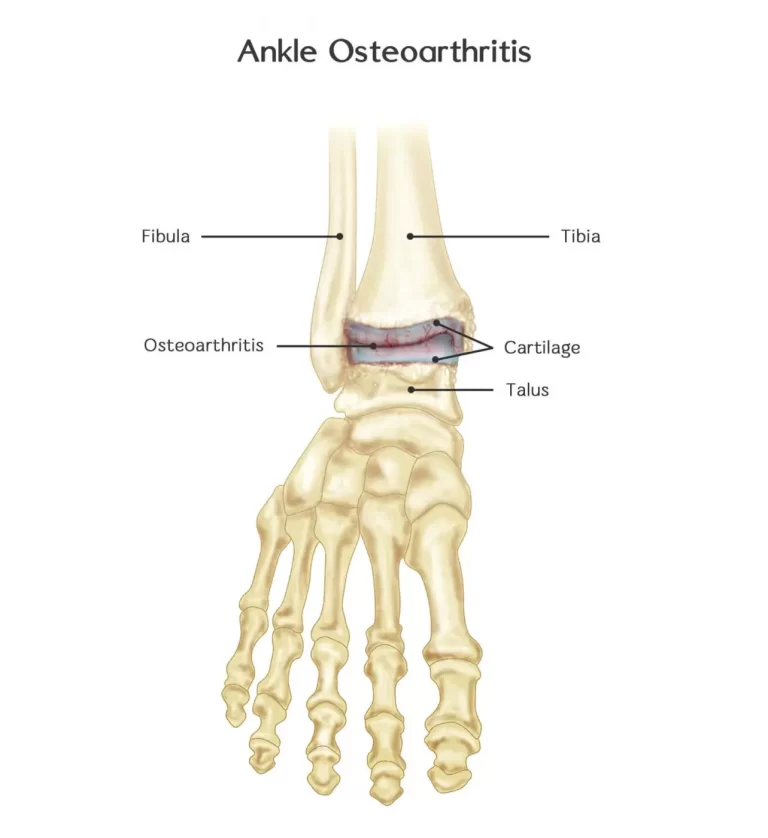
The bones that make up the ankle joint include the distal tibia and fibula (the medial and lateral malleolus, respectively) and the talus.
Joints:

- The Ankle Complex consists of 3 articulations The talocrural (ankle joint) ( Mortise joint) is a hinge joint between the inferior surface of the tibia and the superior surface of the talus.
- It allows the movements of plantarflexion and dorsiflexion(sagittal plane). The talocrural joint receives ligamentous support from a joint capsule and several ligaments, including the anterior talofibular ligament (ATFL), posterior talofibular ligament (PTFL), calcaneofibular ligament (CFL), and deltoid ligament.
- The ATFL, PTFL, and CFL support the lateral aspect of the ankle. Plantarflexion is the least stable position of the ankle joint, which explains why the majority of ankle injuries occur in this position.
- The inferior tibiofibular joint is the articulation between the distal parts of the tibia and fibula, where a small amount of rotation (transverse plane) is possible. The joint is stabilized by a thick interosseous membrane and the anterior and posterior inferior tibiofibular ligaments.
- The subtalar joint is an articulation between the talus and calcaneus and allows the movements of eversion and inversion (frontal plane). It also has an important role as a shock absorber. The ligamentous support of the subtalar joint is extensive, it is divided into 3 groups: (1) deep ligaments, (2) peripheral ligaments, and (3) retinaculum.
- Ligaments:
- The lateral ligaments of the ankle, composed of the anterior talofibular ligament (ATFL), the calcaneofibular ligament (CFL), and the posterior talofibular ligament.
- The medial (deltoid) ligaments are much stronger than the lateral ligament and are therefore injured much less frequently.
Muscles:
The following muscles are involved in moving the ankle joint:
- The calf group is made up of the gastrocnemius and soleus;
- Peroneus longus and peroneus brevis;
- Tibialis anterior.
Innervation:
- The motor and sensory supplies to the ankle complex stem from the lumbar and sacral plexus.
- The motor supply to the muscles comes from the tibial, deep peroneal, and superficial peroneal nerves. The sensory supply comes from these 3 mixed nerves and 2 sensory nerves: the sural and saphenous nerves.
Risk factors:
- Body mass index, slow eccentric inversion strength, fast concentric plantar flexion strength, passive inversion joint position sense, and the reaction time of the peroneus brevis were associated with significantly increased risk of a lateral ankle sprain.
Diagnosis of Ankle lateral ligament injury
The aims of the physical examination are to determine the:
- Amount of instability present by assessing the grade of the sprain;
- Loss of Range of motion (ROM);
- Loss of muscle strength;
- Level of reduced Proprioception.
Observation
- The physical examination begins with a general observation of the foot and ankle. Any signs of injury, inflammation, color changes of the skin, or atrophy/hypertrophy of the muscles are noted.
- After that, observation of the foot and ankle continues in two different positions non-weight bearing (n-WB) and weight-bearing (WB) positions.
- Make a note of the gait pattern, degree of limp (if any), the facial expression on weight-bearing, and any other signs that may provide more information about the injury.
History
- Taking an accurate history is an important step in determining the nature of the injury. A plantarflexion/inversion injury would indicate damage to the lateral ligament, whereas a dorsiflexion/eversion injury would indicate damage to the medial ligament.
- The previous history of injury on the same side will give clues as to whether the ankle was unstable too, begin with, or that a previous injury wasn’t properly rehabilitated. History of injury on the other side as well may indicate a biomechanical predisposition towards ankle injuries.
- Taking an accurate history is an important step in determining the nature of the injury. A plantarflexion/inversion injury would indicate damage to the lateral ligament, whereas a dorsiflexion/eversion injury would indicate damage to the medial ligament.
- The previous history of injury on the same side will give clues as to whether the ankle was unstable too, begin with, or that a previous injury wasn’t properly rehabilitated. History of injury on the other side as well may indicate a biomechanical predisposition towards ankle injuries.
Instability and grade
Ligament sprains can be of the following grades:
- Grade 1 – mild, painful, minimal tearing of the ligament fibers;
- Grade 2 – moderate, painful, significant tearing of the ligament fibers;
- Grade 3 – severe, sometimes not painful, complete rupture of the fibers.
- Range of motion (ROM)
- ROM of the ankle needs to be assessed actively and passively. The movements to be assessed are:
- Plantarflexion and dorsiflexion;
- Inversion and eversion
Palpation
- An important aspect of the initial examination is to determine the exact site of the lateral ligament sprain, whether it’s the ATFL, CFL or PTFL (usually damaged in that order).
- Palpating the lateral aspect of the ankle over the course of the various aspects of the ligament complex will provide detailed information on the exact location of the tear. Begin palpating gently as this can potentially be acutely painful for the patient.
Special Tests for Ankle lateral ligament injury
- An anterior draw is done to test the integrity of the ATFL and CFL. With the ankle in plantar flexion, the heel is grasped with the tibia stabilized and drawn anteriorly.
- Talar tilt is done to assess the integrity of the ATFL and CFL laterally and the deltoid ligament medially. Again the heel is grasped, the tibia stabilized and the talus and calcaneus are moved laterally and medially.
- Proprioception can be assessed in any number of increasingly difficult ways, beginning with a simple single-leg stance. The patient can do it on the normal side first, to allow the therapist to get an idea of what the normal is and then attempt on the injured side.
- This test can be progressed by asking the patient to reach outside their base of support (BOS), rotating their neck, or by closing their eyes. Moving onto a wobble board or any other unstable surface will allow the therapist to assess the patient’s ability to respond to a changing surface.
Treatment of Ankle lateral ligament injury
- According to Green et, al, the overall quality of the existing Lateral Ankle Ligament Sprain Clinical Practice Guidelines is poor with the majority out of date.
- Also, several inconsistencies in the interpretation of the evidence between the CPG development group and an absence of consistent methodology of CPGs present a barrier to implementation.
Reduce pain and swelling
- Initial management (i.e. within the first 48-72 hours) of an acute lateral ligament injury is to reduce pain and swelling by following the RICE regimen; Rest, Ice, Compression, and Elevation.
- If weight-bearing (WB) is too painful, the patient can be given elbow crutches and be non-weight bearing (NWB) for 24 hours. However, it’s important that at least partial weight bearing (PWB) is initiated relatively soon, together with a normal heel-toe gait pattern, as this will help to reduce pain and swelling.
- Gentle soft tissue massage can be performed to assist with the removal of edema and gentle stretches, as long as this is pain-free.
Restore ROM

