
Proprioception Neuromuscular Facilitation(PNF)
What is Proprioceptive Neuromuscular Facilitation?
Proprioception:-having to do with any of the sensory receptors that give data concerning movement and position of the body.
Neuromuscular:-including the nerves and muscles.
Facilitation:-making more straightforward.
Proprioception Neuromuscular Facilitation is the activity in view of the standard of practical human life anatomy and neurophysiology.
it uses:
proprioceptive cutaneous auditory input to deliver practical improvement in motor output and can be an essential component in the recovery cycle of sports-related injuries.
Proprioceptive Neuromuscular Help (PNF) is a bunch of stretching techniques generally utilized in clinical conditions to upgrade both active and passive range of movement to work on motor performance and aid rehabilitation. PNF is thought of as an ideal stretching method when the point is to increase the range of movement, particularly as respects momentary changes.
Herman Kabat developed proprioceptive neuromuscular facilitation (PNF) during the 1940s and further created Dorothy Voss and Margaret Knott. PNF assists with reestablishing normal movement by focusing on creating a sequence of movements and how the agonist and antagonist muscles cooperate to create volitional movement. PNF involves reflexive movement as a reason for learning more volitional movement. The thought is that one should have the option to move before he can crawl and crawl before he walks.
PNF centers around mass movement designs that are corner to corner and look like useful movements. The body doesn’t work in parts, be that as it may, but rather overall. To advance these mass movement designs, PNF utilizes a multi-sensory approach, integrating the hearable, visual, and tactile systems. PNF permits the patient to comprehend what ordinary movement feels like using different senses through the utilization of manual contacts to prompt the patient and facilitate movement.
Neurophysiologic Basis Of PNF
Sherrington….,
concepts of facilitation and inhibition
stretch reflex
neurophysiologic phenomenon
Facilitation

Facilitary:- an impulse causing the enrollment and release of additional motor neurons in the spinal cord.
brings about increased excitability in the muscles.
weak muscles would be helped through facilitation.
Inhibition

Inhibitory:- any improvement that makes motor neurons drop away from the release zone and away from the spinal cord.
inhibition brings about decreased excitability of motor neurons.
muscles spasticity can be diminished.
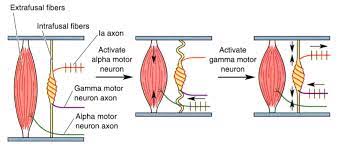
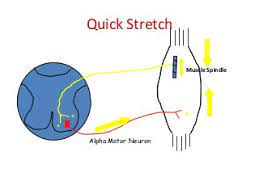
Stretch Reflex
The stretched reflex includes two kinds of receptors:
muscles spindle
Golgi tendons organs
Neurophysiological Phenomena
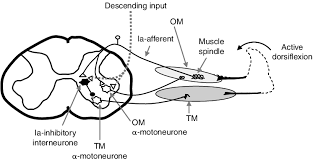
Reciprocal Inhibition
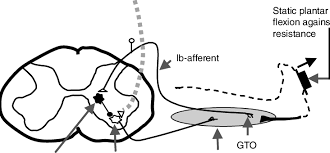
Autogenic Inhibition
Reciprocal Inhibition:- is the second mechanism that manages the connections of agonist and antagonist muscles.
Autogenic Inhibition:- what happens in a contracted or extended muscle as a diminishing in excitability in view of inhibitory signs sent from the Golgi tendon organs (GTOs) of a similar muscle.
Precaution
- Certain precautions should be taken while performing PNF stretches as they can put included pressure on the targeted muscle group, which can build the risk of soft tissue injury.
- To assist with decreasing this risk, it is vital to incorporate a conditioning stage before a most extreme, or intense effort is utilized.
- Likewise, prior to undertaking any type of stretching it is crucially critical that a thorough warm-up be finished.
- Heating up before stretching does various valuable things, yet fundamentally its motivation is to set up the body and psyche for more strenuous movement.
- One of the manners in which it accomplishes this is by assisting with expanding the body’s center temperature while likewise expanding the body’s muscle temperature.
- This is fundamental to guarantee the greatest advantage is gained from your stretching.
Uses Of PNF
- PNF treatment is utilized to increase strength flexibility coordination and functional mobility.
- the primary objective of treatment is to work with the patients in accomplishing a development or stance.
- stretches, as well as diagonals levelheaded exercise patterns, are utilized to further develop ADL functional mobility and athletic performance.
- it is principally utilized in orthopedic rehabilitation for musculoskeletal injuries and in neurological recovery.
- PNF can be utilized for any condition anyway the patient’s condition level might get change.
Basics Principles Of PNF
- Resistance
- Irradiation & reinforcement
- Manual contact
- Stretch
- Verbal commands
- Traction & approximation
- Timing
- Body positioning & body mechanics
Resistance:-

