Fibula Fracture
What is Fibula Fracture?
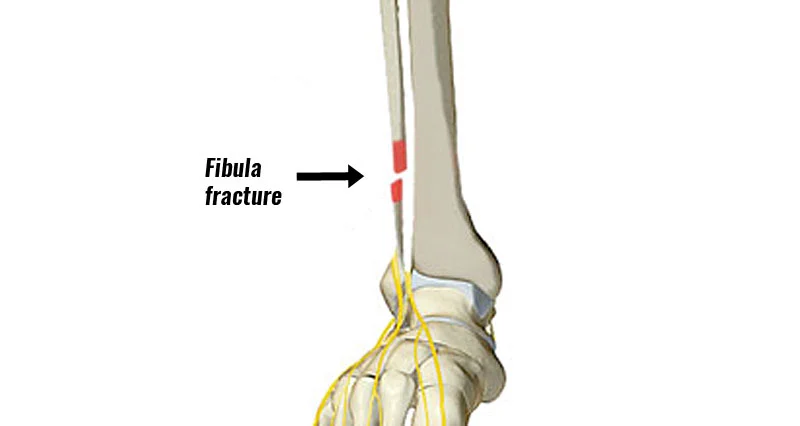
A fibula fracture is a partial or complete break of the fibula bone caused by a forceful impact that results in injury. It can also occur when there’s more tension or stress on the fibula bone than it cannot handle.
What is Fibula?
The fibula is a long, thin bone. It starts just below the knee joint on the lateral side of the leg and lengthens all down to the ankle joint.
Along with the tibia, it is the larger bone of the lower leg and carries most of the body weight. The fibula helps to maintain the ankle joint stable.
A fibula is made up of several parts. These include:
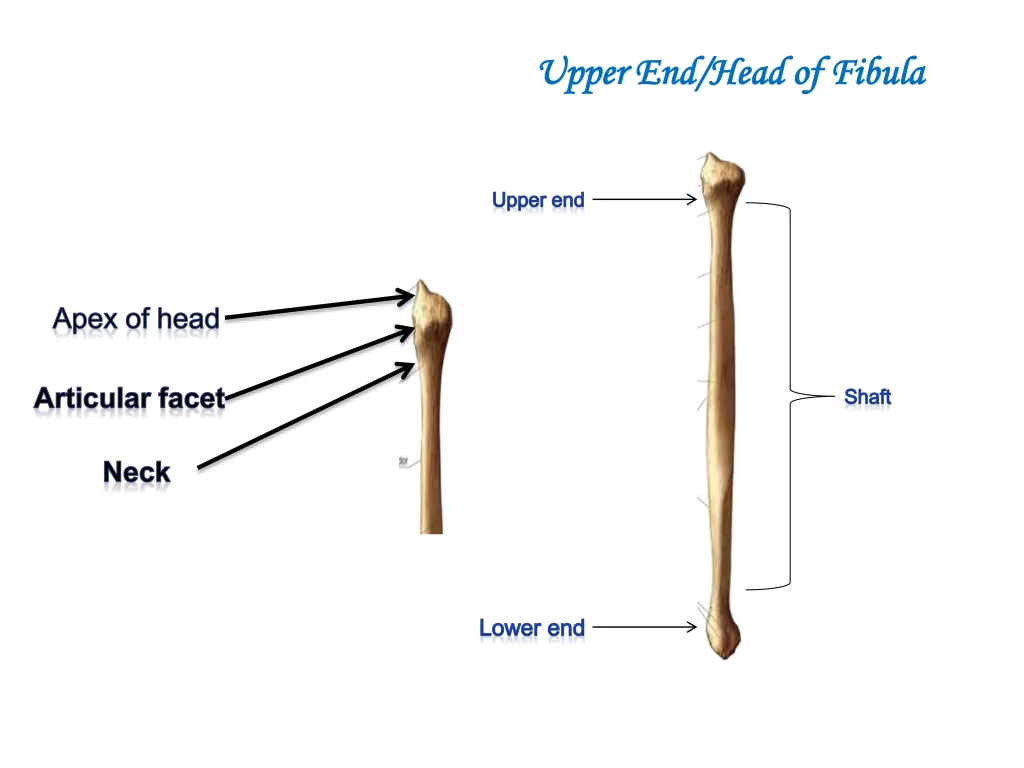
Fibula head (proximal aspect)
The proximal head is an enlarged, irregular part of the fibula.
The styloid process—a small, superiorly pointed tubercle formed from the lateral and posterior aspects is present.