- As soon as pain allows, the patient should begin pain-free active range of movement (ROM) exercises.
Return to functional activity
- Patients should be assessed for the ability to do the following activities pain-free:

- Twisting
- Jumping
- Hopping on one leg
- Running
- Figure of 8 running
- Before returning to full functional activity the patient should have a full range of pain-free movement in the ankle, normal strength, and normal proprioception.
- If returning to sports, the athlete should be encouraged to wear an ankle brace or to tape the ankle for a further 6 months to provide external support. Types of taping include a heel lock and a figure of 6.
FAQs
How long does a lateral ankle ligament take to heal?
Ankle edema and moderate discomfort usually subside within two to three weeks. Around the ankle, there is significant discomfort and edema. Recovery could take 3–12 weeks or more.
What are the symptoms of a lateral ankle ligament tear?
Symptoms of a lateral ankle ligament tear can include:
Pain is usually felt on the outside of the ankle and can vary in intensity depending on the severity of the tear.
Swelling around the injured area.
Bruising or discoloration can occur around the ankle
Instability: You might feel a sense of instability or giving way in the ankle
Difficulty bearing weight
Limited range of motion: You may have difficulty moving the ankle joint
Tenderness: The area around the injured ligaments may be tender to touch.
Difficulty with activities: Activities that involve twisting or turning the ankle, such as running or jumping
How do you treat a lateral ankle injury?
Primary Treatment option are the use of the RICE protocol, which stands for Rest, Ice, Compression, and Elevation, is to reduce pain and swelling within the first 48 to 72 hours after an acute lateral ligament damage. The patient can be provided elbow crutches and told to avoid weight bearing (WB) for 24 hours if it hurts too much.
Do ankle ligaments heal naturally?
The majority of isolated low ankle sprains don’t require surgery. If properly immobilized and rehabbed, even a Grade 3 total ligament tear will recover without surgical procedures.
Is walking good for ligament injury?
Yes. If there is no additional injury to your knee and the pain and swelling go down, you might be able to walk straight lines, climb stairs, and even jog straight lines. A crucial ligament that gives the knee stability is the ACL (anterior cruciate ligament). You can walk with Knee Brace if ligament injury in the Knee or Ankle strap if injury in the Ankle during walking.
Can we walk with ligament tear in ankle?
The remaining ligaments and supporting structures allow you to walk with a torn ligament most of the time, but you may have significant discomfort, a sense of weakness, and instability while walking. However we recommend to use Ankle Strap that stabilize the Ankle and reduce the risk of re-injury. With a complete tear, an Aircast boot can be worn while walking.


2 Comments