
Fibularis brevis muscle
What is Fibularis brevis muscle?
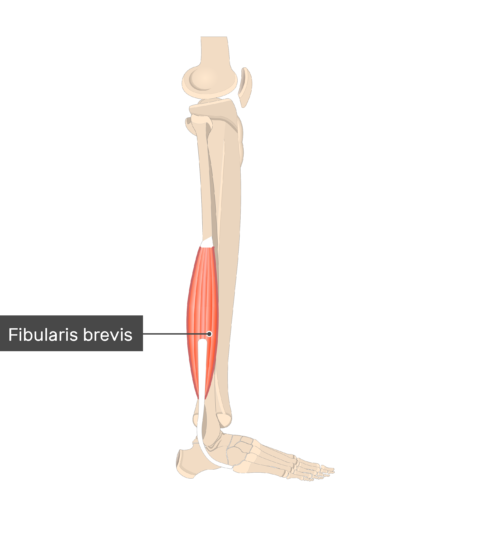
Fibularis brevis muscle, or peroneus brevis muscle, is a short muscle that together with the fibularis (peroneus) longus muscle comprises the group of the lateral leg muscles.
Based on their function, both peroneal muscles belong to a larger group of leg muscles whose primary function is to plantarflex the foot (point the toes downward) at the ankle joint. Various muscles of this group are the soleus, gastrocnemius, tibialis posterior, plantaris muscle, fibularis tertius, flexor digitorum longus, and flexor hallucis longus. But plantarflexing the foot, fibularis brevis, and longus also evert the foot while contracting.
Origin of Fibularis brevis muscle
The Fibularis Brevis muscle arises from the distal two-thirds of the lateral fibula. Its tendon loops posterior to the lateral malleolus and passes downwards.
Insertion
Tuberosity on the fifth metatarsal’s lateral side
Relations
The muscle belly of the fibularis brevis muscle is situated anterior to the flexor hallucis longus, the fibularis longus, and the distal portion of the soleus muscle, and posterior to the extensor digitorum longus and fibularis tertius muscle. The distal section of the sural nerve connects the anterior side of the soleus muscle and the deep area of the fibularis brevis muscle.
The tendon of the fibularis brevis originally runs anterior to the tendon of the fibularis longus as they cross posterior to the lateral malleolus. The tendons of these muscles then enter precise osteofibrous canals defined medially by the calcaneus and laterally by the inferior fibular retinaculum. The fibularis brevis tendon is currently superior to the fibularis longus tendon, and both are inferolateral to the parallel edge of the extensor digitorum brevis. As they pass after the lateral malleolus, they continue horizontally.
Innervation
Motoric innervation to the fibularis brevis muscle is supplied by the superficial fibular (peroneal) nerve (L5-S1). This is a branch of the common fibular division of the sciatic nerve. Cutaneous innervation to the skin overlaying this muscle is mitigated by the spinal nerve roots L5, S1, and S2.
Blood supply
The Fibularis brevis and the further muscles of the lateral compartment of the leg are provided by the inferior and superior branches of the anterior tibial artery. In infrequent circumstances, the prevalent blood supply to the lateral compartment is the fibular artery, which is a component of the tibial artery.
An anastomotic network is located close to the ankle, and it supplies the fibularis brevis tendon and the muscle that is adjacent to it. The network contains the anterior lateral malleolar, arcuate, fibular perforating, lateral and medial plantar, lateral calcaneal, and lateral tarsal arteries. The venous blood from this muscle is transmitted by the anterior tibial vein.
Functions of Fibularis brevis muscle
Fibularis brevis travels both the subtalar (talocalcaneal) and talocrural (ankle) joints and thus contributes to the movements created across these joints. The primary function of the fibularis brevis is to evert the foot at the subtalar joint, which assists to fix the foot to its anatomical position after it has been inverted. This is especially essential when running or walking on irregular terrain.
Since fibularis brevis balances the inversion of the foot, it may also control the body from dropping to the opposite side when the person is balancing on one leg. The muscle also generates plantarflexion of the foot at the ankle joint while it is everting it.
