

Quadriceps Muscle strain
What is Quadriceps Muscle strain?
A quadriceps muscle strain is acute tearing damage of the quadriceps. This injury is usually due to an acute stretch of the muscle, usually at the same time as a forceful contraction or repetitious functional overloading.
Damage to the quadriceps muscle group can be painful and debilitating. Strains and contusions of the quadriceps are typical in athletics and result in lost time from activity and competition.
Clinically Relevant Anatomy
The Quadriceps femoris muscle is a hip flexor and a strong knee extensor. It is situated in the anterior compartment of the thigh.
This muscle is formed of 4 sub-components:
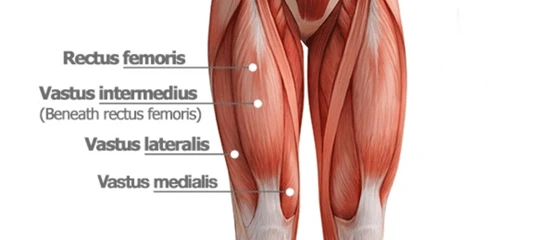
- Rectus femoris (RF)
- Vastus lateralis
- Vastus medialis
- Vastus intermedius
A quadriceps muscle strain is an acute tearing injury of the quadriceps, which usually happens due to an acute stretch of the muscle and forceful contraction at the same time or repetitious functional overloading.
Epidemiology
Quadriceps injuries are typical injuries in athletes with the muscle flat to muscle strains in conditions requiring explosive movements as seen in certain sports.
Rectus femoris muscle is the most generally involved in a quadriceps injury, factors predisposing RF comprise crossing two joints, a high ratio of Type II fibers, and having a complex musculotendinous architecture
Vastus muscle injury is the least common, and the vast intermedius muscle is most commonly impacted by contusions.
Quadriceps tendon rupture is an unusual debilitating diagnosis, arising more often in older men.
Classification of Quadriceps Strains
Factoring in pain, loss of muscle strength, and physical exam results in a grading system benefits provide guidance for treatment, rehabilitation, and eventual recovery to play.
Grade I (mild) strains to impact only a limited number of fibers in the muscle. There is no reduction in strength and there is a fully active and passive range of motion. Pain and tenderness are usually delayed to the next day.
Grade II (moderate) strains have almost half of the muscle fibers torn. Acute and effective pain is accompanied by swelling and a minor reduction in muscle strength.
Grade III (severe) strains describe the complete rupture of the muscle. This indicates either the tendon is disconnected from the muscle belly or the muscle belly is torn in 2 parts. Painful swelling and pain and a complete loss of function are characteristic of this type of strain.
Muscle injuries also are largely classified as either acute or chronic injuries.
Acute injuries: are usually the development of a single traumatic event and generate a macro-trauma to the muscle. There is an apparent link between the cause and detectable symptoms. They mostly happen in contact sports such as rugby, soccer, and basketball because of their active and high-collision nature.
Overuse:(chronic or exercise-induced damages) is subtler and usually happens over a longer period. They result from repetitious micro-trauma to the quadriceps. Analyzing is more challenging since there is a less obvious connection between the cause of the injury and the symptoms.
Grades of a quadriceps strain
Grade 1 symptoms: Symptoms of a grade 1 quadriceps strain are not always serious sufficiently to stop training at the time of injury. A spasm may be felt in the thigh and a general feeling of tightness. The athlete may feel mild distress on walking and running might be difficult. There is improbable to be swelling. A lump or area of spasm at the area of injury may be touched.
Grade 2 symptoms: The athlete may feel an impulsive sharp pain when running, jumping, or kicking and be incapable to play. Pain will make walking challenging and swelling or mild bruising may be seen. The pain would be felt when pressing in on the supposed location of the enclosure muscle tear. Straightening the knee against antagonism is likely to cause pain and the injured athlete will be incapable of fully bending the knee.
