Dolichocyphaly
Introduction
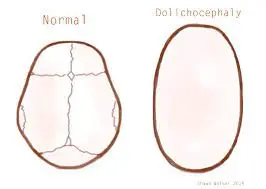
Dolichocyphaly is a term used in craniofacial morphology and anthropology to describe a specific skull shape characterized by elongation of the cranial vault. This condition results in an abnormally long and narrow head, often associated with changes in the shape of the cranial sutures.
It’s not uncommon for newborns to exhibit slight cranial deformities immediately after birth and during the early weeks of life. This is entirely natural because infants’ skulls are designed to be pliable, adapting to the numerous changes that occur during gestation, the birthing process, and the initial year of their lives. Typically, these deformities are minimal and tend to resolve on their own.
However, what should you do if your baby’s head appears significantly misshapen? Is this a cause for concern? If your baby’s skull exhibits an elongated appearance, it might be indicative of a condition known as dolichocephaly, also referred to as scaphocephaly. If you find yourself in this situation, you likely have numerous questions regarding this condition, its implications for your baby, and the available treatment options.
What is Dolichocephaly?
Positional skull deformities can arise when a baby remains in the same position for extended periods. Depending on their posture, this prolonged immobility can lead to changes in the shape of their head.
Dolichocephaly specifically pertains to the elongation of an infant’s head, typically resulting from post-birth positioning. It is frequently, though not exclusively, associated with prolonged stays in neonatal intensive care units (NICUs).
Infant skulls consist of multiple soft plates that are not fully fused at birth. This inherent flexibility facilitates the passage through the birth canal and accommodates the rapid brain growth that occurs within the first 12 months of a baby’s life.
According to the American Academy of Pediatrics (AAP), misshapen heads and skull deformities are observed in approximately 20% of childbirth cases or due to the baby’s positioning in the womb. However, most often, these deformities manifest after birth during the initial 4 to 12 weeks when babies spend a significant amount of time lying flat and have limited mobility.
Understanding ‘breech head’ molding
This post delves into the intricacies of dolichocephaly, a type of positional molding that can impact certain breech babies. We’ll explore how it occurs, why it holds significance, and how to identify it.
Concerns often arise about the potential entrapment of the aftercoming head during a breech birth, and it can indeed seem unpredictable. Interestingly, many breech babies, even those on the larger side, appear to effortlessly navigate the birthing process, while others, despite being smaller, encounter difficulties. According to the Royal College of Obstetricians and Gynaecologists (RCOG) guidelines, an estimated fetal weight exceeding 3800 grams is considered ‘unfavorable’ for a vaginal breech birth.
However, the guidelines go on to note that if the baby’s trunk and thighs can pass through the pelvis simultaneously with ease (although ‘easily’ remains undefined), the likelihood of cephalopelvic disproportion is low. In the context of the growing body of evidence against interventions during breech labor, this interpretation suggests that such passage should occur spontaneously within approximately an hour of active pushing.
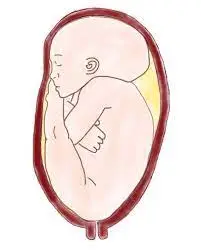
Technically speaking, dolichocephaly represents a mild cranial deformity characterized by the disproportionate elongation and narrowing of the head, resulting from mechanical forces associated with the breech positioning in utero. This alteration in head shape is more commonly linked to primiparity (first-time mothers), larger infants, oligohydramnios, and posterior placenta placement, all of which contribute to increased pressure on the fetal head.
Clinical Significance
Once the arms emerge during a breech birth, the baby’s head aligns within the anterior-posterior diameter of the pelvis. In cases where the head has undergone abnormal elongation, the longest diameter of the fetal head meets the shortest diameter of the maternal pelvis at the inlet. Unless the baby is relatively small and the pelvic inlet is exceptionally round, there’s a risk that the baby’s chin might become lodged on the sacral promontory, hindering head flexion. Even for seasoned breech providers, this situation can be challenging. It may necessitate rotating the head into the transverse diameter for safe entry into the pelvis. A significantly elongated head can also encounter difficulties passing through the lower pelvis and may potentially harm the maternal pelvic floor if not managed with appropriate techniques.
Estimating fetal weight through ultrasound is notoriously unreliable. However, a lack of proportionality between the head circumference and the biparietal diameter is more easily detectable (e.g., HC=90th percentile, BPD=60th percentile) and could be a more relevant indicator that the baby might be too large for the mother to birth comfortably. Dolichocephaly can also be detected through palpation, as the occiput is prominently felt above the fetal back, the head doesn’t move freely and may feel unusually wide. I would recommend caution when the estimated fetal weight exceeds 3500 grams, and there’s a discrepancy between HC and BPD, or when careful palpation indicates abnormal cranial molding, particularly in primiparous women, those with low amniotic fluid levels, and/or a high posterior placenta. In cases where imaging pelvimetry isn’t used to confirm an adequately sized pelvic inlet.