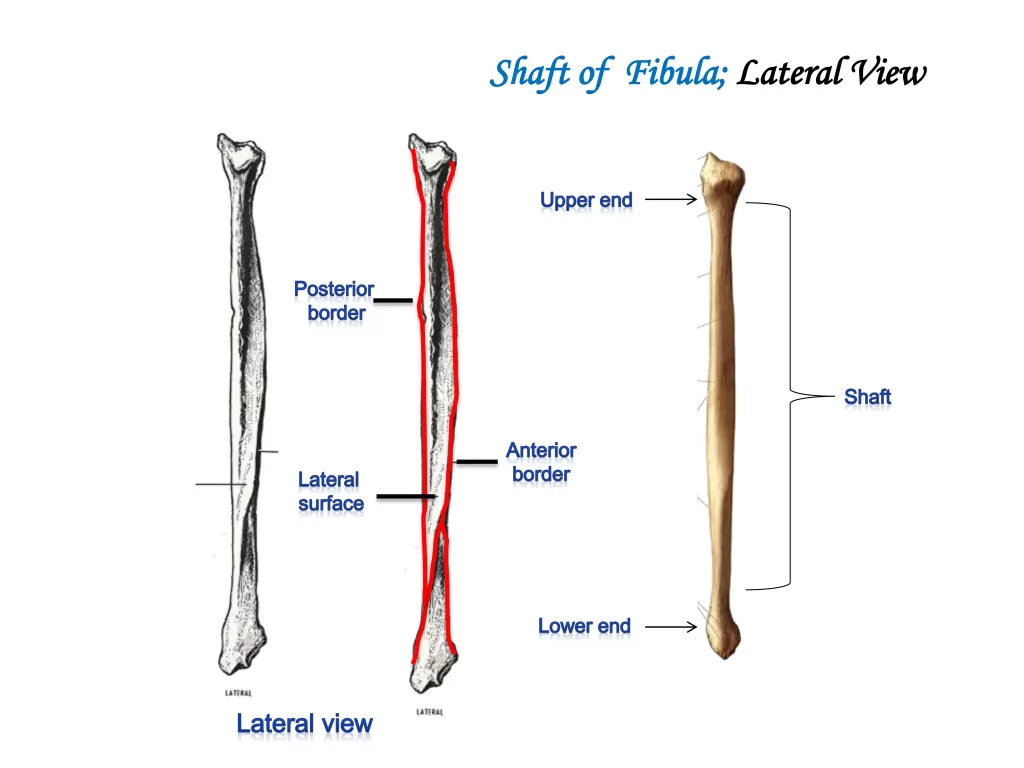
Fibula shaft
The shaft is the long part of the fibula that creates the structure of your calf. It’s shaped like a three-sided prism.
It contains 3 Borders:
- Anterior border
- Posterior border
- interosseous border
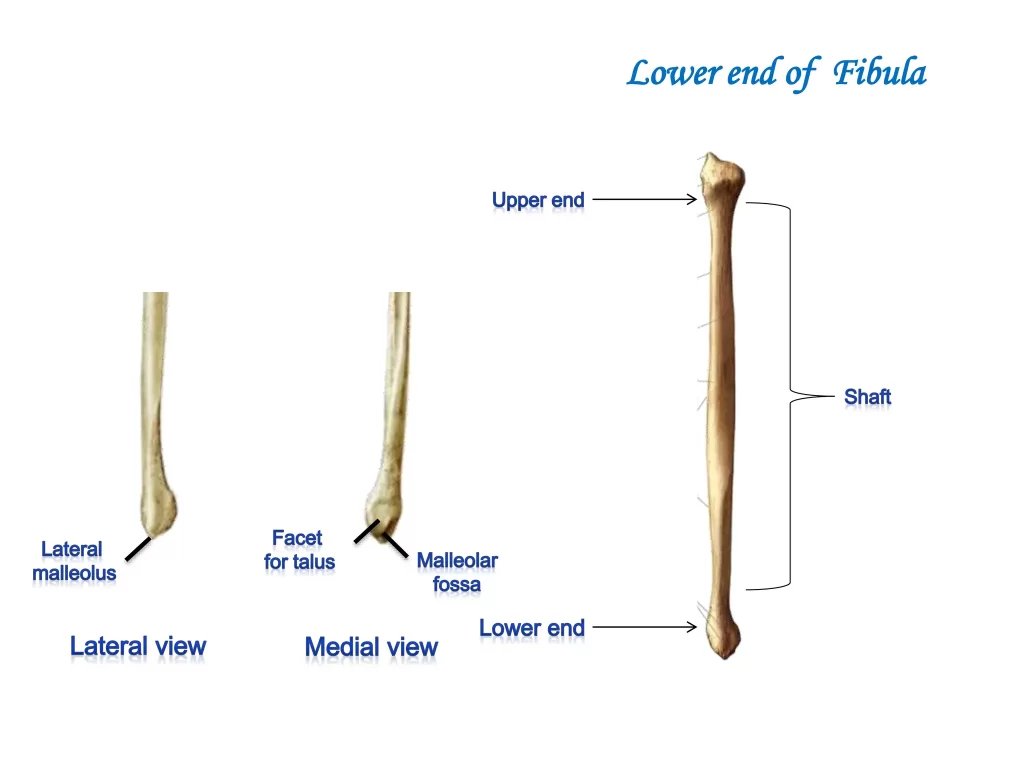
Fibula distal aspect
The lower (distal) end of your fibula creates the top of your ankle joint. It meets the tibia and calcaneus (ankle bone).
