
Orbicularis Oculi Muscle
Introduction
The orbicularis oculi is a muscle in the face that closes the eyelids.
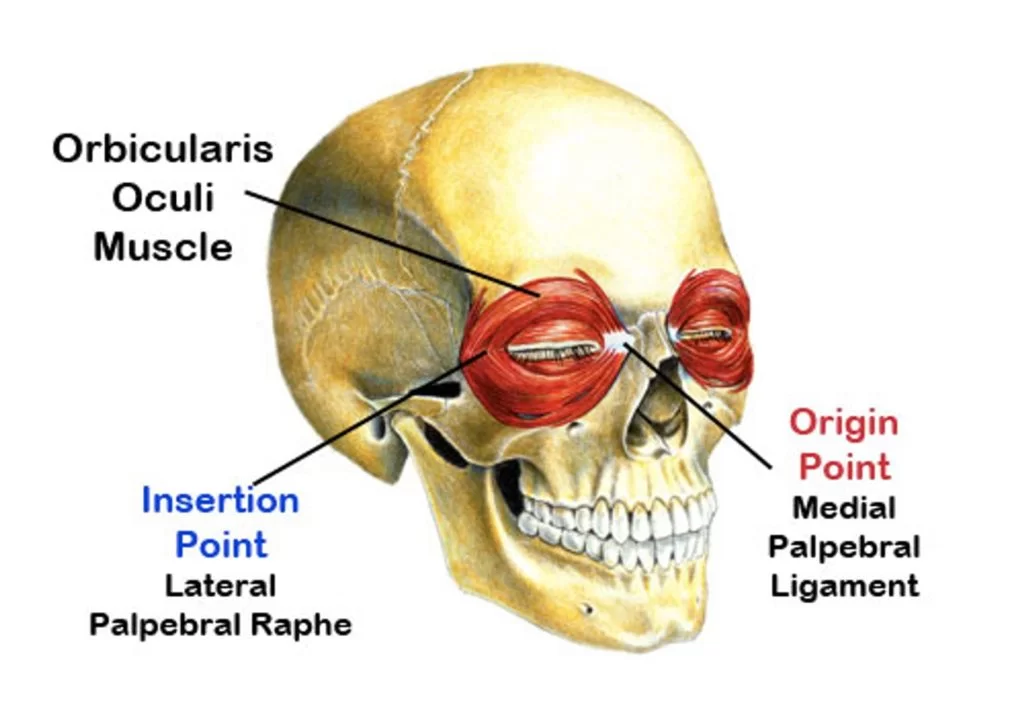
It arises from the nasal part of the frontal bone, from the frontal process of the maxilla in front of the lacrimal groove, and from the anterior surface and borders of a short fibrous band, the medial palpebral ligament.
From this origin, the fibers are directed laterally, forming a broad and thin layer, that occupies the eyelids or palpebrae, surrounds the circumference of the orbit, and spreads over the temple, and downward on the cheek.
Origin and insertion of the Orbicularis oculi:
Orbicularis oculi muscle (Musculus orbicularis oculi):
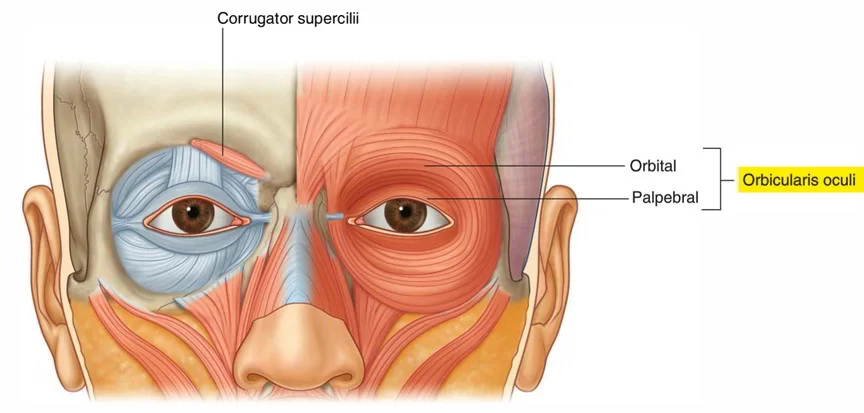
Orbicularis oculi is a flat, broad muscle that forms an ellipse around the circumference of the orbit.
