How Long Does Whiplash Injury take to Heal?
Introduction
Injuries from rapid acceleration-deceleration motions, most frequently from car crashes, are referred to as whiplash-associated disorders (WAD). The mechanism of damage is called “whiplash,” although the symptoms that follow, such as pain, stiffness, headaches, and muscular spasms, are referred to as WAD.
WAD has an uncertain and irregular prognosis; some cases remain acute and recover completely, while others develop into chronic conditions that cause long-term pain and incapacity. Rest, pain management, and simple stretching exercises are advised as early intervention strategies.
Applied anatomy
The force and direction of impact, among many other criteria, determine which cervical spine anatomical components are affected by whiplash and whiplash-associated diseases (WAD). Any of these tissues may be the source of pain, and strain injuries can lead to subsequent oedema, bleeding, and inflammation:
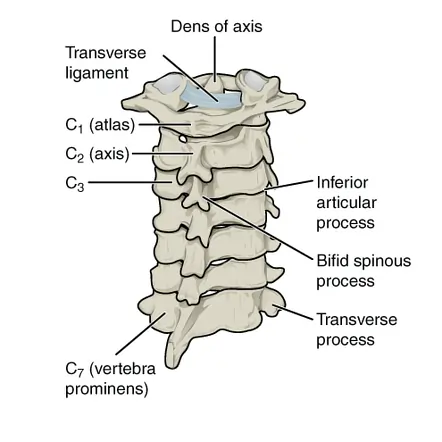
- Joints: zygapophyseal joints, Atlanto-axial joint, Atlanto-occipital joint
- Intervertebral discs and cartilaginous endplates
- Muscles
- Ligaments: Alar ligament, Anterior atlanto-axial ligament, Anterior atlanto-occipital ligament, Apical ligament, Anterior longitudinal ligament, Transverse ligament of the atlas
- Bones: Atlas, Axis, vertebrae (C3-C7)
- Nervous system structures: nerve roots, spinal cord, brain, and sympathetic nervous system
- The vascular system structures: the internal carotid and vertebral artery
- Adjacent joints: Temporomandibular joint, thoracic spine, ribs, shoulder complex
- Peripheral vestibular system
Pathology
The majority of WADs are thought to be mild soft tissue injuries that don’t show any signs of fracture.
The injury occurs in three stages:
- In stage 1, the upper and lower cervical spines flex.
- In stage 2, the cervical spine develops an S-shape before straightening and regaining its lordotic curve. Beyond normal physiological limitations, the cervical spine exhibits an atypical S-shaped curve, with the lower cervical segments hyperextended and the higher segments flexed at the same time.
- Stage 3 is characterized by complete spinal extension, resulting in the facet joint capsules being compressed by strong shearing forces.
According to the severity of their signs and symptoms, patients with WAD (whiplash) are categorized by the Quebec Task Force as follows:
- Grade 1: The patient reports neck pain, stiffness, or tenderness, but the physical examination reveals nothing.
- Grade 2, the patient has musculoskeletal symptoms, such as sore spots and a reduced range of motion.
- Grade 3, the patient also exhibits neurologic symptoms, such as muscle weakness, diminished deep tendon reflexes, and sensory deficiencies.
- Grade 4: A fracture is seen in the patient.
Causes
Whiplash occurs when you suddenly alter your direction or speed of movement. The following are some of the most frequent situations or activities that can cause whiplash:
- The most frequent cause of whiplash is motor vehicle crashes.
- Contact sports (such as football, hockey, rugby, etc.).
- Roller coasters.
Although the most frequent causes are listed above, there are numerous other ways that whiplash can occur. Under the correct conditions, even minor slips and falls might result in whiplash.
Symptoms
Acute or chronic whiplash disorders are both possible. The symptoms of chronic whiplash last for more than three months, whereas those of acute whiplash last for no more than two to three months. Acute WAD patients have decreased cervical mobility and extensive pressure hypersensitivity.
A complicated disorder, whiplash-associated disorder, causes psychological suffering along with a variety of motor, sensorimotor, and sensory function abnormalities. In order to screen for delayed onset cervical spine instability or myelopathy, it is crucial to do comprehensive spinal and neurological exams on individuals with WAD. Sub-occipital headaches are the most prevalent symptom, and they usually start or worsen seven days after the injury.