contradicting power to the patient’s movement is called resistance.
how much resistance gave by during a movement should be right for the patient’s condition and the objectives of the action. this is called optimal resistance.
resistance is utilized in the treatment to:
- work with the capacity of the muscle to contract.
- increase motor control.
- help the patient add attention to movement and its heading.
- increment strength.


Irradiation & Reinforcement:–
Irradiation:- the spread of reaction to the stimulus is called irradiation.
reinforcement:- means to strengthen by the new expansion make stronger is called reinforcement.
Effects:
maximal resistance might be utilized to make light or flood from a stronger pattern to a weaker pattern or from a stronger group of muscles within a pattern to weaker groups within a similar pattern.
Manual Contact:
Effects:
stimulates the muscles.
stimulates the synergistic muscles to build up the movement.
advance trunk stabilization and indirectly assist the limb with motioning.
prevents confusion.

contact or manual contact
contributes the facilitation by stimulating the exteroceptors and it should be:
intentional
directional
agreeable
Stretch:
the stretch boost happens when the muscles are lengthened.
the lengthened place of the muscle is the beginning place of each pattern and the stretch is kept up all through the movement.
every one of the parts of a pattern should be stretched at the same time.
effects:
boost the action of the muscle spindle.
any contraction of muscles on the stretch will bring about movement and the brain knows not muscles but a movement.
Verbal Commands:-
the volume with which the orders are provided influences the strength of resulting muscle contraction.
louder command major areas of strength for when contraction is required.
gentler and more quiet tone when the objective is relaxation and the relief of pain.
the commands are divided into three parts:
planning:- Prepares The patient for Activity “prepared”.
activity:- advise the patient to begin the activity ” now pull your leg up and in”.
correction:- advise the patient how to address and change the activity “continue to pull your toes up”.
commands used:
hold
pull/push
relax
Traction:
traction is the lengthening trunk or its extremity.
traction force is applied continuously to keep up with all through the movement and joined with proper resistance.
joint partition stimulates joint receptors.
muscle stretch stimulates the muscle spindle to stretch receptors.
works with alpha motor neurons.
works with strength.
Approximation:

pressure through the joint stimulates joint receptors.
work with alpha motor neurons.
work with strength.
uses:
promote stabilization.
work with weight bearing and contraction of postural muscles.
work with upstanding responses.
oppose some part of the movement for example approximation toward the finish of shoulder flexion to oppose scapula rise.

Timing:
timings are the sequencing of movements.
typical timing of most planned and effective movements is from distal to proximal.
timing for emphasis includes changing the typical sequencing of movement to stress a specific muscle or wanted action.
Body Positioning & Body Mechanics:

the therapist’s body ought to be in the line with the movement.
shoulder and pelvis face course of movement.
the therapist stands in walk standing position.
the resistance comes from the therapist’s body while the hands and arms stay relatively relaxed.
Principles of PNF
- all people have possibilities that are not completely evolved.
- motor development happens cerviocaudal succession proximodistal direction.
- early motor behavior is dominated by reflex action though mature motor conduct is upheld or built up by postural reflex.
- the development of motor conduct has cyclic patterns as proven by the shift between flexor and extensor predominance.
- the objective coordinated action is comprised of turning around the movement.
- ordinary development and stance are reliant upon synergism and an equilibrium interaction of the antagonist.
- creating motor conduct is communicated in a methodical grouping of complete examples of development and stance.
- typical improvement has a methodical succession yet comes up short on bit-by-bit quality and for the most part, shows cross-over.
- improvement in motor capacity relies on engine learning.
- recurrence of feeling and redundant action is utilized to advance and hold motor advancing as well concerning g the improvement.
Effect Of PNF
While there are various PNF stretching methods, every one of them depends on stretching a muscle as far as possible. Doing this
triggers the reverse mitotic reflex, a defensive reflex that quiets the muscle to prevent injury. “PNF makes the mind go ‘I don’t believe that muscle should tear’ and makes an impression on letting the muscle loosen up somewhat more than it would typically,” says sociologist Ashley Dark.
PNF is a stretching technique used to build ROM and flexibility. PNF builds ROM by increasing the length of the muscle and
increasing neuromuscular productivity.
PNF Techniques
Reversal Of Antagonists:
A gathering of techniques that consider agonist contraction followed by antagonist contraction immediately or relaxation.
Dynamic Reversals (Slow Reversals ): Uses isotonic compressions of first agonists, then antagonists performed against resistance. Compression of the stronger pattern is chosen first with movement to weaker pattern example. The appendage is traveled through the full scope of movement.
Indications: Impaired strength and coordination among agonist and antagonist, restrictions in the scope of movement, fatigue
Stabilizing Reversals: Uses rotating isotonic contractions of first agonists, then, at that point, antagonists against resistance,
permitting, without a doubt, an extremely limited range of motion. Impaired strength, stability, equilibrium, coordination.
Rhythmic Stabilization (RS):
Uses alternating isometric contractions of first agonists, then, at that point antagonists against resistance, no movement is permitted.
Indications: Impaired strength and coordination restrictions in ROM impaired stabilization control and equilibrium.
Repeated Contractions, RC (Repeated stretch): Repeated isotonic contractions from the protracted reach, instigated by fast stretches and upgraded by resistance; are performed through the range or part of the range at a mark of weakness. The method is repeated(i.e., three or four stretches) during one example or until contraction weakens. Impaired strength, the commencement of movement, and limitation in dynamic ROM.
Rhythmic Initiation (RI):
Voluntary relaxation followed by passive movements advancing to dynamic helped and dynamic resisted movements to at last dynamic movements. Verbal orders are utilized to set the speed and rhythm of the movements. Light following is utilized during the resistive stage to work with movement.
Signs Inability to relax, hypertonicity (spasticity, inflexibility); trouble starting movement; motor planning deficits (apraxia or dyspraxia); motor learning deficits; communication deficits (aphasia).