Grade 3 symptoms: Symptoms consist of intense, impulsive pain in the front of the thigh. The patient will be untrained to walk without the aid of crutches. Bad swelling will occur immediately and significant bruising within 24 hours. A static muscle contraction will be painful and is possible to produce a bulge in the muscle. The patient can wish to be out of competition for 6 to 12 weeks.
Causes of Quadriceps muscle strain
Among quadriceps muscles, the rectus femoris is considerably frequently strained, due to causes such as muscles traveling two joints, those with a high percentage of Type II fibers, and muscles with difficult musculotendinous architecture.
Acute injuries usually happen as a result of:
- Impulsive deceleration movement of the leg,
- Violent contraction of the quadriceps,
- The immediate deceleration of an overstretched muscle while fast changing direction,
- Muscle exhaustion,
- A traumatic event, macro-trauma to the muscle,
- Due to connection sports such as rugby, soccer, basketball, etc
- Overloaded by repeated eccentric muscle compactions of the knee extensor mechanics
- As a consequence of overuse
- Repetitious micro-trauma to the muscle
- Excessive passive stretching can also lead to strains.
There is an increased risk of rupture due to a few medical situations or due to the use of specific medications, including the following:
- Systemic lupus erythematosus (SLE), etc.
- Obesity
- Rheumatoid arthritis
- Gout
- Kidney disease
- Diabetes mellitus
- Acute strain injuries of the quadriceps commonly happen:
- In sports that regularly require sudden forceful eccentric contraction of the quadriceps during limitation of knee flexion and hip extension eg soccer, rugby, and football.
- When high forces happen across the muscle–the tendon branches with eccentric contraction.
- When excessive passive stretching or activation of a maximally stretched muscle happens.
When a muscle is fatigued?
There are commonly three mechanisms of injury for a quadriceps strain:
- Impulsive deceleration of the leg (e.g. kicking),
- forceful contraction of the quadriceps (sprinting) and
- quick deceleration of an overstretched muscle (by a quick transition of direction).
Signs and symptoms of Quadriceps muscle strain
Symptoms of a quadriceps strain may contain:
- Bruising
- Swelling
- Trouble moving the affected leg or walking
- Cramping
Aside from pain, a quad strain may also show the following symptoms:
- Pain and swelling in the thigh
- Observable inflammation or bruising
- Difficulty flexing and straightening the knee
- Leg weakness and reduced range of motion
- Intense pain when running, jumping, or kicking
Diagnosis of Quadriceps muscle pain
Physical examination:
After receiving a comprehensive medical history, a careful physical examination is done for observation, palpation, strength testing, and evaluation of movement.
The examiner has a close look at the affected site and observes swelling and bruising. Also, observes the patient in standing and walking, and look for postural irregularities. Palpation of the quadriceps muscle is done along the whole length of the muscles. It’s required to determine swelling, thickening, tenderness, defects, and masses if present. Strength testing of the quadriceps includes the resistance of knee extension and hip flexion. Sufficient strength testing of the rectus femoris includes resisted knee extension with the hip flexed and extended. For this, the best way to estimate the patient is in both sitting and prone-lying positions. The prone-lying position allows optimum examination of quadriceps motion and flexibility. Pain is usually sensed by the patient with resisted muscle activation, passive stretching, and direct palpation over the muscle strain.
Ely’s test: Ely’s test is a physical test used to evaluate rectus femoris spasticity or tightness. The patient lies prone and the therapist stands next to the patient, at the flank of the leg that is to be tested. One hand is placed on the lower back, the other hand maintains the leg at the heel. Then bend the knee passively, the heel should touch the buttocks. For comparison test both sides. The test is positive if the heel cannot touch the buttocks, and the hip of the tested side rises from the table, the patient feels pain or pricking in the back or legs.
Radiographs: Radiographs are useful to determine the etiology of the pain in the quadriceps muscles, which can be a muscle strain or stress rupture etc.
Ultrasound: Ultrasound is usually used as it is affordable. But it also has a disadvantage, in that it’s highly operator dependent and needs a skilled and professional clinician. An advantage is that it can image the muscles dynamically and evaluate for bleeding and hematoma appearance via Doppler.