Primary Motor Features
- Restricted range of motion of the cervical spine
- Altered patterns of muscle recruitment in both the cervical spine and shoulder girdle regions (clearly a feature of chronic WAD)
- Mechanical cervical spine instability
Sensorimotor Features
- Loss of balance
- A disturbed neck influenced eye movement control.
Sensory and Psychological Features
- Psychological distress
- Post-traumatic stress
- Concentration and memory problems
- Sleep disturbances
- Anxiety
- Post-traumatic stress and anxiety are more common in women (19.7% and 11.7%, respectively) compared to men (13.2% and 8.6%)
- Depression
- Early depression: linked to increased intensity of neck and low back pain, tingling or numbness in the hands and arms, blurred vision, lightheadedness, and fractures
- Persistent depression: associated with older age, greater initial neck and low back pain, post-crash dizziness, anxiety, numbness/tingling, vision and hearing problems
- Depression may be present in around 5% of women and men.
Muscular Changes
- Neck stiffness
- Fatty infiltrate may be present in the deep muscles in the suboccipital region, and the multifidi may account for some of the functional impairments, such as Proprioceptive deficits, Balance loss, and Disturbed motor control of the neck.
Associated Symptoms
- Tinnitus
- Malaise
- Disequilibrium/Dizziness
- Thoracic, temporomandibular, facial, and limb pain
Differential Diagnosis
- Cervical spine fracture,
- Carotid artery dissection,
- Herniated disc,
- Spinal cord injury,
- Subluxation of the cervical spine,
- Muscle strain,
- Facet injury,
- Ligamentous injury.
Outcome Measures
- Neck Disability Index
- Visual Analogue Scale (VAS)
- Pain Catastrophizing Scale
- The Whiplash Activity and Participation List (WAL)
- Disabilities of the Arm, Shoulder, and Hand (DASH) in persistent Whiplash
- SF-36
- Functional Rating Index
- The Self-Efficacy Scale
- The Coping Strategies Questionnaire
- Patient-Specific Functional Scale
- General Health Questionnaire (GHQ)
Diagnosis
Examination
- Range of motion in your neck and shoulders.
- range of motion that hurts or makes discomfort worse.
- Tenderness in your neck, shoulders, or back.
- Reflexes, strength, and feeling in your limbs.
Imaging tests
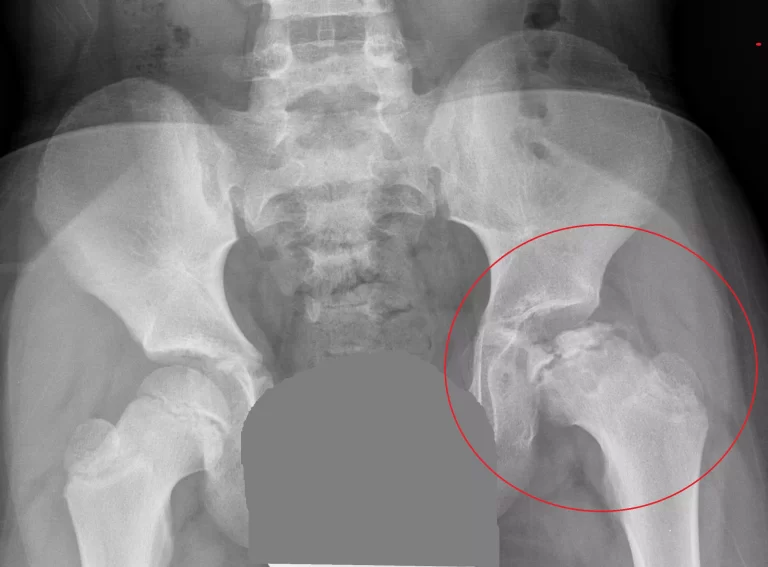
X-rays. Broken bones, arthritis, and other conditions can be seen on neck X-rays obtained from various perspectives.
CT scan. This particular kind of X-ray can produce fine-grained pictures of bone and highlight damage.
MRI. This imaging test creates finely detailed three-dimensional images using radio waves and a magnetic field. In addition to bone injuries, MRI scans can reveal soft tissue injuries such as ligament, disk, or spinal cord damage.
Treatment
The goals of whiplash treatment are to:
Manage your pain.
Restore your neck’s range of motion.
Return you to your normal activities.
Your treatment plan will depend on the extent of your whiplash injury. Some people just require at-home care and over-the-counter medications. Others could require physical therapy, pain management, or prescription medications.