Counseling Women:
Women often resist the use of weight limits as ‘selection criteria.’ They recognize that no two women are alike, and their ability to carry and birth babies varies widely. For instance, Ann, a multiparous woman standing at 6’1″, might carry a 4000-gram baby without experiencing abnormal head molding and expect a straightforward birth. Conversely, Carol, a primiparous woman of shorter stature at 5’0″, might observe signs of dolichocephaly in her 3300-gram baby, particularly if she has low amniotic fluid levels and a posterior placenta. Carol may still achieve a successful birth, but her outcome will depend more on the expertise of her healthcare provider in assisting the aftercoming head to flex, rotate, and navigate the pelvic dimensions, as well as the inherent dimensions of her pelvis.
We must shift our perspective away from rigid ‘selection criteria,’ which professionals use to make decisions for women, and toward a deeper understanding of what constitutes ‘normal’ for breech births. It’s crucial to gain insights into which babies are more likely to experience those graceful, often smoother-than-cephalic, arrivals into the world, and which babies might genuinely face additional risks due to their in-utero conditions.
This shift will enable us to educate women about the advantages of cesarean sections for pregnancies that have deviated from what is considered ‘normal.’ Women will approach this intervention with greater openness when they perceive that professionals are genuinely supportive of ‘normal’ breech births and provide personalized care and screening for cases that deviate from this norm.
What are the Causes of Dolichocephaly?
The origins of dolichocephaly remain somewhat mysterious, as specific risk factors are not well-defined. However, it frequently arises in infants who spend prolonged periods in a fixed position.
Craniosynostosis:
Craniosynostosis, a congenital defect, is one of the primary causes of dolichocephaly. In a baby’s skull, there exist spaces filled with a pliable substance called sutures. These sutures, owing to their flexibility, enable the brain to grow and develop naturally.
Craniosynostosis occurs when the bones of the infant’s skull prematurely fuse together before the brain has had a chance to fully develop. In babies affected by craniosynostosis, the brain’s growth is hindered in the portion of the skull that has fused prematurely, while other areas of the brain continue growing. Consequently, an abnormal skull shape takes form.
Among the various types of craniosynostosis, sagittal synostosis is most closely associated with dolichocephaly. Sagittal synostosis involves the untimely closure of the sagittal suture, which extends from the top of the baby’s head near the fontanelle (soft spot) all the way to the rear of the head. Normally, the sagittal suture begins closing later in life, typically around 21 to 30 years of age.
Prolonged Side or Prone Positioning:
Sometimes colloquially termed “NICUcephaly,” dolichocephaly is observed in certain cases involving premature babies who spend time in the Neonatal Intensive Care Unit (NICU). The U.S. National Library of Medicine explains that most instances of dolichocephaly occur in preterm infants born at less than 32 weeks of gestation. This condition can be attributed to the extended periods during which these babies are placed in side-lying or prone positions, meaning they lie on their stomachs.
These specific positions are employed in the NICU to safeguard the health of premature infants, reducing their risk of issues such as reflux, apnea, and bradycardia. However, unfortunately, they can result in the development of dolichocephaly. While some cases of dolichocephaly may resolve by the time the baby is discharged from the hospital, others persist, leading to babies being discharged with this condition.
Risk Factors of Dolichocyphely
Dolichocephaly can manifest even in an otherwise typically developing skull when a baby spends excessive time in specific positions. Although some research suggests a genetic association with craniosynostosis-related dolichocephaly, the precise underlying causes of this condition remain incompletely understood.
What are the Complications related to Dolichocyphaly?
According to the American Academy of Pediatrics (AAP), the majority of cases involving misshapen infant heads or skull deformities are generally not serious and do not pose any threats to an infant’s health or overall well-being. The AAP notes that “Positional skull deformities do not impact brain growth or intellectual development.” These deformities are primarily cosmetic and typically do not necessitate surgical intervention.
However, severe cases of dolichocephaly can be more complex and may potentially impact a baby’s health and development. As outlined by the U.S. National Library of Medicine, “The long-term consequences of dolichocephaly are not entirely understood, but it has been associated with delayed attainment of motor skills, muscular tightness in the spinal extensors and scapular retractors, and the development of motor imbalances.”
Moreover, a pronounced deformity can affect an individual’s self-esteem and confidence as they progress into adulthood. Surgical correction during infancy can not only enhance the head’s shape but also prevent potential psychological issues stemming from severe cosmetic concerns.
If you have concerns about the possibility of your baby having a severe case of dolichocephaly that might lead to developmental, health, or psychological challenges, it is advisable to consult your pediatrician. They will assess the situation and determine whether additional tests, such as a CAT scan, are necessary to gain a better understanding of how dolichocephaly might impact your baby. If required, your pediatrician will discuss specific interventions and treatments.
What is the Treatment of Dolichocyphaly?