Magnetic resonance imaging (MRI): Magnetic resonance imaging (MRI) is used to give precise images of muscle injury.
Differential Diagnosis
- Myositis ossificans
- Soft tissue tumors/ bone tumors
Examination
After receiving a detailed history, a careful analysis should ensue including observation, palpation, strength testing, and evaluation of movement.
Observation: The therapist will have a comparative look at the injured area, observing for swelling and bruising in particular. They should also observe the patient in standing and walking, looking for postural anomalies. They may present with an obvious deformation such as a bulge or weakness in the muscle belly.
Palpation: Palpation of the quadriceps muscle should happen along the whole length of the muscles and the aponeuroses. This is required to determine swelling, thickening, tenderness, defects, and masses if present. Acute compartment syndrome should be evaluated if there is tenseness of the fascial envelope enveloping the compartment and pain out of ratio to the clinical situation.
Strength testing: the quadriceps should maintain the resistance of knee extension and hip flexion. Sufficient strength testing of the rectus femoris must include resisted knee extension with the hip flexed and extended. This is best conducted by evaluating the patient in both a sitting and prone-lying position. The prone-lying position also allows for optimum review of quadriceps motion and flexibility. Pain is generally felt by the patient with resisted muscle activation, passive stretching, and direct palpation over the muscle strain.
Assessing tenderness: any palpable weakness and strength at the onset of muscle injury will determine the grading of the injury and give direction for further diagnostic testing and treatment.
Risk factors of Quadriceps muscle strain
You may be more likely to strain a quadricep if you:
- Have exhausted muscles
- Overstretch the leg muscles
- Play individual sports, such as football or soccer
- Do not warm up enough before exercising
Weak quadriceps muscles are more likely to tear. The following can donate to quadriceps weakness, and increase your chance of sustaining a tear:
- Tendinitis in the quadriceps
- Utilizing steroids
- Being inactive for long periods
- Keeping specific chronic
Outcome Measures
- Muscle Strength Testing
- Range of motion.
- Volunteer activation by superimposing percutaneous electrical stimulation onto an isometric quadriceps. When the muscle is activated, the electrical stimulation does not cause additional pressure above the voluntary contraction.
Treatment
Medical Treatment
Management of quadriceps injuries relies on the type and location of the damage. A whole quadriceps tendon tear with loss of the extensor mechanism needs surgery and reattachment of the quadriceps tendon. All other quadriceps damages can be managed conservatively utilizing the accepted method to treat muscle strain injuries in the initial time, being the RICE (rest, ice, compression, and limb elevation) principle or the POLICE principle.
Surgery:
Conservative treatment effects in a good outcome. But there are individual specific indications in which surgical intervention might be useful, these are:
- Large intramuscular hematoma,
- Full (III degree) strain,
- Tear of a muscle,
- Partial or II degree strain if more than half of the muscle belly is torn.
Physiotherapy Treatment
Rest:
Rest controls the worsening of the injury. Place the injured knee to rest the first few days after the trauma, this can control the appearance of a large gap within the muscle, and reduce the size of the hematoma, and the size of the connective tissue scar. A short period of immobilization accelerates the formation of granulation tissue at the site of injury during the initial stage. Gradually mobilization should be started to optimize the healing by improving the strength of the injured muscle, preventing muscle atrophy, the loss of strength, and extensibility.
Ice therapy:
Ice therapy lowers the intra-muscular temperature and reduces blood flow.
Compression:
Compression wrap or bandage can help to reduce both blood flow and extra interstitial fluid accumulation. It desires to prevent hematoma formation and interstitial edema, thus reducing tissue ischemia.
Elevation:
The elevation of an affected leg beyond the level of the heart results in a reduction in hydrostatic pressure and also decreases the collection of interstitial fluid, so there is less swelling at the place of injury.