Management
- The preferred course of treatment is typically education, returning to regular activities, and mobilization exercises.
- Exercises may help people with Whiplash-Associated Disorders with their neck pain and weakness.
- In cases of neck pain issues, therapeutic ultrasound may lessen the severity of the pain.
- Although nonsteroidal anti-inflammatory drugs and analgesics are used as treatments, “the evidence supporting pharmacological therapy for cervical facet joint pain or pain due to WAD is scarce.”
- There is little evidence to support the use of psychological therapies (such as relaxation or biofeedback) to treat pain following a musculoskeletal injury.
- Pain symptoms were also observed to be alleviated by lidocaine injection.
- The majority of treatments by themselves seemed to be only moderately effective; early mobilization was consistently the most successful, and combinations of treatment measures improved efficiency.
- Pain and psychological suffering can be effectively reduced with cognitive behavioral therapy. When started within six months of the injury, it works better.
Physiotherapy Management
Advice that encourages a return to regular activity and exercise is the basis of managing acute WAD, and current professional recommendations support this strategy.
- There is a lack of research on management strategies for patients with WAD.
- Individualized therapy approaches are necessary since people frequently do not fit into treatment categories due to a variety of circumstances and variances.
- Whiplash-associated disorder is a crippling and expensive condition that lasts for at least six months.
- Six months after the incident, 50% of victims with WAD grades 1 and 2 will still be disabled and have persistent neck pain. A sizable proportion have late whiplash syndrome (LWS), which is characterized by the persistence of notable symptoms for more than six months following an accident.
- Chronic WAD may result from a mix of psychological issues, such as a poor coping style, and the injury.
Acute Whiplash
The biopsychosocial treatment for whiplash patients must include education from general practitioners or physiotherapists, as this is important in preventing persistent WAD. The interventions’ primary objectives are:
- Giving the patient comfort
- Changing negative thinking about WAD
- Making the patient active
- Education aims to prevent and treat chronicity, improve therapy compliance, and remove therapeutic barriers.
- Written guidance and verbal instruction are beneficial for acute WAD (there is evidence that oral information is just as effective as an active exercise program).
- For subacute or chronic patients, a multidisciplinary program that incorporates education, physical activity, and behavioral therapy is ideal.
Different types of education include:
- Oral Education: Give oral instruction on the mechanisms underlying whiplash, with a focus on proper posture and physical exercise. Compared to rest and neck collars, it has a greater impact on pain, cervical mobility, and healing. Oral instruction may be just as beneficial as mobilization and active physiotherapy.
- Instructional video: When compared to standard care, a quick psycho-educational film at the patient’s bedside appears to have a significant impact on the patient’s subsequent pain and use of medications for acute whiplash patients.
The following details must be included in any patient education or information:
- Reassurance that there is a positive outlook after a whiplash injury.
- Encouragement to use recovery-promoting exercises to resume regular activities as soon as possible.
- Reassurance that using analgesia regularly is necessary to manage pain, which is common after a whiplash injury
- It is advised against wearing a soft collar because being active and/or doing workouts has been demonstrated to have better effects on pain and handicap.
Different types of exercise can be considered for WAD:
ROM exercises
Neck side flexion
- Place your arms next to your body and begin standing or sitting.
- In order to maintain a straight spine, contract your abdominal muscles and pull your shoulder blades downward.
- While maintaining the same posture for your shoulders, slowly bend your neck to bring your right ear closer to your right shoulder.
- Maintain this posture for five to ten seconds.
- Do it on the left side.
- Perform 2-4 reps on each side.
Neck flexion
- Pull the shoulder blades down and back.
- Bring your chin slowly up to your chest.
- For 15 to 30 seconds, hold.
- Perform two to four repetitions.
Neck extension
- Sit down in the beginning.
- Breathe slowly backward while looking up at the ceiling.
- For five to ten seconds, hold this position.
- Perform 5 repetitions.
Neck rotation
- Look over your shoulder and turn your neck gently to the left.
- Keep this posture for 20 to 30 seconds.
- Put on the other side.
- Do each side two or four times.
McKenzie exercises
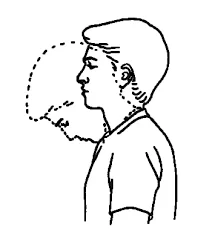
Head Retraction in Sitting
- With your head relaxed and angled slightly forward, take a comfortable seat.
- Without tilting, slowly bring your head back as far as it will go straight.
