Students’ elbow and Physiotherapy management
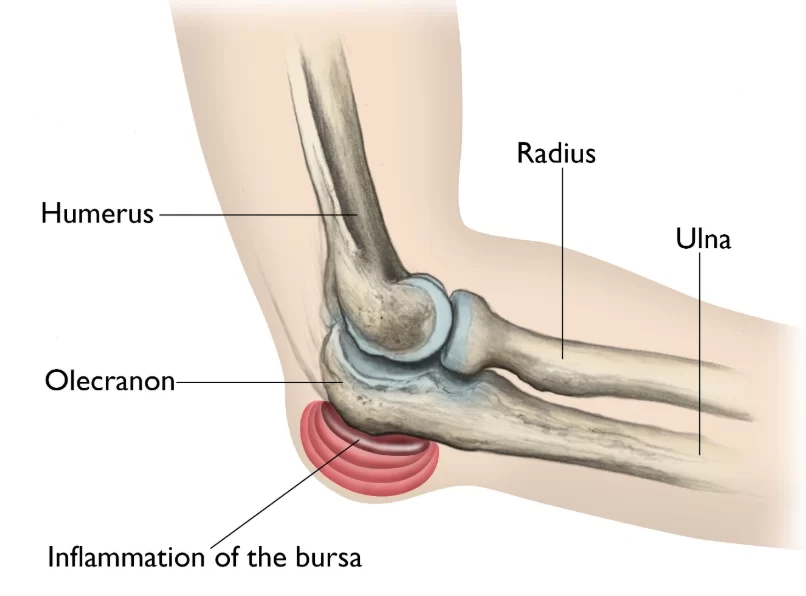
- Baker’s elbow also known as Student’s elbow – is clinically referred to as Olecranon Bursitis. This condition is characterized by pain, redness, and swelling around the olecranon, caused by inflammation of the elbow’s bursa.
- Bursitis normally develops as a result either of a single injury to the elbow (e.g., a hard blow to the tip of the elbow), or more commonly due to repeated minor injuries and if a person’s job involves a repetitive movement, also the possibility of developing the condition is more common as a person gets older.
- Olecranon bursitis is a condition in which there is an inflammation of the bursa overlying the olecranon process at the proximal aspect of the ulna. The superficial location of the bursa, namely between the ulna and the skin is susceptible to inflammation from a variety of mechanisms, primarily either acute or repetitive trauma. It is also possible that the inflammation is due to infection, called septic bursitis.
Anatomy related to Students’ elbow

- A bursa is a part of your body that allows two other parts to move smoothly together (outside of a joint).
- It’s a sac made of thin, slippery tissue. Bursae occur in the body wherever skin, muscles, or tendons need to slide over bone and are lubricated with a small amount of fluid inside that helps reduce friction from the sliding parts.
- The olecranon bursa is located between the tip, or point, of the elbow (called the olecranon) and the overlying skin. This bursa allows the elbow to bend and straighten freely underneath the skin, but when the bursa gets irritated, the sac fills up with fluid which leads to swelling of the elbow tip.
Causes of Students’ elbow
- There is no predisposition for race or sex. Olecranon bursitis occurs with children and adults. Long-term hemodialysis treatment, uremia, or a mechanical factor (like resting the posterior elbow during a hemodialysis treatment) can be a cause of inflammation.
- This condition can be caused by acute injuries (trauma) during sports activities because they can include any action that involves direct trauma to the posterior elbow. For example, falling onto a hard floor, etc.
- Other common causes of olecranon bursitis, which are not related to sports activities, include repetitive microtrauma, like rubbing constantly the elbow against a table during writing.
- Such a trauma or those repeated small injuries lead to bleeding into the bursa or the release of inflammatory mediators.
- People in certain occupations are especially vulnerable, particularly plumbers or heating and air conditioning technicians who have to crawl on their knees in tight spaces and lean on their elbows. Finally, inflammation may be due to a systematic inflammatory process, like rheumatoid arthritis, or a crystal deposition disease, like gout and pseudogout. This condition can also be a side-effect of sunitinib, which is used to treat patients with renal cell carcinoma.
Symptoms of Students’ elbow
- Patients usually remark a focal swelling at the posterior elbow. the swelling is sometimes painless.
- Pressure, like leaning on the elbow or rubbing against a table while writing with the ipsilateral hand, are factors that can often exacerbate the pain.
- Chronic recurrent swelling is usually not tender.
- A typical symptom of olecranon bursitis is the frequent bumping of the swollen elbow because it protrudes further than it usually would.
Clinical presentation of Students’ Elbow
- Bursal inflammation’s most classic finding is a swelling, at the posterior elbow. This swelling is clearly marked off by its appearance as a goose egg over the olecranon process.
- There may be tenderness for palpation at the affected site. Cases in which infection is present may show a warm and red affected area.
- If the trauma has recently occurred, the inspection of the skin may reveal abrasion or contusion.
- Generally, a patient with an advanced infection can have a fever.
- The Range of motion (ROM) of the affected elbow is usually normal but now and then it is possible that the end range of elbow flexion is slightly limited due to pain.
- Patients suffering from systematic inflammatory processes (like rheumatoid arthritis) or crystal – deposition disease (like gout or pseudogout) may reveal evidence of focal inflammation at other sites. When you examine a patient who has rheumatoid arthritis, it is possible that you can see rheumatoid nodules during an inspection of the elbow.
- If the patient reports elbow pain during active or passive ROM and if a history of trauma exists, this may increase the clinical suspicion of an olecranon process fracture.