It is composed of orbital, palpebral, and deep palpebral parts, each of which has its own specific set of attachments :
Orbital part:
- Overlays the orbital rim and originates from the nasal part of the frontal bone, frontal
- process of maxilla and medial palpebral ligament.
- The fibers encircle the orbit completely, extending into the soft tissues of adjacent regions.
- The orbital part has no bony insertions, but instead, it attaches to various soft tissue structures of the periorbital region.
- The upper fibers merge with the occipitofrontalis, corrugator supercilii, and depressor supercilii muscles, finally inserting into the skin and subcutaneous tissue of the eyebrow.
- The inferior and medial fibers of the orbital part blend with the levator labii superioris, levator nasolabialis, and zygomaticus minor muscles.
- Most peripheral fibers can stretch even further, loosely inserting into the temporal part of the epicranial aponeurosis.
Palpebral part:
- Originates from the superficial surface of the medial palpebral ligament.
- The muscle fibers compose the eyelids as they travel toward the lateral commissure of the eye.
- The superior and inferior fibers unite and insert into the lateral palpebral ligament (raphe).
- The most peripheral fibers of the palpebral part that travel along the margins of each eyelid form the ciliary bundle.
- Deep palpebral part: also known as the lacrimal part, originates from the lateral surface and lacrimal crest (superior part) of lacrimal bone.
- The fibers course laterally, passing posterior to the lacrimal sac.
- Some insert into the superior and inferior tarsi of eyelids, while others continue past the tarsi to insert into the lateral palpebral ligament.
Blood Supply and Lymphatics:
The orbicularis oculi muscle receives its blood from the branches of the facial artery and superficial temporal artery (which are branches of the external carotid artery), as well as the ophthalmic artery (which is a branch of the internal carotid artery).
The common carotid arteries arise from the brachiocephalic trunk on the right side and directly from the aortic arch on the left side.
At the superior border of the thyroid cartilage in the neck, each common carotid artery divides into the internal and external carotid arteries.
The external carotid artery continues superiorly and splits into a number of branches, including the facial artery, superior temporal artery, superior thyroid artery, lingual artery, facial artery, ascending pharyngeal artery, occipital artery, maxillary artery, and posterior auricular artery.
The facial artery then courses from the mandibular area, up the side of the nose, and to the medial canthus of the eye, where it is called the angular artery.
Branches of the facial artery and superficial temporal artery supply the orbicularis oculi muscle.
The internal carotid artery enters the skull through the carotid canal in the temporal bone.
It travels through the cavernous sinus and then splits off a major branch called the ophthalmic artery.
The ophthalmic artery enters the orbit through the optic canal.
Within the orbit, it divides into various branches, including the lacrimal artery, supraorbital artery, ethmoidal arteries, supratrochlear artery, central retinal artery, ciliary arteries, and muscular branches.
Some of these branches, such as the lacrimal artery and supraorbital artery, supply the orbicularis oculi muscle.
Nerve supply:
This muscle nerve supply is from the 7th cranial nerve – the facial nerve.
The upper half of the orbicularis oculi muscle nerve supply is from the temporal branch of the 7th cranial nerve (facial nerve), while the lower half of the muscle nerve supply is zygomatic branch of the 7th cranial nerve (facial nerve).
Function of the Orbicularis oculi muscle:
The muscle acts to close the eye and is the only muscle capable of doing so. Loss of function for any reason results in an inability to close the eye, necessitating eye drops at the minimum to surgical closure of the eye in extreme cases.
The palpebral portion acts involuntarily, closing the lids gently, as in sleep or in blinking the orbital portion is subject to conscious control.