Clinical notes
The area of the fibularis brevis tendon causes it susceptible to injury. Over time, it is disclosed to shear stress while gliding between the lateral malleolus and the tendon of the fibularis longus. If the foot evolves over-inverted, the extra downward force will be used to the lateral portion of the foot, generating tears or rupture of the fibularis brevis tendon. These damages are seen among tennis, basketball, and football (NFL) players. If the tendon of the fibularis brevis breaks, it can also generate an avulsion fracture of the fifth metatarsal tuberosity.
Microtears in the fibularis brevis tendon can over time outcome in fibular (peroneal) tendonitis. This is frequently described by pain and swelling to the posterolateral aspect of the ankle and foot. The pain is sluggish and aggravates with exertion. Acute management of this issue includes resting the limb, using ice packs to the involved region, compression bandage of the ankle, and elevation of the limb. Non-steroidal anti-inflammatory medicines can also aid in relieving the pain.
Physiotherapists suggest that people perform good stretching before beginning strenuous activities. This benefit promotes collagen synthesis and muscle fiber organization, therefore maintaining the muscle. The manual inversion and evert of the foot is one method for stretching the fibularis muscles. This can be accomplished by sitting on a chair with the leg relaxing on the opposite knee and maintaining the foot in the contrasting hand. Now gradually twist the sole toward the floor (eversion) and then back toward the roof (inversion). Another method includes sitting with the lower limbs similar to the bottom, covering a towel around the toes, and dragging the foot into dorsiflexion and inversion. The fibularis muscles will coincidentally be begun and extended in an attempt to check the motion characterized.
Assessment
When evaluating a person for a Fibularis Brevis injury, an general alignment of the leg and posture of the hindfoot must first be assessed. Persons that show hindfoot varus are predisposed to peroneal injury.
Observation: Upon observation, peroneal conditions will frequently present with swelling slightly posterior to the fibula or along the lateral wall of the calcaneus. Persons are generally present with posterolateral ankle pain that aggravates with movement and enhances with rest.
Palpation: may present with tenderness along the path of the tendons.
Range of motion testing may indicate pain with resisted eversion, passive inversion stretch, or resisted plantar flexion for the first time.
Strength testing is possible to produce aches and will be decreased going into eversion.
Special tests like the peroneal compression test should be conducted to assess aches, crepitus, and popping at the posterior border of the distal fibula during forceful ankle eversion and dorsiflexion.
Fibularis brevis muscle stretching