Types of Fibular Fractures
- There are different types of fibular fractures.
- Lateral malleolus fractures: These are fibular fractures of the lower end of the fibula that take place at the ankle.
- Fibular head fractures: These are fractures that occur at the knee portion of the fibula bone.
- Avulsion fractures: These fractures occur when a part of the bone is pulled away by the tendon or ligament attached to it.
- Stress fractures: Stress fractures occur due to repeated stress to the bone and are most commonly seen in sports activities such as long-distance running, basketball, tennis, gymnastics, dance, and track and field.
- Fibular shaft fractures: These fractures occurs at a long, narrow part of the fibula bone.
Causes of Fibula Fracture
Fibular fractures are usually caused by:
Low-energy trauma: Simple, ground-level falls most commonly seen in elders or sports injuries that athletes usually experience.
High-energy trauma: It includes motorcycle or automobile accidents. May be patient have a history of direct (motor vehicle crash)trauma or indirect (twisting) trauma.
Symptoms of Fibula Fracture
Fibular fractures can show the following symptoms:
- Pain at the site of the fracture on the body.
- Tenderness, swelling, or bruising.
- Visible signs of deformity
- can not able to bear weight or take any form of pressure on the injured leg.
- Numbness in the foot.
- Bleeding or bruising at the fracture site.
- Pain that gets worse when you move.
- Difficulty in walking.
Diagnosis
The doctor will physically examine your injury and operate tests to understand the type of injury and how serious it is.
Physical examination: Generally it contains examining for signs of deformities, symptoms, feeling the bone and joint surfaces, and testing for muscle weakness, reflexes, and range of motion.
Imaging tests:
X-ray: Your doctor may suggest for X-rays to get a better look at your injury to see if you have a fracture or dislocation.

CT scan, bone scan, or MRI: Your doctor may request a CT scan, bone scan, or MRI to identify fractures not visible on the X-ray and to get more detailed pictures of the interiors of the bone and the soft tissues.
Treatment of Fibula Fracture
- Non-surgical method
- Surgical method
Non-surgical method
depending on the stability and risk level of the fracture the doctor will suggest either, a non-removable cast, or a removable walking cast – depending on the stability and risk level of the fracture.
The doctor will give you precise instructions.
If a removable walking cast is suggested by the doctor, weight-bearing in the removable cast is allowed.
- The doctor may allow you to discontinue crutches as soon as the bone heals and pain subsides.
- Further, To avoid falls, prevent further fracture displacement, and ensure that bone healing will go properly, the doctor may recommend continuing to use crutches.
- Use the removable walking cast for all weight-bearing activities as long as your doctor prescribes.
- It is ok to remove the removable walking cast during sleep, bathing, and icing.
- Apply an Ice pack to the fracture area for 15-20 minutes, three times per day for at least 2-3 weeks.
- Reduce activity level, rest, and elevate the affected limb as much as possible every day – for at least 2-3 weeks – longer, if instructed by the doctor.
If a non-removable cast is suggested, the doctor may or may not allow weight bearing. Also advises the use of crutches to prevent falls, for the other benefit against further fracture displacement, and to confirm that bone healing will proceed properly.
This treatment takes 6-8 weeks for proper healing.
Surgical method
It includes internal or external fixation methods
- Internal fixation
In this procedure metal implants are placed inside the broken bone to maintain the fracture together while it heals. - External fixation
metal screws or pins are placed outside the skin to keep the bones in place and together.