- Hold for two to three seconds, then return to the beginning position.
- Increase the backward movement progressively and repeat ten times every two hours.
Neck Extension in Sitting
- Perform the head retraction while seated.
- Tilt your head back as though you were staring at the ceiling while maintaining that posture.
- Hold each position for five seconds as you slowly rotate your head half an inch to the right and then to the left.
- Go back to where you were before.
- Every two hours, complete ten repetitions, aiming for greater extension each time.
Head Retraction in Lying
- Place your head close to the edge of the bed and lie face-up on a pillowless bed.
- To move the neck backward, tuck your chin in and softly press the back of your head into the mattress.
- Hold for a short while, then let go.
- Increase the backward movement progressively and repeat ten times every two hours.

Neck Extension in Lying
- With your hand under your head, lie face-up on a pillowless bed with your head near the edge.
- Move your head over the side of the bed slowly, then gently lower it back.
- Try to increase extension by turning your head half an inch to the right and then half an inch to the left.
- Use your hand to support your head as you return to the beginning position after holding the maximum extension for two to three seconds.
- Once every two hours, do this. After this workout, refrain from making sudden movements.
Postural exercises
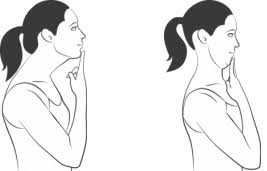
Chin Tucks Exercise
- Put two fingers at your chin’s base.
- Pull your head back and tuck your chin in gently. At the same time, keep your chin tucked in the whole time with your fingers.
- For three to five seconds, hold the end position.
- Take a moment to relax your neck (let it come forward).
- Try to complete two or three sets of ten reps.
One Arm Pec Stretch – At A Wall
- Reach a wall and extend one arm behind you, placing the palm against the wall.
- In order to lean forward and slightly away from the extended arm, pull in your stomach (do not arch your back).
- Your chest should feel stretched.
- Wait 30 seconds.
- Repeat on the opposite side.
Strengthening
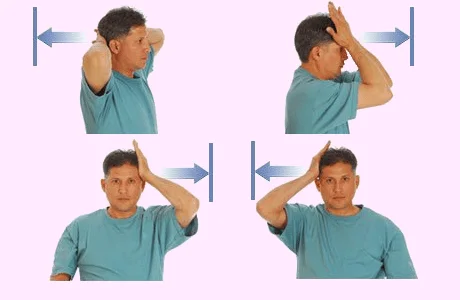
Neck Isometrics
First, place your feet flat on the floor and sit in a chair. To ensure that you are evenly balanced on your buttocks, your weight should be somewhat forward. Keep your head level and your shoulders relaxed. You might be able to maintain your equilibrium by using a chair with arms.
- Put your hand on your forehead. Use the muscles in your neck to resist. Hold for ten seconds. Calm down. Five times, repeat.
- Apply pressure to the side of your head and repeat the exercise. Five times, repeat. Change sides.
- Five times, repeat.
Motor control exercises.
Neck motor control
- Without a pillow beneath your head or neck, lie on your back with your knees bent. If this is uncomfortable, support your head with a tiny, folded towel.
- Start by focusing your gaze on a point on the ceiling.
- Next, move your gaze to a location on the wall that is slightly above your knees. As you nod slowly and gently, as though you’re saying “yes,” feel the back of your head glide up the bed. To feel the superficial muscles during the workout, lightly place your palm on the front of your neck. As they perform the head nod action, make sure they remain calm and soft.
- While you continue to glance down, stop when you feel the muscles starting to harden.
- After 10 seconds of holding the pose, let go. To return to the beginning position, look up to a point on the ceiling.
- Do this ten times.
Active treatment, which consists of:
- As homework, students can also be required to perform gentle, small range of motion exercises ten times in each direction.
- For individuals with acute WAD, daily usage of home exercise regimens that include relaxation techniques, training for the shoulder and neck range of motion, and general advice is proper therapy.
- There is significant proof that active mobilization and exercise regimens considerably lessen pain in the near term, and there is evidence that mobilization may help increase range of motion.
- The clinical treatment of neck pain frequently involves spinal manual therapy. Manual treatment, including passive mobilization, given to the cervical spine may help reduce pain, according to systematic evaluations of the few trials that evaluated manual therapy approaches alone.