When the entire muscle is brought into action, the skin of the forehead, temple, and cheek is drawn toward the medial angle of the orbit, and the eyelids are firmly closed, as in photophobia.
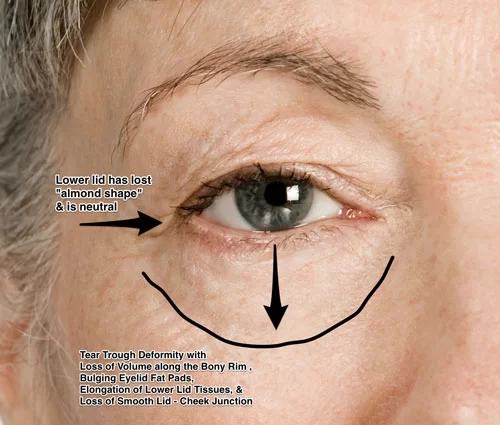
The skin thus drawn upon is thrown into folds, especially radiating from the lateral angle of the eyelids these folds become permanent in senescence, and form the so-called “crow’s feet.”
The Levator palpebrae superioris is the direct antagonist of this muscle; it raises the upper eyelid and exposes the front of the bulb of the eye.
In addition, the orbital and palpebral portions can work independently of each other, as in the furrowing of the brows by contraction of the orbital to reduce glare while keeping the eyes open by virtue of the relaxation of the palpebral.
Each time the eyelids are closed through the action of the orbicularis, the medial palpebral ligament is tightened, and the wall of the lacrimal sac is thus drawn lateralward and forward so that a vacuum is made in it and the tears are sucked along the lacrimal canals into it.
The lacrimal part of the orbicularis oculi draws the eyelids and the ends of the lacrimal canals medialward and compresses them against the surface of the globe of the eye, thus placing them in the most favorable situation for receiving the tears, it also compresses the lacrimal sac.
This part comprises two pieces: Horner’s muscle and the muscle of Riolan, the latter helps hold the eyelids together to keep the lacrimal passage waterproof.
Associated pathology such as a lesion of the facial nerve seen in Bell’s palsy results in the inability to blink or close the ipsilateral eyelid. Subsequent lack of irrigation increases the risk of corneal inflammation and ulcers.
A number of auxiliary muscles assist in cooperating with the eyelid muscles.
For example, the corrugator supercilii pulls the eyebrows to the bridge of the nose, making a roof over the middle of the forehead and forehead wrinkles, used mainly to protect the eyes from excess sunlight.
The procerus (pyramidalis) muscles, in the bridge of the nose, arising from the lower nasal bone to the lower forehead, on each side of the midline. The procerus muscles pull the skin into horizontal wrinkles.
The frontalis muscle, which runs from the upper forehead, halfway between the coronal suture (which traverses the top of the skull) and the top edge of the orbit, attaches to the eyebrow skin.
Since it pulls the eyebrows upward, it is the antagonist of the orbicularis oculi.
It is used in looking up, and increasing vision if there is insufficient light or when objects are far away.
Clinical Importance:
The involvement of orbicularis oculi in blinking and eyeball hydration can have important clinical consequences in day-to-day living.
Paralysis of the facial nerve (Bell’s palsy, stroke, trauma, infection) results in an inability to close the eye and failure to blink.
This causes inefficient lubrication and a condition known as dry eye syndrome (keratoconjunctivitis sicca), which manifests with redness, inflammation, irritation, discharge, and fatigue of the eyes.
These problems can also appear during prolonged computer usage. When exposed to visual stressors (glare, small fonts, etc.).
Blood flow and voluntary contraction of orbicularis oculi increase, resulting in squinting, less blinking, and tear evaporation.
The Benign essential blepharospasm is a condition in which involuntarily contraction of the orbicularis oculi muscles is the most common symptom. This highly affects the patient’s day-to-day activities like reading and driving, as the patient has difficulty holding the eyes open to do activities properly.
Periodic chemodenervation with botulinum toxin injections in the orbicularis oculi muscle can relax the involuntary contraction of the muscle and overall improve the symptoms.

3 Comments