
Congenital Dislocation of Hip
What is Congenital Dislocation of the Hip(CDH)?
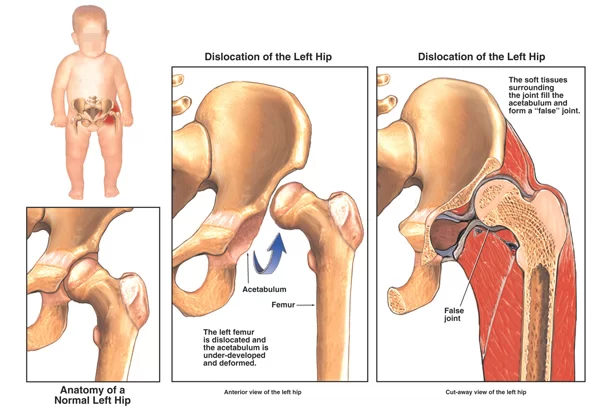
Congenital dislocation of the hip, also known as developmental dysplasia of the hip (DDH), is a condition where the hip joint is improperly formed or dislocated at birth.
It occurs when a child is born with a dislocated hip (unstable hip). It is caused by abnormal development of the hip joint during the early stages of fetal development. It is also called “developmental dysplasia of the hip.” This instability increases as your child grows.
The Hip joint is a ball-and-socket type where the head of the femur pops out of its socket (acetabulum) during hip movement. As per American Family Physician records, 1 child is born with CHD in every 1000 infants.
Introduction:
Developmental dysplasia of the hip (DDH) is a hip problem in a baby born with a dislocated Hip or Dislocation of the Hip that occurs in the first year of life. In a normal hip, the thighbone fits tightly into a cup-shaped socket in the pelvis, and it is held in place by muscles, tendons, and ligaments.
The cause of CHD is unknown in many cases. Contributing factors include low levels of amniotic fluid in the womb, breech presentation, which occurs when your baby is born hips first, and a family history of the condition. Confinement in the uterus may also cause CHD or contribute to it. This is why your baby is more likely to have this condition if you’re pregnant for the first time. Your uterus hasn’t been previously stretched.
Symptoms of Developmental Dysplasia of the Hip:
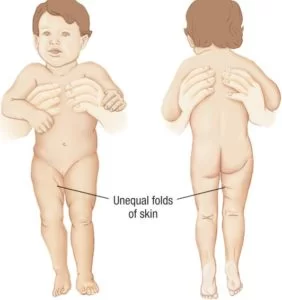
Signs and symptoms in infants, you might notice that one leg is longer than the other. Once a child begins walking, a limp may develop. During diaper changes, one hip may be less flexible than the other. Some children may not see any visible symptoms.
The few most common symptoms are:
- legs are rotated outside
- Legs length are unequal
- reduced range of motion
- uneven skin folds on their legs when their legs extend
- Limping gait or toe walking or waddling gait
- delayed motor function development, which you can see how your child sits, crawls, and walks
How is a Congenital Hip Dislocation Diagnosed?
CHD diagnosis is mostly a physical examination of the Hip joint. Your child’s doctor will perform a few examination tests of the Hip and legs and if clicking or clunking sounds appear that may indicate a dislocation of the Hip. This exam has two tests:
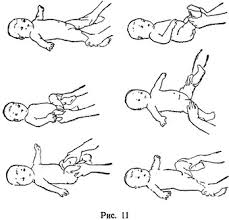
Ortolani test: The doctor will apply upward force while they also move your child’s hip away from the body. Doctors’ thumbs are against the inside of the knees & thighs & the fingers are placed along the outside of the thighs. With gentle traction, the thighs are abducted & pressure is applied against the greater trochanter of the femur.
The Doctor may feel a click, clunk, or jerk, which indicates a positive test & that the hip has reduced.
Barlow test: Each hip is examined individually while the Doctor’s other hand steadies the opposite femur & the pelvis.
The Doctor’s middle finger of each hand is placed over the greater trochanter,& the thumb is placed adjacent to the inner side of the knee & thigh opposite the lesser trochanter.
The hip is taken into abduction while the examiner’s middle finger applies forward pressure behind the greater trochanter.
If the femoral head slips forward into the acetabulum with a click, clunk, or jerk, the test is positive.
It indicates that the hip was dislocated.
Treatment of CDH
Treatment for congenital dislocation of the hip varies depending on the severity of the condition and the age of the patient.
Nonsurgical Treatment
Treatment methods depend on a child’s age.
Newborn The baby is placed in a soft positioning device, called a Pavlik harness, for 1 to 2 months to keep the thighbone in the socket. This special brace is designed to hold the hip in the proper position while allowing free movement of the legs and easy diaper care. The Pavlik harness helps tighten the ligaments around the hip joint and promotes normal hip socket formation.

Parents play an essential role in ensuring the harness is effective. Your doctor and healthcare team will teach you how to safely perform daily care tasks, such as diapering, bathing, feeding, and dressing.
Newborns are placed in a Pavlik harness for 1 to 2 months to treat DDH.
1 month to 6 months. Similar to newborn treatment, a baby’s thighbone is repositioned in the socket using a harness or similar device. This method is usually successful, even with hips that are initially dislocated.
How long the baby will require the harness varies. It is usually worn full-time for at least 6 weeks, and then part-time for an additional 6 weeks.
If the hip will not stay in position using a harness, your doctor may try an abduction brace made of firmer material that will keep your baby’s legs in position.
In some cases, a closed reduction procedure is required. Your doctor will gently move your baby’s thighbone into the proper position, and then apply a body cast (spica cast) to hold the bones in place. This procedure is done while the baby is under anesthesia.