Hold-Relax
One PNF procedure that Dark says can set off the reflex is usually called “hold-relax.” This includes:
Setting a muscle in a stretched position and holding for a couple of moments. Contracting the muscle without moving (likewise called isometric, for example, pushing tenderly against the stretch without really moving. This is the point at which the reflex is set off and there is a “6-to 10-second open door for a past ‘typical’ stretch,”
Dark says.
Relaxing the stretch, and afterward stretching again while breathing out. This subsequent stretch ought to be deeper than the first.
Contract-Relax
Another normal PNF technique is the contract-relax stretch. It is practical, identical to hold-relax then again, actually as opposed to contracting the muscle without moving, the muscle is contracted while moving. This is once in a while called isotonic stretching.
For example, in a hamstring stretch, this could mean a mentor gives resistance as a competitor gets the muscle and pushes the leg down to the floor.
Hold-Relax-Contract
A third method, hold-relax- contract, is like hold-relax-, then again, actually, in the wake of pushing against the stretch, rather than relaxing into a passive stretch, the competitor effectively drives into the stretch. For example in a hamstring stretch, this could mean connecting with the muscles to raise the leg further, as the mentor pushes in a similar heading.
Despite strategy, PNF stretching can be involved in most muscles in the body, as per Dark. Stretches can likewise be changed so you can do them alone or with an assistant.
Rhythmic Rotation
Relaxation is accomplished with the slow, repeated turn of a limb where limitation is taken note of. As muscles loosen up the appendage is gradually and delicately moved into the range. As another pressure is felt, RRo is repeated. The patient can utilize dynamic movements(voluntary efforts) for RRo or the advisor can perform RRo inactively. Voluntary relaxation when conceivable is significant. Signs Relaxation of excess tension in the muscles (hypertonia) joined with PROM of the range- restricting muscles.
Keeping that in mind, PNF Techniques have wide applications in treating individuals with neurologic and musculoskeletal conditions most often in restoring the knee, shoulder, hip, and lower leg.
PNF Stretching Techniques
it is in many cases a blend of passive stretching and isometrics contractions that energize flexibility and coordination throughout the limb’s entire range of motion.
PNF is utilized to enhance day-to-day stretching and is utilized to make fast acquires in the scope of movements to assist competitors with further developing execution great scope of movement improves biomechanics diminishes weakness and assists with overuse injuries.
Contract Relax
moves the body parts inactively into the agonist design.
the patient is told to move by contracting the antagonist isotonically against the resistance.
at the point when ROM is restricted by muscle tightness.
Hold Relax
starts with isometrics contraction of the antagonist against resistance followed by concentric contraction of the agonist’s muscles.
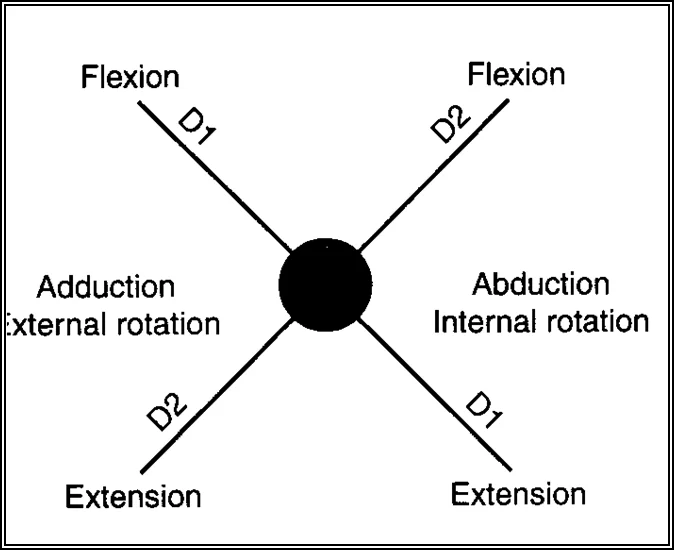
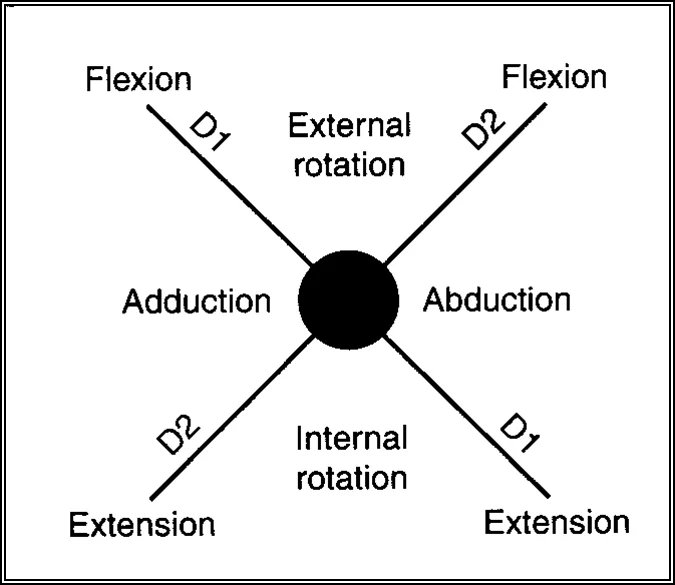
PNF Pattern
The PNF practice patterns include three parts: flexion-extension abduction-adduction, and internal-external rotation.
The examples imitate a diagonal rotation of the upper extremity, lower extremity, upper trunk, and neck.
The patterns enact muscle bunches in lengthened or stretched positions.
The upper and lower limits each have two patterns: D1 and D2 movements focusing on flexion and extension.
The patterns are utilized to further develop the scope of movement at the joint as well as present obstruction preparation. This will assist with further developing the patient’s strength.
Upper Extremity
D1 Flexion

