

Tarsal tunnel syndrome: Physiotherapy Management
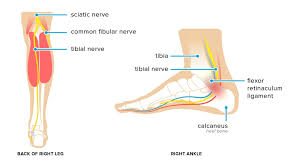
Tarsal tunnel syndrome is a condition caused by repeated pressure that results in damage on the posterior tibial nerve. Posterior Tibial nerve is the branches off of the sciatic nerve and is found near your ankle.
The tibial nerve Pas through the tarsal tunnel, which is a narrow passageway inside ankle that is bound by bone and soft tissue.
Damage of the tibial nerve mainly occurs when the nerve is compressed as a result of continuous or repeated pressure.
Definition :
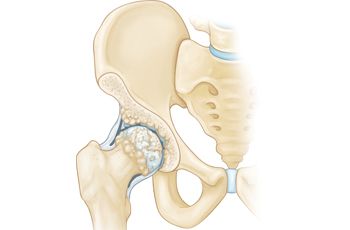
The tarsal tunnel is a channel between the medial malleolus, talus, calcaneus and the flexor retinaculum – a fibrous sheet that runs from the medial malleolus to the calcaneus.
The tunnel contains:-
-Flexor digitorum longus tendon
-Posterior tibial artery & vein
-Tibial nerve (yellow in image)
-Flexor hallucis longus tendon
The tibial nerve divides into two terminal branches – the medial and lateral plantar nerves – as it passes through the tarsal tunnel.
The medial calcaneal nerve branches from the tibial nerve at or superior to the flexor retinaculum.
Tarsal Tunnel Syndrome (TTS) is a rare compressive neuropathy of the tibial nerve or one of its branches as they pass under the flexor retinaculum.
In the TTS literature, the tibial nerve is also referred to as the posterior tibial nerve and TTS is also known as Posterior Tibial Nerve Neuralgia.
Some authors refer to compression of the deep fibular nerve as “anterior tarsal tunnel syndrome”.
This page is limited to the discussion of tarsal tunnel syndrome as the entrapment of the posterior tibial nerve or its branches. -Tibialis posterior tendon
Anatomy :
Posterior tarsal tunnel :-
an anatomic structure defined by
flexor retinaculum (laciniate ligament)
calcaneus (medial)
talus (medial)
abductor hallucis (inferior)
contents include :
tibial nerve
posterior tibial artery
FHL tendon
FDL tendon
tibialis posterior tendon
Tibial nerve
has 3 distal branches :
medial plantar
lateral plantar
medial calcaneal
the medial and lateral plantar nerves can be compressed in their own sheath distal to tarsal tunnel
bifurcation of nerves occurs proximal to tarsal tunnel in 5% of cases
Anterior tarsal tunnel
flattened space defined by
inferior extensor retinaculum
fascia overlying the talus and navicular
contents include
deep peroneal nerve and branches
EHL
EDL
dorsalis pedis artery
Presentation :
History :-
may have previous trauma or surgery
Symptoms :-
pain :-
pain with prolonged standing or walking
often vague and misleading medial foot pain
sharp, burning pains in the foot
numbness :
intermittent paresthesias and numbness in the plantar foot
may present as part of the “heel pain triad”
posterior tibial tendon deficiency (adult-acquired flatfoot), plantar fasciitis, tarsal tunnel syndrome
believed to be due to loss of static and dynamic stabilizers of the medial arch and susequent traction neuropathy on the tibial nerve
Physical exam :
tenderness of tibial nerve (tinel’s sign)
sensory exam equivocal
pes planus
muscle wasting of foot intrinsics
abductor digiti quinti or abductor hallucis
pain with dorsiflexion and eversion of the ankle
compression test :