Therapeutic Ultrasound:
Ultrasound benefits improve the process of healing. It delivers the thermal effect, which is of help to chronic muscle strains, it also decreases inflammation and promotes healing, which can help with an acute injury.
Transcutaneous electrical stimulation (TENS):
Transcutaneous electrical stimulation (TENS) can be used to reduce pain and swelling. It can help pump out inflammation, reduce pain, and desensitize nerve fibers. It even can strengthen muscles and re-educate.
Shockwave therapy:
Shockwave therapy is used to create an improvement in healing and regeneration by a single hearing wave impulse which stimulates the healing of soft tissue, mainly by deterring the function of afferent pain receptors and improving angiogenesis. Therefore, it increases blood flow by inducing a healing process refereed by the caused inflammatory process
Mobilization:
Mobilization is done to restore normal pain-free motion of the leg. The areas above and below the injury site are mobilized originally. It should be carried out gently and initially not mobilizing over the site of injury. But as the pain reduces, mobilization over neighboring sites to the injury can be started gently.
Active range of motion exercises:
Active range of motion is done once the injured leg is recovered well. This phase includes a simple range of movement exercises like knee flexion-extension, ankle motion, and toe movements. But before starting with AROM exercises passive movements are suggested.
Stretching Exercises:
Stretching exercises should be accomplished carefully to the point of pain, but without pain. This contains techniques such as passive, active-passive, dynamic, and proprioceptive neuromuscular facilitation stretching. e.g. Static quad stretch, hip flexor stretch, etc.
Strengthening Exercises:
Strengthening exercises are done to slowly raise the load that is put via a muscle. Initially, isometric or static exercises are advised, then move to low-level pain-free exercises and then to advanced exercises with the resistance band and finishing with sports-specific running and sprint drills. Strengthening exercises can also be done in an aquatic pool by using the antagonism of water.
Isotonic Exercise:
Isotonic exercises are started with the lightest free weight, 3 sets of 10 repetitions up to 3 times a day. Terminal knee extensions at 20 degrees, raise as comfort and knee flexion allows. Once terminal knee extensions are done properly without extensor lag, free consequences are added to the SLRs and terminal knee extensions, and weight is improved gradually.
Eccentric Exercises:
These exercises include higher-speed eccentric exercises that contain plyometric and sports-specific activities such as squat jumps, split jumps, bounding and depth jump, single leg bounding, backward skips, lateral jumps, lateral bounding, plyometric box hops, eccentric ahead pulls, eccentric back steps, eccentric lunge slides, single and double leg deadlifts, etc.
Isokinetic Exercises:
Isokinetic exercises are very high-intensity exercises such as swimming, running, and treadmill walking Isokinetic strength testing should be conducted under both concentric and eccentric movement conditions.
Exercises for Quadriceps muscle strain
Standing quadriceps stretch

If you are not stable on your feet, hold on to a chair, counter, or wall.
Bend the knee of the leg you want to stretch, and reach after you to grab the front of your foot or ankle with the hand on the identical side. For example, if you are stretching your right leg, utilize your right hand.
Keeping your knees next to each other, pull your foot toward your buttock until you feel a mild stretch across the front of your hip and down the front of your thigh. Your knee should be indicated straight to the ground, and not out to the side. Maintain the stretch for at least 15 to 30 seconds. Repeat 2 to 4 times.
Quadricep and hip flexor stretch (lying on the side)

Lie on your side with your right leg apartment on the floor and your hand holding your head.
Bend your top leg, and come after you to grab the front of that foot or ankle with your other hand.
Stretch your leg back by dragging your foot toward your buttock. Feel the stretch in the front of your thigh. If this induces stress on your knee, do not do this stretch. Keep the stretch for at least 15 to 30 seconds. Repeat 2 to 4 times.
Hamstring stretch (lying down)
Lie lying on your back with your legs straight. If you feel pain in your back, place a small towel roll beneath your lower back.
Holding the back of your involved leg for help, lift your leg straight up and toward your body until you feel a stretch at the back of your thigh. Hold the stretch for at least 30 seconds. Repeat 2 to 4 times.
