
Costotransverse syndrome and Physiotherapy management :
Definition of Costotransverse syndrome :
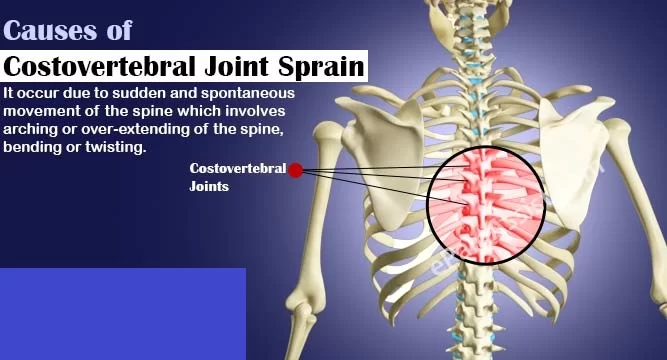
Costotransverse disorders are disorders affecting or involving the costotransverse and costovertebral joints and ligaments which are often overlooked during examination for pain source localization in this area due to possible visceral pain referral and the complexities of the thoracic neural network.
The joints between the vertebrae in the upper back and the ribs are called the costovertebral joints. A joint disorder refers to an injury affecting one of these joints. Physiotherapy is an excellent treatment for costovertebral joint disorders.
It is suggested that dysfunctions in these joints could account for pain in the thorax or functional impairments.
Clinically Relevant Anatomy
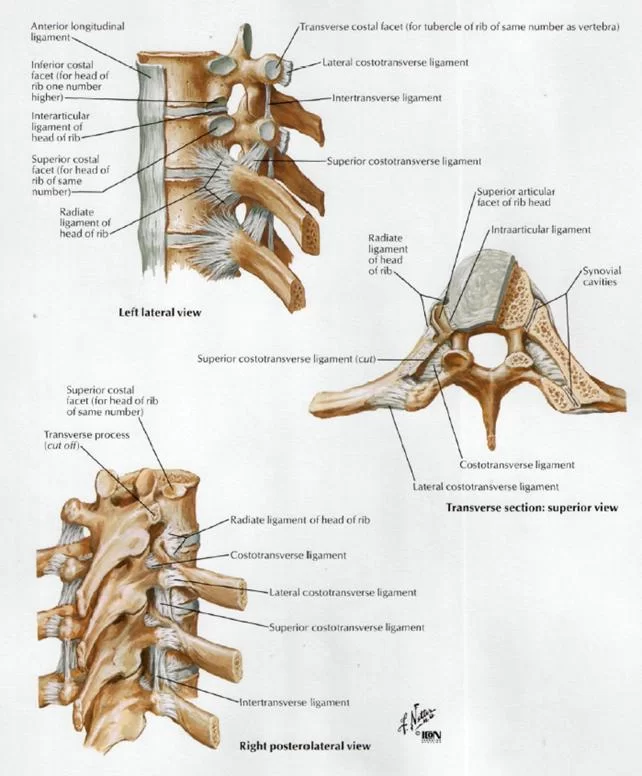
- The costotransverse joint is an articulation between the articular costal tubercle of the rib and the costal facet of the transverse process of a thoracic vertebra.
- The costovertebral joint is the articulation between the costal facte or demi-facets (formed by the caudal side of the superior vertebra and the cranial side of the inferior vertebra) and the head of the rib These facets form a solid angle whose base consists of the annulus fibrosis of the intervertebral disc.
- A synovial joint ensures the connection between the rib and the thoracic vertebra. Together with the thoracic cage, the costovertebral and costotransverse joints provide stability.
The following costotransverse and costovertebral ligaments connect the two joints
- ligamentum costotransversarium superius
- ligamentum costotransversarium.
- ligamentum costotransversarium laterale
- ligamentum capitis costae radiatum
- inferior costotransverse ligaments
- posterior costotransverse ligaments, identified on the fifth to tenth ribs
- These ligaments limit movement in the costotransverse joint to a minimal gliding movement.
- The ribs articulate posteriorly twice with the corresponding vertebra. The radiate ligament and the intra-articular ligament stabilise the head of ribs 2 to 9 and sometimes the head of the 10th rib in the costovertebral joint.
- The head of ribs 2 to 9 and sometimes the 10th articulate with the vertebral body of two thoracic vertebrae in the costovertebral joint. The head of ribs 1, 11 and 12 articulate with the corresponding vertebrae.
- There is no intra-articular ligament in these joints. The neck of ribs 1 to 10 articulate, through the tubercle, with the transverse process of their corresponding vertebrae and are stabilized with ligaments and the articular capsule. Ribs 11 and 12 do not articulate with the transverse processes.