compression plantar flexion and inversion of ankle
digital pressure over tarsal tunnel
highly senstitive and specific
Etiology :
Incidence is unknown. A higher prevalence is reported for women than men. It can be seen at any age. Causes of TTS include:-
-Repetitive stress activities such as running, excessive walking or standing
-Traumas such as fracture, dislocation or stretch injuries
-Heel varus or valgus
-Fibrosis
-Excessive Weight
-Space occupying lesions in tarsal tunnel region such as a ganglion, tumors, edema, osteophytes or varicosities
-Tendonitis
-Systemic diseases that cause ankle inflammation or nerve compromise (ex: diabetes mellitus, arthritis)
Many cases (20%-40%) are idiopathic.
Pathophysiology :
Tarsal tunnel syndrome results from the compression of the posterior tibial nerve or one of its two branches, the lateral or medial plantar nerve, within the tarsal tunnel.
Up to 43% of patients have a history of trauma including events such as ankle sprains. Abnormal biomechanics can contribute to disease progression.
Risk factors include systemic diseases such as diabetes mellitus, hypothyroidism, gout, mucopolysaccharidosis, and hyperlipidemia.
Clinical feacture :
Some of the symptoms are:-
-Pain and tingling in and around ankles and sometimes the toes
-Swelling of the feet and ankle area.
-Painful burning, tingling, or numb sensations in the lower legs. Pain worsens and spreads after standing for long periods :
pain is worse with activity and is relieved by rest.
-Electric shock sensations
-Pain radiating up into the leg, behind the shin, and down into the arch, heel, and toes
-Hot and cold sensations in the feet
-A feeling as though the feet do not have enough padding
-Pain while operating automobiles
-Pain along the Posterior Tibial nerve path
-Burning sensation on the bottom of foot that radiates upward reaching the knee
-“Pins and needles”-type feeling and increased sensation on the feet
A positive Tinel’s sign

Tinel’s sign is a tingling electric shock sensation that occurs when you tap over an affected nerve. The sensation usually travels into the foot but can also travel up the inner leg as well.
Risk factors:
Common risk factors for TTS include :
chronic overpronation or rolling inward of the foot when walking
flat feet or fallen arches
osteoarthritis
diabetes and other metabolic conditions
ankle or foot injury
jobs that require standing or walking for a long time, such as retail, teaching, mechanical, manufacturing, and surgical jobs
poorly-fitting shoes that allow the foot to pronate inward or do not support the arch and ankle
nerve disease
cysts, tumors, or small masses in the foot and ankle area
proliferative synovitis or inflammation of the synovial membrane
varicose veins or inflamed, enlarged veins
foot deformities
reflex sympathetic dystrophy
peripheral neuropathy conditions
generalized leg edema or swelling, especially related to pregnancy
being overweight
cause :
Tarsal tunnel syndrome results from compression of the tibial nerve, and it’s often caused by other conditions.
Causes can include:-
severely flat feet, because flattened feet can stretch the tibial nerve
benign bony growths in the tarsal tunnel
varicose veins in the membrane surrounding the tibial nerve, which cause compression on the nerve
inflammation from arthritis
lesions and masses like tumors or lipomas near the tibial nerve
injuries or trauma, like an ankle sprain or fracture — inflammation and swelling from which lead to tarsal tunnel syndrome
diabetes, which makes the nerve more vulnerable to compression
Imaging :
Radiographs :
weight-bearing radiographs provide osseous structure.

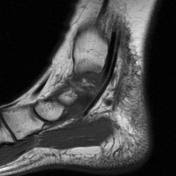
MRI :
may be helpful to rule out accessory muscle or soft-tissue tumorn .
EMG :
positive finding include :
distal motor latencies of 7.0 msec or more
prolonged SENSORY latencies of more than 2.3 msec
sensory (SAP) more likely to be abnormal than motor
decreased amplitude of motor action potentials of
abductor hallucis
or abductor digiti minimi
Differential Diagnosis :
The differential diagnoses of tarsal tunnel syndrome is broad, making diagnosis difficult. These include :
Compartment syndrome of the deep flexor compartment
Degenerative changes (calcaneal spurs, arthrosis of the joints of the foot)
Inflammatory conditions of the ligaments and fascia of the foot and ankle.
Intersection syndrome of the FHL and FDL at the knot of Henry
L5 and S1 nerve root compression
Morton metatarsalgia
Neurogenic intermittent claudication
Plantar fasciitis
Polyneuropathy
Retrocalcaneal bursitis
Prevention :
The exact cause of Tarsal Tunnel Syndrome (TTS) can vary from patient to patient.
However the same end result is true for all patients, the compression of the posterior tibial nerve and it branches as it travels around the medial malleolus causes pain and irritation for the patient.
There are many possible causes for compression of the tibial nerve therefore there are a variety of prevention strategies.
One being immobilization, by placing the foot in a neutral position with a brace, pressure is relieved from the tibial nerve thus reducing patients pain.
Eversion, inversion, and plantarflexion all can cause compression of the tibial nerve therefore in the neutral position the tibial nerve is less agitated.
Typically this is recommended for the patient to do while sleeping.
Another common problem is improper footwear, having shoes deforming the foot due to being too tight can lead to increased pressure on the tibial nerve.
Having footwear that tightens the foot for extended periods of time
even will lead to TTS. Therefore, by simply having properly fitted shoes TTS can be prevented.
Complications :
TTS tends to cause pain on the inside of the ankle and bottom of the feet, though it can also impact the toes and lower legs.
TTS is similar to carpal tunnel syndrome, involving a nerve being squeezed in a narrow, confined, tunnel-like joint space.
Common symptoms of TTS include:
searing, shooting pain
numbing
tingling
burning
the sensation of electric shocks
weakened ability to flex, bend, and fan out the toes
loss of sensation in the toes and bottom and sides of the feet
Management :
PHARMACOLOGICAL MANAGEMENT:
Pharmacological treatments are often used in combination with physical therapy management to optimize recovery and decrease functional disability.
-NSAIDS
-Corticosteroid Injections
-Pain Medications
SURGICAL MANAGEMENT :
Surgery is indicated for patients who have not benefited from conservative treatments such as physical therapy and have symptoms that significantly impact their daily life.
Individuals with a space occupying lesion tend to not to respond to conservative management and often require surgery.
Godges and Klingman have identified several characteristics that have been associated with a successful response to surgery.
The charateristics include; younger age, short history of symptoms, no previous history of ankle pathology, early diagnosis, and a determined etiology.
Posterior Tibial Nerve Decompression
If there is a space occupying lesion, the lesion will be removed
and decompression will not be done.
Cryosurgery
CONSERVATIVE MANAGEMENT :
Orthotics :
-Ankle bracing