Leg Laterally Rotated
Raise your leg similarity to the bent leg. Don’t arch your back. Keep your abdominals engaged. Another take is to achieve this with your toes straight into the air. You could also add an ankle weight to improve the test level. Act 2 sets of 15 repetitions per leg once a day. (When you can efficiently perform this exercise for at least 30 repeats, stop and restart with the other sports.)
Bridge Exercise

Lie on your back with your knees bent to ready for the bridge motion.
Bridge Exercise with Straight Leg Raise
Keep pelvis level as you raise hips/pelvis and buttocks into the air. Pause, and raise your leg. Hold for 3-5
seconds, then replace the leg to the floor and repeat with the opposing leg. Return your buttocks to the ground and rest when you can no longer keep your pelvis from wobbling or your buttocks from falling downward. Portray on both legs. Perform 2 sets of 10 repetitions per leg once per day.
Squats

Squats can be completed in many ways including ball squats, double-leg squats, and single-leg squats.
Start with 1/4 squats, or as far as relaxing. As you become stronger, achieve deeper squats.
Start with 2 sets of 10 reps and slowly increase to 3 sets of 15 before moving.
Wall Squat
Stand with your pelvis, back, and head touching a wall. Your feet will be about hip-width apart and far sufficiently out from the wall. When you glide down, your knees will make a 90-degree angle. Make sure your knees follow your feet, and you can see your toes. Try to have the knee track toward your second toe to guarantee proper alignment of the knees.

Wall Squat
From your starting position, slowly lower your body down and hold for a time. As you enhance, lengthen the amount of time you hold the wall squat. Be confident to keep your pelvis, back, and head against the wall. Keep the motion pain-free.
(A variation to improve activation of the VMO would be to squeeze a ball between the knees as you perform the exercise. Normally the ball would be about 12 inches in diameter.) Perform 3 sets of 15-20 seconds holds once a day.
Wall Squat with Leg Raise
From your starting place, slowly lower your body down and hold for a time. Extend your knee. Hold for 3-5 seconds originally. As you enhance, lengthen the amount of time you hold the wall squat and knee-raised position. Be sure to hold your pelvis, back, and head against the wall. Keep the motion pain-free. Perform 2 sets of 10 repeats once per day. Gain the time carried up to 10-15 seconds per rep.
Plank Exercise Raise

Keep your chin folded down so you’re looking straight into the ground. Your thighs, buttocks, stomach, and back muscles are all committed. Elbows should be straight under the shoulders. Keep your body straight, do not tilt. Perform 2 sets of 30-60 seconds once a day.

Step Ups
Start with a box height that is relaxing for you to step up on. Be sure to support the knee in alignment with your second toe. Step up and keep your pelvis level and your knee in alignment. Be sure to engage the buttocks muscles and fully lock out the knee. Produce slowly back down to the ground. The emphasis should be on the slow eccentric (lowering) back to the ground for 1 second up and 3 seconds down. Perform 2 sets of 15-20 repetitions once per day.
Thigh strain stretching exercises
After an injury, the muscle usually pulls up to protect the injury and control further injury. Whilst this may be useful in the early stages, it can slow the function of producing sport and make you more prone to future damages if not corrected. We recommend seeking experienced advice before trying any self-help.
Active range of motion exercises
This exercise is helpful in the early stages of rehabilitation whilst movement is particularly restricted.
Only bend and straighten the knee via its full pain-free range of movement.
This can be accomplished in the sitting position, the standing position, and lying down.
Do not overstretch too soon. If it is painful then avoid it!
Perform 10 reps at a time, at least 3 times each day.
Static quadriceps stretch
This can be achieved either standing or laying in your front.
Pull the foot of the injured leg towards your buttock until you can sense a mild stretch on the front of the thigh.
To improve the stretch, tilt your hips back.
Keep this position for 20-30 seconds and repeat it 3 times.
Do this at least 3 times per day.