- Lateral flexion as well as rotation is limited by the ribcage therefore only small movements are possible in the costotransverse joints. There is no sagittal plane flexion and extension in these joints, however gliding movements within the joint have been seen.
- These gliding movements are mostly medially and laterally orientated. The medial and lateral glides are functional motions.
Movement of the ribs at the costovertebral joints. The axes of the ribs allow three basic types of motion:
- Bucket handle motion: One end of the rib is fixed at the vertebral end, the majority of the rib elevation occurs through an upward excursion of the lateral position. This motion increases the transverse diameter of the rib cage.
- Pump handle motion: One end is fixed, and the free end describes an arc. When the ribs move around the axis, the anterioposterior diameter of the rib cage increases.
- Caliper motion: The 11th and 12th ribs have only costovertebral articulations. The motion produces slight changes in both the transverse and the anteroposterior dimensions.
- All twelve ribs have pump handle and bucket handle movements, but the upper ribs have a greater pump handle motion and the lower ones have more bucket handle type movements.
Cause of Costotransverse syndrome :
- Local joint compression may occur as a result of a trauma or muscle spasm
- It is more common in women and can occur at any age
- When subjected to severe trauma, these joints can subluxate or dislocate. Due to being at the top of the rib cage, the first costotransverse joint is the most vulnerable.
- Though distinctly unusual at the costotransverse and costovertebral joints, rheumatoid arthritis can occur in these joints.
- The involvement of dysfunction at these joints is a source of referred pain at the thoracic spine, with suggested involvement of the costotransverse joint concerning T4 syndrome
- The costotransverse joint is known to be involved in patients with ankylosing spondylitis, which, combined with the involvement of the costovertebral, sternoclavicular, and sternomanubrial joints, would result in increased rigidity of the thorax and increased dorsal kyphosis. This does not result in decreased pulmonary function, which is possibly due to an increase in diaphragmatic breathing
- Due to the positive response to manual therapy directed towards posterior spinal structures, conditions diagnosed as costochondritis might actually be caused by neurogenic inflammation.
- Characteristics/Clinical Presentation
Possible symptoms are:
- Pain localized to the posterior thorax
- Pain may radiate to the anterior chest wall, along the rib, sometimes into the shoulder and sometimes towards the upper limb
- Unilateral symptoms
- Pain with deep inspiration, coughing/sneezing/laughing
- Increased pain with passive or active thoracolumbar flexion, rotation and ipsilateral side bending, lifting or twisting movements
- Hypomobility of the costotransverse and costovertebral joint
- Palpable tenderness and pain at costotransverse joint and rib angle
- Movement in adjacent thoracic vertebral and rib segments is usually restricted and may stimulate or exacerbate protective muscle spasm
- Increased muscle tension in paraspinal muscles, rhomboid muscles, trapezius muscles, and levator scapula muscles
- Neck pain, headache or both
- The sensation of having a useless or heavy limb
- Referred pain originating from under the scapula and worsens with coughing, sneezing or deep breathing
- Acute, atypical chest pain
Differential Diagnosis
- Differential diagnostic possibilities have to be taken into consideration in cases of posterior upper thoracic and/or scapular pain and possible involvement of costovertebral and costotransverse joints. Possible musculoskeletal sources of thoracic pain are:
- Muscle strain (erector spinae, lower and middle trapezius, rhomboideus, latissimus dorsi, levator scapulae, and intercostal muscles)
- Vertebral or rib fracture
- Zygapophyseal joint arthropathy
- Active trigger points
- Spinal stenosis
- Intervertebral disc protrusion or herniation
- Diffuse idiopathic skeletal hyperostosis (DISH)
- Intercostal neuralgia: > often follows injury or thoracic surgery
Examination
The physical examination consists of the following components:
- Inspection of the posterior, lateral and anterior sides of the trunk, to check for deviations from an ideal posture (standing)
- Active range of motion of the cervical (seated), trunk (standing), and shoulder regions (seated) to determine pain-provoking movements
- Manual muscle testing to assess upper extremities strength and intensity of possible elicited pain (seated)
- Sensory examination of the upper extremities and thoracic area, in order to determine whether nerve root or peripheral nerve lesions are present
- Accessory motion or joint movement of the thoracic spine (in prone position) to check for pain and mobility using the posterioranterior (PA) pressure test.
- Posterior (prone) and anterior (supine) costosternal joint movement to assess for pain and mobility
- Active and passive scapular mobility in case of reduced active shoulder range of motion and/or pain of the scapula region
- Palpation of the cervical, upper trunk, and shoulder regions to check for soreness or pain
Medical Management
- In an unstable thoracic spine (caused by trauma, degenerative conditions, tumors, and deformities) posterior instrumentation and fusion are commonly used as treatment.