In many instances, mild cases of dolichocephaly and other forms of skull deformities will naturally resolve as your baby grows and develops. However, for moderate or severe skull deformities, various therapies and interventions may become necessary. The decision to pursue these interventions is typically determined on a case-by-case basis in consultation with your healthcare provider.
As per guidance from the American Academy of Pediatrics (AAP), there are three primary interventions for addressing misshapen skulls and positional skull deformities: physical therapy, helmet therapy, and surgery.
Physical Therapy:
Enlisting the assistance of a pediatric physical therapy Treatment can be beneficial as you navigate the challenges posed by dolichocephaly. They can assess your baby for any developmental delays and offer guidance on stretching and positioning exercises that can be performed at home to aid your baby’s progress.
Helmet Therapy:

Some infants with misshapen heads may benefit from the use of a molding helmet. Typically, this is recommended when a baby’s head fails to attain a healthy shape by the age of 5 to 6 months. The fitting and adjustment of these helmets are carried out by specialists.
Surgery:
In more severe cases, surgery may become necessary, especially for significant instances of sagittal craniosynostosis. During surgery, the affected suture is surgically corrected to reshape the baby’s head. Ideally, this surgical procedure is performed during the early months of life to achieve the best possible results.
At-Home Treatments for Dolichocyphaly
In addition to specialized treatments, there are practices you can incorporate at home to support your baby’s skull development. Here are some guidance from the American Academy of Pediatrics (AAP):
- Variety in Positioning: Avoid keeping your baby in a single position for extended periods, especially those that exert pressure on their head. For example, limit prolonged periods in car seats, bouncy chairs, or baby swings.
- Encourage Movement: Facilitate opportunities for your baby to move, with a particular emphasis on tummy time. Babies with skull deformities may benefit from increased tummy time, which allows them to move their neck, head, back, shoulders, hips, and arms naturally. Start gradually and work up to longer tummy time sessions if your baby initially resists.
- Alternate Feeding Positions: When feeding your baby, switch arms periodically to promote balanced head growth.
- Vary Crib Placement: While it is essential to place babies on their backs for sleep, you can alter the position within the crib to facilitate head-shape balance.
Tips to Prevent Head Deformity
When it comes to preventing head deformities, early awareness, and proactive measures can make a significant difference in allowing your baby’s head to develop properly. Here are some valuable tips:
- Limit Time in Carriers: Minimize the duration your baby spends in a carrier, such as a car seat, stroller, baby swing, or bouncy chair. Extended periods in these devices can exert pressure on your baby’s head and potentially lead to misshaping.
- Prioritize Tummy Time: While it’s essential to place your baby on their back for safe sleep (reducing the risk of Sudden Infant Death Syndrome, or SIDS), during their waking hours, incorporate ample tummy time into their routine. Tummy time facilitates the development of muscle tone in your baby’s back, neck, shoulders, hips, and arms. It prepares them for milestones like rolling, sitting up, crawling, and independently changing positions.
- Vary Feeding Positions: Change your baby’s feeding positions regularly. This practice prevents their head from being consistently in the same position, promoting the development of a normal head shape.
- Rotate Sleeping Orientation: When putting your baby down to sleep, alternate the ends of the crib they use. Different ends of the crib offer varying lighting and visual stimuli for your baby. This encourages more diverse head movements and helps alleviate pressure on the same spot of the skull.
By following these tips, you can actively contribute to your baby’s healthy head development and reduce the risk of deformities.
FAQ
Is dolichocephalic normal?
The majority of dolichocephaly cases, according to the AAP, are not significant and have no impact on the infant’s health. There are other examples, though, that are more serious and may be connected to delayed physical abilities like reaching and gripping.
What are the effects of dolichocephaly?
Dolichocephaly is a main feature that sets CED apart from the majority of other ciliopathies. It is frequently subsequent to sagittal craniosynostosis. Delays in development and brain abnormalities are also possible.
What are dolichocephalic head shapes?
Babies are at their least mobile during this stage and are unable to roll over, alter positions, or sit up by themselves. The positional skull deformity in neonates with dolichocephaly (scaphocephaly) is characterized by a head shape that is longer and narrower, comparable to a boat.
When does dolichocephaly resolve?
Although dolichocephaly may go away before hospital discharge, infants are occasionally sent home with the abnormality. Few studies describe the frequency of dolichocephaly in preterm infants despite the fact that it has been documented for almost three decades and the rate at which it resolves with treatment.
Why is my baby’s head elongated?
When a baby is delivered head 1st, the pressure of birth canal can form the head into an oblong shape. The head of a child might alter shape due to these cracks between the skulls. The bones of the skull may precisely overlap depending on the intensity & period of the pressure.
Reference
- Pmp, K. C. M. B. (2022, December 15). What Is Dolichocephaly in Newborns? FamilyEducation. https://www.familyeducation.com/babies/health/what-is-dolichocephaly-in-newborns
- Wisner, W. (2022, May 19). What to Know About Dolichocephaly. Verywell Family. https://www.verywellfamily.com/what-to-know-about-dolichocephaly-5116781