With inversion of the foot at the subtalar joint and dorsiflexion of the foot at the ankle joint, the fibularis longus muscle is stretched.

Fibularis brevis muscle strengthening
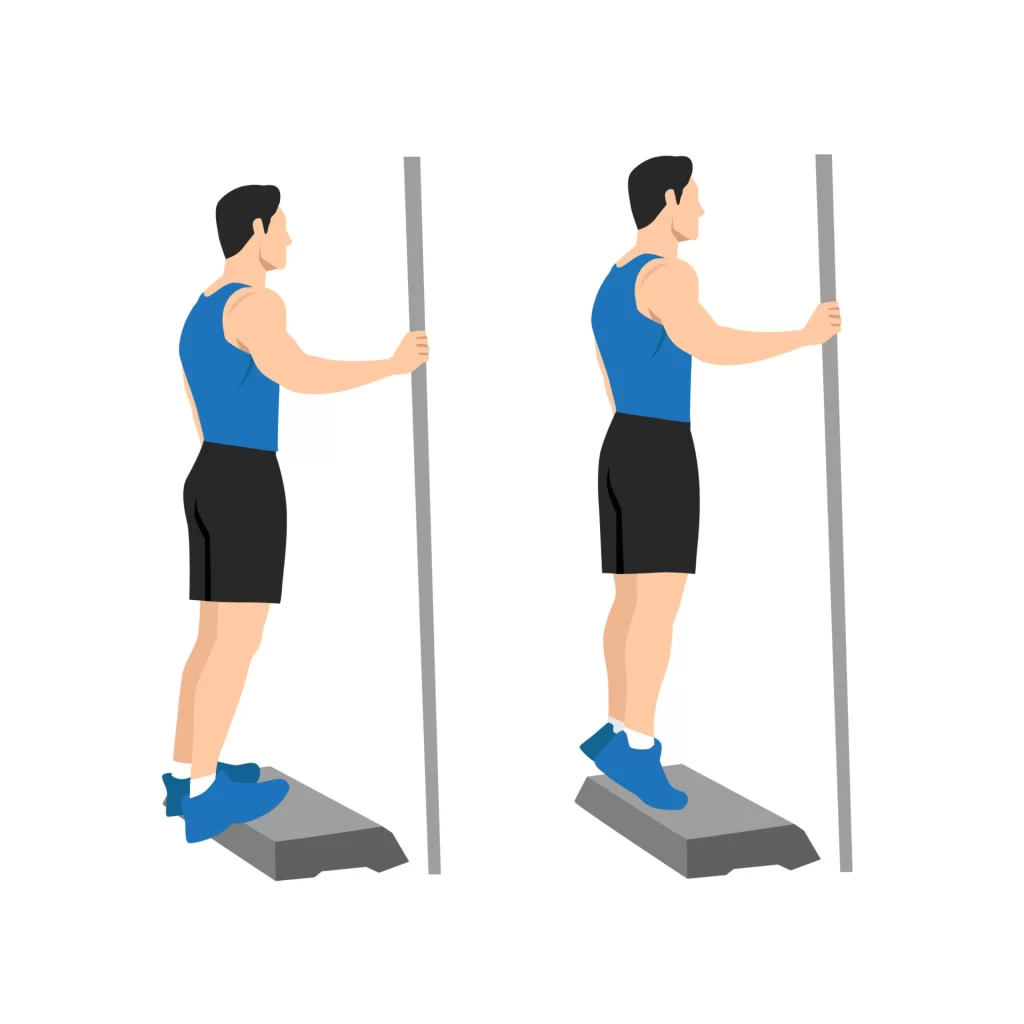
Standing calf raises
Stand on a step with the heels hanging over the border. Maintain onto a wall or handrail for assets. Stand erect and drag your abdominals in. Flex the knees barely so the calf muscles aren’t completely extended, and then lift the heels high. Maintain the position for a moment, then decrease your heels below the border of the step until a stretch in the calf muscles is sensed. Repeat as many at least five times or more, if likely, for three sets. As strength enhances, raise the number of repetitions, and also complete the calf raises on one leg at a time.
Balance and reach exercises
Stand after a chair to provide assistance, if required. Stand on one foot and flex the supporting knee gradually. Lift the arch of this foot while maintaining the big toe on the bottom. Maintain your foot in this position. With the hand that is distant away from the chair, arrive forward to barely cross the body, as if to touch the further side of the chair, by flexing at the waist. Avoid flexing the knee any other while bending. Conduct two sets of ten repetitions per side. To create the activity more difficult, reach distance forward and down.
FAQ
What causes pain in the peroneus brevis?
Overuse of the tendons usually generates pain, but a sudden injury like an ankle sprain can also cause it. Pain and swelling in your peroneal tendons are typically reduced after a few weeks of conventional therapies.
How long is recovery for peroneal brevis?
Healing from surgical repair of your peroneal tendon generally brings approximately four months. Your ankle will sense weak when it reaches out of the cast and it is essential to conduct a gentle range of motion exercises three or four times a day for three or four weeks after your cast is extracted.
How do you relax your peroneus brevis?
Put your involved leg a step behind your further leg. Maintaining your back leg straight and your back heel on the bottom, flex your front knee and gently get your hip and chest toward the wall until you sense stretching in your back leg’s calf. Keep stretching for at least 15-30 seconds. Do again 2 to 4 times.
How do you massage your peroneus brevis?
Put the ball under the muscle and get your knee down. You may put your hands over the leg and press should you need extra pressure. Maintain for 30 seconds and free. Recall massaging the further leg as well.
What does peroneus brevis pain feel like?
Pain on the outside of your foot, particularly over the main bony region on the outside of the forefoot, is one of the symptoms of a peroneus brevis tendon tear. Ache will most probably come on unexpectedly after a twisted ankle, or sudden forced motion of the ankle. You may keep bruising and swelling and the foot.



One Comment