- Numerous techniques have been reported to restore spinal stability and correct spinal deformities. Posterior fixation of the thoracic spine through the costotransverse joint may be an alternative (figure 2).
- Thanapipatsiri and Chan showed that posterior thoracic fixation through the transverse processes is safe as implants placed beneath the transverse processes are away from the parietal pleura and the intercostal vessels and nerves.
- Heller et al. demonstrated that transverse process screws were weaker biomechanically than pedicle screws in the upper thoracic spine, but safer technically Fixation around the transverse processes in the thoracic spine appears to be simple and safe, but fixation through the costotransverse joint may be more rigid than through the transverse process.
Risks of costotransverse screw fixation:
- Injury of the intercostal neurovascular structures.
- Injury of the parietal pleura.
- Fixation at multiple levels may result in limitation of movement of the thoracic cage and may affect the long function.
Figure 2: posterior costotransverse screw insertion technique.
- Patients with upper back pain, pain between the ribs, and thorax pain may be candidates for a costotransverse or costovertebral joint injection. The injections have two purposes: to confirm the diagnosis that these joints are the source of back pain and secondly, to offer temporary pain relief.
Physiotherapy Management
- Physiotherapy interventions have been shown to be effective at improving the prognosis of back pain in the thoracic region.
Mobilization:

- Mobilisation of the rib is in an anteroposterior direction, using oscillations with contact on the dorsal surface of the rib, adjacent to the thoracic spinal articulation). Rib distraction mobilizations can be an effective initial treatment. This technique is best done with the patient in a sitting or prone position.
- A rib rotational glide is an effective technique and sometimes preferable to the rib distraction technique if direct pressure on the rib is too painful. This technique can be administered while the patient in standing, sitting, or in reclining position
- Maitland suggests that mobilizations are effective for:
- Treatment of stiffness
- Treatment of pain, rather than stiffness.
- 3 repetitions are usually performed, followed by retesting for pain on palpation. Mobilizations are repeated to any rib that was still painful until there is no longer palpable pain.
- Also General spinal mobilizations and Elbow mobilizations
Other manual techniques include:
- Dorsal glides of the thoracic spinal facet joints (via the ribcage).
- Soft tissue techniques: massage (deep friction, friction, and normal), stretching, and trigger point release)
- Massage of the scalene muscles
- LASER therapy of the ribs
- Acupuncture (contra-indications)
- High velocity, low amplitude chiropractic diversified adjustments in an anteroposterior direction with the patient in a supine position
- High-velocity, low-amplitude manipulations directed at the costovertebral, costotransverse, and intervertebral zygapophyseal thoracic joints
- Mobilizations of the costovertebral and costosternal joints: large amplitude P/A oscillations of the ribs in prone position.
- Exercise therapy:
- Chest lifts as a home exercise
- Chest lifts may be a useful generic treatment technique for rib articular dysfunction or thoracic facet joint dysfunction. With the patient in hand and knee position, reach underneath the chest with both hands, lace fingers together, and slowly and gently lift the torso.
- Repeat this manoeuvre a few times, slowly and rhythmically, lifting from different portions of the chest or sternum to create a movement at different segments of the thoracic spine. These techniques should be pain free.
- Underwater treadmill therapy
- Push-ups to activate the pectoral musculature (after the 6th visit). 5 to 10 repetitions, 3 sets
- Wall push-ups (after the 7th visit), progressively build up to full push-ups. 5 to 10 repetitions, 3 sets
- Rotation exercises while seated: sitting tall, back and neck straight, and your arms across your chest. Keep the legs still and rotate to one side as far as able without pain, hold for 3 seconds and repeat 10-15 times to each side, alternating sides
- Shoulder retraction: This exercise should first be performed while seated. In a later phase, a standing position can be adopted. Retract the shoulders as far as comfortably possible, without pain, and hold for 3 seconds, repeating 10-15 times
- Scapular stabilisation and postural re-education
Self-mobilization techniques:
- Tape two tennis balls together to create an ellipse shaped ball.
- Thoracic spine mini-crunches.
- Place the balls on the segmental level below the on to be mobilised.
- Lying on the balls and arms are crossed over the chest, which protracts the scapula, allowing the balls to make contact with the spine
- Slowly lift the shoulders off the floor. Hold this position for 3 seconds.
- Do 2-3 sets of 15-20 repetitions
Supine arm circles
- Place the balls at the point of discomfort
- Lie down on the balls. Bring the shoulders to 90 degrees abduction. Draw circles with the wrist in a clockwise and then counterclockwise motion.
- 2-3 sets of 30 to 60 seconds in both directions




2 Comments