- Wearing a collar goes against what the majority of studies suggest, which is exercise, mobilization, and activation. It has been demonstrated that early exercise therapy reduces whiplash injury pain and handicap more effectively than collar therapy. A soft collar is not as effective at relieving pain as exercise treatment, according to other studies. Soft collars are not advised for patients with acute WAD.
Chronic Whiplash
- The combination of the injuries and psychological variables leads to chronic WAD.
- Compared to those with non-specific chronic neck pain, persons with chronic WAD report worse health.
- Chronic WAD patients are treated with a multidisciplinary approach that includes cognitive, behavioral, and physical therapy, as well as neck exercises. Additionally, it produces favorable outcomes in terms of a decrease in sick leave and neck pain.
- Since behavioral treatment lessens the severity of the patient’s discomfort during troublesome everyday activities, it is employed in therapy. That is, modify treatment and planning.
- Short-term pain reduction is one benefit of exercise routines. For individuals with chronic WAD, exercise programs are the most effective noninvasive treatment. To lessen neck pain, coordination exercises should be included in the treatment.
- Negative thoughts are a significant factor in patients with persistent WAD. Specialists and physical therapists can help patients with chronic WAD by teaching them about the neurophysiology of pain and how it affects their negative attitudes and pain behaviors.
- Simple guidance works just as well as a more thorough and rigorous physiotherapy workout regimen.
Conclusion
- There is significant proof that multidisciplinary therapy is beneficial for the treatment of persistent whiplash. An exercise regimen is part of this therapy. When imaging diagnostics and other more severe clinical illnesses identified during examination have been ruled out, early mobilization works best.
- The severity of WAD, age, socioeconomic background, and pre-injury comorbidities all affect the prognosis. It has been demonstrated that full healing takes a few days to a few weeks. On the other hand, disabilities can range from ongoing pain to decreased physical function and can be permanent.
- The most common symptom is neck pain, but headaches and/or dizziness can also be persistent, chronic symptoms. Chronic pain that interferes with physical function and job can lead to a loss of lifestyle and income.
- WAD diagnosis and therapy are intricate processes that involve numerous problems. The management and results are influenced by the legal context, defensive medicine, age, comorbidities, and previous injuries. The ability to seek compensation for WAD or legal culture is a major factor in the wide range of diagnoses and symptom persistence.
FAQs
What is whiplash’s primary cause?
The most common cause of whiplash is a forceful, rapid backward and forward toss of the head. This frequently occurs after a rear-end collision. The neck’s muscles and tissues may sustain harm from this motion.
What keeps whiplash from happening?
For everyone inside the car, a properly placed head restraint is crucial to preventing whiplash injuries. Your ears should, at the absolute least, be level with the headrest’s top. Less than three inches should separate the headrest from the back of your head.
Whiplash affects which nerves?
The symptoms of cervical radiculopathy, which include tingling, weakness, and/or numbness that radiate down the shoulder, arm, hand, and/or fingers, can occasionally result from whiplash-induced compression or inflammation of one of the neck’s spinal nerve roots.
When whiplash occurs, what should one avoid?
Avoid doing anything that exacerbates the pain. For a few days, relax. If your neck is not harmed or at risk for further stress or damage, you can resume your regular activities.Stay away from sports, lifting, and other activities that could strain your neck.
References
- Whiplash_Associated_Disorders, physio pedia, https://www.physio-pedia.com/Whiplash_Associated_Disorders
- Whiplash (Neck strain). (2025, July 10). Cleveland Clinic. https://my.clevelandclinic.org/health/diseases/11982-whiplash
- Whiplash – Diagnosis and treatment – Mayo Clinic. (n.d.). https://www.mayoclinic.org/diseases-conditions/whiplash/diagnosis-treatment/drc-20378926
- Cronkleton, E. (2019b, September 9). What is neck flexion? plus exercises for improving your range of motion. Healthline. https://www.healthline.com/health/neck-flexion#rotation-exercise
- Dr.Emma, Dr.Emma, & Dr.Emma. (2025, June 29). 7 Effective McKenzie method exercises for alleviating neck and arm pain. TLSO Back Brace Guide & Reviews -. https://tlsobackbrace.com/7-effective-mckenzie-method-exercises-for-alleviating-neck-and-arm-pain/
- McQuilkie, S., DC. (2024, November 21). How to fix forward head posture – 5 exercises and stretches. PostureFlow (Formerly Back Intelligence). https://backintelligence.com/how-to-fix-forward-head-posture/