Beginning Position
Shoulder extended, abducted, and internally rotated
Forearm pronated
Wrist ulnar deviated
Fingers extended
Hand Position
Hand set in patient’s palm so that patient can grip and flex wrist to the radial side.
hand on the Anterior-medial surface of the patient’s arm just simply over the elbow.
Movements To End Position
Shoulder flexed, adducted, and externally rotated
Forearm supinated
Wrist radially deviated
Fingers flexed
D1 extension

Starting Position
Shoulder flexed, adducted, and externally rotated
Forearm supinated
Wrist radially deviated
Fingers flexed
Hand Position
Hand over the dorsal-ulnar part of the patient’s hand.
on the back horizontal surface of the patient’s arm simply over the elbow.
The Movement To Ending Position
Shoulder extended, abducted, and internally rotated
Forearm pronated
Wrist ulnar deviated
Fingers extended
D2 flexion

Starting Position
Shoulder extended, adducted, and internally rotated
Forearm pronated
Wrist ulnar deviated
Fingers flexed
Hand Position
Hand over the dorsal-ulnar part of the patient’s hand.
Hand on the anterior-lateral surface of the patient’s arm simply over the elbow.
Movements To End Position
Shoulder flexed, abducted, and externally rotated
Forearm supinated
Wrist radially deviated
Fingers extended
D2 Extension

Starting Position
Shoulder flexed, abducted, and externally rotated
Forearm supinated
Wrist radially deviated
Fingers extended
Hand Position
Hand set in the patient’s palm so the patient can grasp and flex the wrist to the ulnar side.
Hand on the posterior-medial surface of the patient’s arm simply over the elbow.
Moving To Ending Position
Shoulder extended, adducted, and internally rotated
Forearm pronated
Wrist ulnar deviated
Fingers flexed
Lower Extremity
D1 Flexion

Starting Position
Hip extended, abducted, and internally rotated
Ankle plantarflexed
Foot everted
Toes flexed
Hand Position
Hand on the distal foremost medial part of the thigh.
Hand on the medial part of the dorsal surface of the foot.
Movements To Ending Position
A hip flexed, adducted, and externally rotated
Ankle dorsiflexed
Foot inverted
Toes extended
D1 Extension

Starting Position
A hip flexed, adducted, and externally rotated
Ankle dorsiflexed
Foot inverted
Toes extended
Hand Position
Hand on the distal back horizontal thigh.
Hand on the horizontal part of the plantar surface of the foot.
Movements To Ending Position
Hip extended, abducted, and internally rotated
Ankle plantarflexed
Foot everted
Toes flexed
D2 Flexion

Beginning Position
Hip extended, adducted, and externally rotated
Ankle plantarflexed
Foot inverted
Toes flexed
Hand Position
Hand on the distal front horizontal thigh.
Hand on parallel part of the dorsal surface of the foot
Movements To Ending Position
A hip flexed, abducted, and internally rotated
Ankle dorsiflexed
Foot everted
Toes Extended
D2 Extension

Beginning Position
A hip flexed, abducted, and internally rotated
Ankle dorsiflexed
Foot everted
Toes Entended
Hand Position
Hand on the distal back medial thigh (folded over the back part of the femur).
Hand on the medial part of the plantar surface of the bundle of the foot.
Movements To Ending Position
Hip extended, adducted, and externally rotated
Ankle Plantarflexed
Foot inverted
Toes flexed
PNF In Sports
here are a few basic principles while finishing PNF stretching:
- leave 48 hours between PNF stretching schedules.
- perform just a single activity for every muscle group in the session.
- for each muscle group total of 2-5 sets of the chosen exercise.
- each set should consist of one stretch held for up to 30 seconds after the contracting phase.
- PNF stretching isn’t suggested for anybody younger than 18.
- on the off chance that PNF stretching is to proceed as a different activity meeting an intensive warmup comprising of 5-10 minutes of light vigorous activity and some powerful stretches should go before it.
FAQ
What is an example of PNF?
For example, a typical PNF hamstring stretch includes lying on your back with one leg brought up in the air. While contracting the hamstring and attracting the leg to the ground, a partner applies gentle force in the opposite direction.
What are 3 PNF techniques?
There are three distinct types of PNF stretches, Contract-Relax Method. Agonist-Contract Method. Contract-Relax-Agonist-Contract Method.
How is PNF performed?
target muscle (TM) being protracted (“stretched”)
hold in a stretch position while the person contracts (activates) the TM to 50-60% of maximum isometric contraction for 4-6 seconds.
follow this with a more limited relaxation of the muscle for 2-3 seconds “let go.”
What does PNF mean?
Proprioceptive Neuromuscular Facilitation(PNF) is a high-level type of flexibility training, which involves both the stretching and contracting of the muscle group being targeted.
Why is PNF stretching important?
PNF stretching can work on your scope of movement, or ROM. It can likewise help your muscle flexibility and strength. Increase ROM. By stretching or lengthening the muscle spindles and Golgi tendon organs (GTO) through PNF, you can increase your ROM.
What is the most effective PNF stretching technique?
The hold-relax with agonist contraction is the best PNF stretching procedure because of helps through both reciprocal and autogenic inhibition.
What are the disadvantages of PNF stretching?
However, partner PNF stretching has 2 significant disadvantages – 1) it requires an assistant, and 2) has more risk in that your partner should impart and answer properly to guarantee that the stretch is performed securely. Self- PNF stretching could take out both of those downsides.




2 Comments