Diagnosis of Students’ elbow
- Laboratory tests are essential to differentiate septic from non-septic bursitis when doubt remains after clinical examination, so the aspirate should be sent for microscopy and culture.
- Blood tests are not usually helpful. If there is any doubt about the diagnosis then treatment should be given as for a septic case until culture results are available.
Treatment of Students’ elbow
NON-SURGICAL TREATMENT
- Step 1 involves the aspiration of the bursa with an 18-gauge needle. In step 2, a mixture of 80-mg methylprednisolone and 2% lidocaine (specifically 1 mL of methylprednisolone and 1.5 mL of lidocaine without adrenaline) is injected into the elbow joint from a lateral approach. Step 3 involves the application of a dry gauze dressing, followed by the application of a tensor bandage or elbow brace for a period of 3 to 6 months.
- The technique was discovered over 3 to 4 years, with 4 or 5 cases being treated per month. Follow-up with each patient occurred at 2 weeks, 3 months, and 6 months. At each follow-up visit, side effects, pain assessment, and limitation of function (including warmth, degree of swelling, and tenderness) were assessed and recorded.
- The typical pain, skin atrophy, and corticosteroid-induced side effects mentioned by some authors 1–5 were not observed in any of these cases. In addition, none of my patients who used this technique developed septic bursitis or tendon rupture.
Other treatments that have been suggested in the past for nonseptic olecranon bursitis include the following:
- Bursal aspiration alone, with or without compressive dressings;
- Conservative approach:
- Nonsteroidal anti-inflammatory drugs for 10 to 14 days;
- Corticosteroid injections alone, after aspiration;
- A “blood patch” injection;
- The temporary 3-day use of a percutaneous-intrabursal drainage catheter;
- Holding a needle in place with a hemostat, if aspirating and injecting;
- Intrabursal injections of tetracycline and talcum powder. However, from my clinical experience, these treatments are not as effective as the 3-step technique I have described above.
Surgical treatment of Students’ elbow
- Surgery for Infected Bursa
- If the bursa is infected and it does not improve with antibiotics or by removing fluid from the elbow, surgery to remove the entire bursa may be needed.
- This is often an inpatient procedure, meaning you will need to stay overnight in the hospital. This surgery may be combined with further use of oral or intravenous antibiotics.
- The bursa usually grows back as a non-inflamed, normally functioning bursa over a period of several months.
Surgery for Non-Infected Bursa
- If elbow bursitis is not a result of infection, surgery may still be needed if nonsurgical treatments do not work. In this case, surgery to remove the bursa is usually performed as an outpatient procedure. The surgery does not disturb any muscle, ligament, or joint structures.
- Although formal physical therapy after surgery is not usually needed, there are specific exercises to improve your range of motion. These are typically permitted within a few days of the surgery.
Physiotherapy management of Students’ elbow
- Most of the time physical and occupational therapy is not necessary but is often indicated to reduce recovery time. Patients who have often olecranon bursitis are recommended to apply the RICE method of treatment. Rice stands for Rest, Ice, Compression, and Elevation. There are also other physical therapy modalities that could be helpful for reducing pain and inflammation.

- PHONOPHORESIS: Phonophoresis is the use of ultrasound to enhance the delivery of topically applied drugs. Phonophoresis has been used in an effort to enhance the absorption of topically applied analgesics and anti-inflammatory agents through the therapeutic application of ultrasound.,
- ELECTRICAL STIMULATION: Electrical stimulation or neuromuscular electrical stimulation (NMES) is a technique used to elicit a muscle contraction using electrical impulses. Electrodes, controlled by a unit, are placed on the skin over a predetermined area.
- The electrical current is then sent from the unit to the electrodes and delivered into the muscle causing a contraction. Decrease pain, Muscle re-education, and Strengthening Increase range of motion Increase circulation Decrease spasticity, Reduce edema, Decrease inflammation, Improve overall function.
- However, most patients with olecranon bursitis don’t necessarily need those modalities. The physical therapist can also take care of the patient’s education and present compensatory strategies for resting the involved upper extremity while healing takes place.
- When the patient shows no response to conservative treatment and his condition deteriorates, then surgery may be indicated. When a patient undergoes a bursal excision (bursectomy), there might be a recommendation for physical therapy after the operation to regain or maintain the ROM and strength of the elbow.
FAQs
What is a student’s elbow called?
Olecranon bursitis, frequently referred to as “student’s elbow,” can develop in people who lay their elbow on a hard surface for an extended period of time, such as when using a computer keyboard.
Why is it called students elbow?
A bursa may become inflamed and uncomfortable as a result of bleeding into it or inflammation. Medically speaking, it is referred to as olecranon bursitis, although it is also referred to as a student’s elbow. This is due to the possibility that continually leaning on your elbows while studying could create this injury.
How do you get rid of student’s elbow?
Use of Ice Pack and Hot Pacl to relieve Pain.
To lessen swelling and inflammation, a doctor may give anti-inflammatory drugs (such ibuprofen, naproxen, diclofenac, etc.).
If a lot of fluid accumulates, a medical expert can aspirate the fluid by using a sterile needle and syringe.
How long does student’s elbow last?
With rest and other proper Medical and Physiotherapy treatments, elbow bursitis often gets well in three to six weeks. If you have an infection, taking your antibiotics should make you feel better right away.
Is students elbow painful?
A swelling on the end of your elbow that may be painful or (often) not. Leaning on your elbow causes pain.