-CAM walker
-Plantar arch taping

-Medial heel wedge
-Pt edu on footwear
Therapeutic Ex :
-Calf stretching

-Nerve mobility
Manual Therapy :
-Soft tissue massage
-Tibial nerve mobilization
Subacute Stage :
Goal :
increase
flexibility and STR
Therapeutic Ex :
Posterior tibialis strengthening
Settled Stage :
Goal :
promote
symmetrical flexibility, STR, and functional mobility
Therapeutic Ex :
-Posterior tibialis strengthening in WB
POSTOPERATIVE TREATMENT :
Phase-1 : (1-2weeks)
Goals :
Protect nerve, joint, and incision site
Control swelling
Reduce pn
Intervention :
-Immobilization with NWB precautions
-Ankle passive ROM

-RICE
-Gait training with AD
Phase-2 :- (3-6weeks)
goals :
-Prevent contractures
-Prevent scar tissue adhesions
-Increase joint mobility
Intervention :
-WBAT
-Gentle passive and active ankle stretching
-Begin tibial nerve glide with anti-tension technique (foot PF and inverted)
-Gait training to tolerance with protective splint
-Aquatic therapy
Phase-3:- (6-12weeks)
goals :
-Normal gait mechanics
-Increase ankle mobility
-Increase PF strength
-Specific skill development
Intervention :
-Gait training without splint
-Pain free theraband exercises
-Tibial nerve glide progression (foot everted and dorsiflexed)
-Weight bearing exercises
-Resistive exercises (impairment approach)
-Balance/proprioceptive training
-Specific skill development in pain free range
-Cardiovascular fitness
Acute Stage :
Goal:-
reduce pain and swelling
Physical Agents :
-Ice
-Pulsed ultrasound
-Phonophoresis
-E-stim
physiotherapy managment :
A doctor should always assess and treat symptoms of TTS early.
The first line of treatment for TTS is RICE, which stands for rest, ice, compression, and elevation.
Over-the-counter non-steroidal anti-inflammatory medications, or NSAIDs, such as acetaminophen or ibuprofen, can also help make symptoms more manageable.
For more severe or chronic cases, more aggressive treatment options exist, such as corrective devices, therapies, and in some cases, surgery.
Common ways to manage and treat TTS include :
Rest:
The easiest and most immediate way to reduce inflammation anywhere in the body is to stop using and putting pressure on the affected area.
How long an individual should rest the foot depends mostly on the severity of symptoms.
For minor cases, rest may mean replacing running with swimming.
For more severe cases, resting the nerve may require completely refraining from exercise and activity.
Ice:
An ice pack covered with a cloth or towel can be applied to the inside of the ankle and foot for 20-minute sessions to reduce inflammation.
It is best to have the foot elevated during this time.
Icing sessions can be repeated several times daily, as long as breaks of at least 40 minutes are taken.
Compression and elevation:

Compression and elevation
Compressing the foot, and keeping it raised above the heart, helps reduce blood flow to the foot, and so reduces inflammation.
Try wrapping the foot with an ACE wrap, and resting it on a pillow while sitting and sleeping.
Over-the-counter pain and anti-inflammatory medications: These can include ibuprofen and acetaminophen.
Full immobilization:-
For severe cases, especially those involving physical damage to the nerve, a cast may be necessary to restrict movement completely, allowing the nerve, joint, and surrounding tissues a chance to heal.
Injection therapy :
For very painful or disabling symptoms, anti-inflammatory medication, such as corticosteroids and local anesthetics, may be directly injected into the nerve.
Orthopedic devices and corrective shoes :
Podiatrists can make specialized shoes, and inserts that help support the arch and limit motions that can further irritate the inflamed nerve and surrounding tissues.
Shoes also exist to help prevent pronation or inward rolling of the foot.
Reducing foot pressure:
In some cases, wearing looser or larger fitting footwear and socks may help reduce tightness around the foot.
Physical therapy:
Physical therapy exercises can often help reduce symptoms of TTS long-term, by slowly stretching and strengthening the connective tissues, mobilizing the tibial nerve and opening the surrounding joint space to reduce compression.
Other types of physical therapy used for TTS include :-
ultrasound therapy
acupuncture
manual therapy
taping or bracing :
Ultimately, surgery may be performed for very severe or chronic cases of TTS that do not respond to any other form of medical or physical therapy.
Exercises :
As symptoms become less painful or easily irritated, strengthening exercises should be done to help prevent problems, including pronation or rolling of the foot, which can worsen symptoms.
Common exercises recommended for the treatment of TTS include :
Ankle pumps, circles, and eversion or inversion
A person can gently stretch the ankle by bending the foot towards the ground with the legs extended.
Sitting down with the legs extended, slowly and gently bend the foot at the ankles downward towards the ground, and then upwards towards the body, as much as possible, without pain. Repeat several times.
Slowly and gently roll the ankles through their circular range of motion as aggressively, as is comfortable, several times.
Slowly turn the ankles inward and outward, creating a windshield wiper motion, several times, as far as is comfortable.
Repeat all three exercises several times daily.
Heel-toe raises :
Standing straight, slowly raise or flex the toes upward, as far as possible, without pain.
Slowly lower the toes and gently raise the heels, putting gradual pressure on the ball of the foot.
Repeat this exercise 10 times and perform several times daily.
Pencil toe lifts :

Sitting down with the legs fully extended, place a pencil or pen on the floor directly below the toes and attempt to pick it up using only the toes.
Once the pencil is fully grasped, hold for 10 to 15 seconds.
Relax the toes.
Repeat 10 times and perform several times daily.
Balance exercises :


Standing straight slowly raise one leg and rest the sole of the raised foot on the inner calf of the other foot.
Hold for at least 10 to 15 seconds or, as long as is comfortable, without overstretching the inner ankle and foot. If too wobbly, stop by lowering the foot and restarting the exercise.
For a more intense version of this exercise, gradually lift the raised leg further in the air, away from the body.
Plantar fascia stretch :

Sitting down with the legs extended, as far as comfortable, reach out and grasp the big toe and top of the sole, then gently pull backward. This can also be done using a stretching band, dishtowel, or sock.
Stretch the foot backward until a stretch that runs from the sole to the ball of the foot is felt.
Hold for 30 seconds before slowly releasing the foot.
Repeat the stretch at least three to five times, three times daily for several weeks, even after initial symptoms have greatly improved to reduce the chances of them returning.
The plantar fascia ligament can also be stretched by rolling out the arch, sole, and heel in a gentle downward motion on something round, such as a soup can, therapy ball, tennis ball, or rolling pin.
Gastrocnemius stretch:

Standing a small distance away from a wall, step one foot forward, closer to the wall, and lean in, pressing the hands into the wall while keeping the back leg straight.
This position should look somewhat similar to an assisted lunge.
Widen or deepen, the stretch as feels comfortable or produces a notice, pain-free stretch along the full-length of the back of the calf.
Start by holding the stretch for 10 to 15 seconds, gradually increasing holding time to reach 45-second intervals.
Repeat the stretch three to five times consecutively, three times daily for several weeks.
For a more intense stretch, try standing on a step with the foot halfway hanging off the edge, and then gently push the heel downwards. Hold for as long as feels comfortable, up to 10 times daily.
Soleus muscle stretch :

Repeat the steps of the gastrocnemius stretch, except with the back leg being stretched bent at the knee.
To increase the stretch, place something under the front or ball of the foot, or prop the ball of the foot up on the wall.
Prognosis :
The prognosis of tarsal tunnel is variable.
In patients with an identifiable etiology due to mass effect diagnosed early in the disease course, the response is generally favorable.
Patients without an identifiable cause and who do not respond to conservative therapy generally do not do as well with surgical intervention.
A positive Tinel sign is a strong predictor of surgical relief.



7 Comments