Caring for a baby in a spica cast requires specific instruction. Your doctor and healthcare team will teach you how to perform daily activities, maintain the cast, and identify any problems.
6 months to 2 years. Older babies are also treated with closed reduction and spica casting. In most cases, skin traction is used for a few weeks prior to repositioning the thighbone. Skin traction prepares the soft tissues around the hip for the change in bone positioning. It may be done at home or in the hospital.
However, patients with hip dysplasia may also be advised to visit a physiotherapist before undergoing surgery. A therapist can prescribe exercises that should make the surgery and rehabilitation process more tolerable.
The stronger the joint and surrounding area are before the surgery the easier the rehab should be done.
Surgical Treatment
For 6 months to 2 years old Child
Open surgery is required if the thighbone cannot be properly realigned using a closed reduction operation. During this treatment, the baby’s hip is cut open, giving the surgeon a clean view of the soft tissues and bones.
To fit the bone into the socket correctly, the thighbone may occasionally need to be shortened. During the procedure, X-rays are taken to verify that the bones are positioned correctly. The kid is then kept in the correct hip position by wearing a spica cast.
Older than 2 year Child
In certain kids, the looseness gets worse as they get bigger and more active. In most cases, open surgery is required to straighten the hip. Typically, a spica cast is used to keep the hip in its socket.
Hip replacement:
A hip replacement procedure may be considered in circumstances that are really severe or when all other treatments have failed. Adults with long-standing, untreated hip dysplasia usually undergo this procedure.
Recovery
A cast or brace is often necessary to retain the hip bone in the joint as the kid heals from DDH. You might require the cast for two to three months. During this time, your child’s physician may decide to replace the cast.
Following DDH treatment, X-rays and other routine follow-up monitoring are required until the child’s growth is finished.
PHYSIOTHERAPY EXERCISE
Post-surgical-
Patients require skilled therapy once the hip joint has been corrected through surgery.
The first stage is known as gait training where patients are taught how to use a walker and/or crutches.
After approximately six to eight weeks the muscles will have reattached and the bone will be healed. The condition will then need to be treated by a physiotherapist with procedures such as heat, ice, massage therapy, ultrasound, and possibly traction.
Light strengthening exercises will be prescribed to help mobilize your hip and regain its range of motion. At this stage, it’s important for the therapist to identify any weak muscles and work on them.
This is also an ideal time for patients to get used to using a walker or crutches and for the therapist to let them know what exactly they’ll be facing in the weeks after the procedure.
The traditional physical therapy includes ball catching, ball bouncing, target throwing, kicking, balance beam activities, gait, and stairs, unleveled terrain, running and jumping as well as sensory integration activities including swiss ball, vestibular swing tasks, and scooter board.
Complications
- Children who have spica casting treatment may experience a delay in walking. On the other hand, normal walking development occurs when the cast is taken off.
- There may still be a discrepancy in leg length and skin discomfort around the straps from the Pavlik harness and other positioning devices. In rare cases, location in the Pavlik may also result in loss of motion due to nerve compression in the leg. When the harness is taken off or modified, the nerve nearly always heals.
- Although they are uncommon, growth abnormalities of the upper thighbone can happen when there is an interruption in the blood flow to the thighbone’s growth region.
- A shallow hip socket may continue even after appropriate treatment, and early childhood surgery may be required to restore the hip joint’s normal anatomy.
How to prevent Congenital Hip Dislocation?
CHD cannot be prevented. It is crucial to take your child to checkups on a regular basis so that the physician can diagnose and treat the illness as soon as possible. Before you depart the hospital after delivery, you might want to be sure their doctor checked your baby for indications of a dislocated hip.
Conclusion
If your baby’s CHD is treated with a Pavlik harness and your doctor detects it at an early stage, you may not need as much complex or invasive therapy. Depending on how severe the illness is, it is predicted that between 80 and 95 percent of cases that are discovered early on get a successful outcome.
The success rates of various surgical procedures differ. While some instances only require one operation, others need numerous procedures and years of follow-up care. Untreated congenital heart disease (CHD) in early childhood can lead to early-onset arthritis and severe pain in later life, potentially requiring total hip replacement surgery.
Following a successful course of treatment for their CHD, your kid will probably continue to see an orthopedic specialist on a regular basis to ensure that their hip is growing normally and that the disease doesn’t recur.
FAQs
What is congenital dislocation of the hip?
A total or partial displacement of the femoral head out of the acetabulum is known as congenital acetabular dysplasia, which results in hip dislocation or subluxation. Age-related physical indicators are necessary for diagnosis. The most sensitive tests are those for instability in newborns.
What are the different types of congenital hip dislocation?
The five types that we recognize are as follows:
1. lateralized acetabulum
2. False acetabulum
3. capacious acetabulum
4. maldirected acetabulum
5. femoral deformity
When the acetabulum keeps facing laterally and forward, it is considered maldirected.
What are the long-term effects of congenital dislocation of the hip?
If therapy is delayed, the child may experience limited hip abduction, limping, and leg length disparity. In fact, DDH is the most prevalent cause of early osteoarthritis in women under 40. The objective should be to detect and screen for DDH before the child reaches six months of age in order to avoid long-term issues.
What is the special test for congenital hip dislocation?
Ortolani’s Test
Utilized for hip dislocation confirmation. After flexing the knees and hips to a 90-degree angle, gently adduct the leg with your thumbs while applying anterior pressure over the greater trochanter. There will be a noticeable clunk as the hip moves if it was dislocated. Ortalani’s test would be positive for this.


2 Comments