Complications of Fibula Fracture
Many patients will experience stiffness and swelling in the fractured leg for many months, even after the fracture has healed.
Other complications such as:
- malunion
- nonunion
- Infection
- Bleeding
- Damage to blood vessels, tendons, and nerves
- Arthritis
Physiotherapy treatment
Immediately postoperatively, the fractured extremity is positioned in a well-padded splint.
The patient is suggested to be non–weight bearing on the fractured limb and to maintain elevation to the level of the heart.
The splint is taken off two weeks after surgery, and the surgical sites are checked. If wound healing is sufficient, range-of-motion exercises may begin.
The patient is positioned into a removable cast boot. Typically, patients are instructed to be 6 weeks of non-weight bearing is required following surgery; however, the operating surgeons may choose to shorten or extend that period as they see suitable.
At 6 weeks postoperatively, the cast boot is released and weight bearing begins.
Phase 1: 0 to 2 weeks
Hematoma formation (days 1 to 5 after fracture). This stage starts immediately after your fracture and starts the healing process of your broken bone.
Fibrocartilaginous callus construction(days 5 to 11 after fracture). It involves the forming of new bone cells to heal your fracture site.

Immobilized by below-knee plaster splint.
Range of motion exercises like
Toe-curling
Knee ROM
Hip ROM
Modalities like Elevation, Cryotherapy were given.
Patient in the non-weight bearing stage.
Phase 2: 2 to 6 weeks
At this stage if the fracture is stable start weight-bearing with the use of a brace and crutch.
If the fracture is unstable non-weight bearing continues.
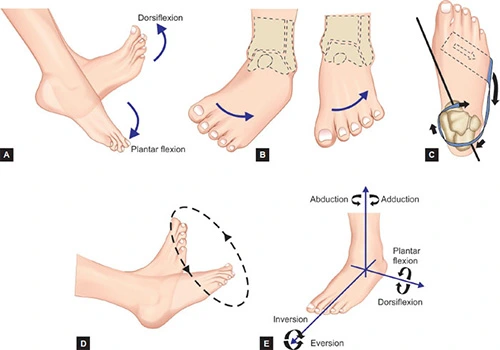
Starts range of motion exercises of the ankle like Dorsiflexion, Planter flexion, Inversion, Eversion, and Rotation.
Strengthening exercises like straight leg raise exercises are performed.
Modalities like cryotherapy are given.
Phase 3: 6 to 12 weeks
At this stage, full weight bearing will be started.
Starts full weight-bearing range of motion exercises.
Strengthening exercises like isotonic strengthening exercises are performed.
Starts proprioceptive training like
Gait training
Single-leg stance
Inversion-eversion boards
Mini-trampoline

Phase 4: after 12 weeks
After 6 months non-athletes can return to their regular activities.
Athletes will also initiate sports-specific exercises, plyometrics, unilateral exercises, and running on the treadmill for cardiovascular recovery.
Perform proprioceptive training like
- Gait training
- Single-leg stance
- Inversion-eversion boards
- Mini-trampoline
- Sport-specific exercises
FAQs
What are the main risk factors for a Fibula Fracture?
Bone mass is the main risk factor for fractures of the fibula in older adults.
Cigarette smoking is another significant risk factor for fibular fractures.
In snowboarding as compared to skiing, fibula fractures are more frequent, and each sport’s fracture pattern is unique. snowboarders are more likely to sustain isolated fractures of the distal third of the fibula whereas skiers typically fracture both the proximal third of the tibia and the fibula.
What are the precautions for a Fibula Fracture?
Ice every 2 to 3 hours. Compression is applied all the time with an ace wrap. Elevate the fractured leg as much as possible, during sitting and sleeping. Swelling can be reduced by compression and elevation after a surgical procedure for healing a fibula bone fracture.
What are the causes of a Fibula Fracture?
Low-energy trauma: Simple, ground-level falls most commonly seen in elders or sports injuries that athletes usually experience.
High-energy trauma: It includes motorcycle or automobile accidents. May be patient have a history of direct (motor vehicle crash)trauma or indirect (twisting) trauma.
How long does it take to recover from surgery for a Fibula Fracture?
It depends upon the type of surgery performed and how severe the injury was. After six weeks, some weight-bearing activities might be possible.
Most movements may take six months or longer to make progress.
What are the complications of Fibula Fracture?
Infection
Bleeding
Damage to blood vessels, tendons, and nerves
Arthritis
Nonunion
Malunion