Passive quadriceps stretch
This affects utilizing some outward force to help stretch the muscles. Perform either this stretch or the static quad stretch overhead, there is no condition to do both!
You can utilize a wall by standing in front of it, flexing the knee, and bending back onto the foot.
Or can get a partner to push your leg in the laying down the stretch.
Also, maintain for 20-30 seconds and repeat 3 times, at least 3 times each day.
Hip flexor stretch
This stretch will concentrate on the rectus femoris and Iliopsoas muscles.
Kneel with one knee on the floor and the other foot out in show with the knee tendency.
Move your hips ahead and keep the back upright.
You should feel a stretch at the front of the hip and the top of the thigh.
Maintain for 20-30 seconds, repeat 3 times, at least 3 times each day.
Thigh strain strengthening exercises
Strengthening exercises can start as soon as they are pain-free to complete. If it hurts, don’t do it. In grade 1 tears, activities may be created from day 2.
Isometric quadriceps contractions
Static contractions can be utilized very early on in the recovery process. They are concerned about contracting the muscle without any motion of the leg. This can be done in standing or posing with the legs out straight.
Maintain contractions for 10 seconds at a time.
Rest for 5 seconds before repeating and perform 10 repeats. As your strength enhances, improve sets to 2 or 3 sets of 10 reps.
Although this exercise is exhausting it will sustain muscle bulk and provide you back to full fitness faster.
Continue with this exercise every day until you can complete the concentric exercises below.
Straight leg raise
This exercise can be accomplished lying down or sitting. Lying down is more comfortable. Sit flat on the floor with your legs directly out in front of you.
Lift one leg off the floor holding the knee straight.
Maintain for 3 to 5 seconds before dropping back to the ground. Repetition 10 to 20 times.
This activity can be done daily.
Advance the exercise by improving the length of hold and the number of reps.
Ankle importance can be added to improve the problem.
Knee extensions
The quad muscles are accountable for straightening the knee. This exercise can be achieved using no weight, ankle weights, an antagonism machine, or an opposition band.
Start with no weight and then move to either ankle weights or an opposition band.
Straighten the knee then slowly produce to the start position.
Begin with 2 sets of 10 reps and slowly increase to 3 sets of 15 raising the weight or opposition when satisfied to do so.

Lunges
Lunges are a little easier version of a squat and are periodically called split squats. Start with an expansive stance.
Bend the back knee towards the floor, but don’t let it touch.
Keep your back upright around and don’t let the front knee move forwards above the toes.
Start with 2 sets of 10 reps with the injured leg in front and then do 2 sets of 10 with the injured leg behind. Slowly rise to 3 sets of 15.
To make it harder, you can add either a dumbbell in per hand or a barbell over the shoulder
Rehabilitation Protocol Example
Phase1: Acute Phase week 1-2
| Goals: | Reduce pain and inflammation Slowly enhance flexibility and ROM Retard muscular atrophy and power loss Improve healing of a muscular strain |
| Protection | Avoid extreme active or passive lengthening of quadriceps |
| Rehab | RICE–Rest, Cryotherapy, reduction wrap, and elevation The use of crutches originally to promote rest and immobilization of the quadriceps NSAIDS Soft tissue mobs/IASTM Pulsed ultrasound Conventional TENS Ankle pumps, isometric quadriceps groups, hamstring sets, glut sets |
Phase 2: Subacute phase (weeks 3 – 12)
| Goals | Recover pain-free quadriceps strength, advancing via full ROM Develop neuromuscular control of the trunk and pelvis with a progressive increase in movement and speed training for functional motions. |
| Precautions | Avoid end-range lengthening of quadriceps if painful |
| Rehab | Cryotherapy NSAIDS Electrical stimulation Initial isometrics with quadriceps contractions done with the knee fully extended and in various positions at 20-degree increments as knee flexion enhances May suspend isometrics when can sit comfortably, perform straight leg raises at 0 degrees, 20 degrees, and 40 degrees Isotonics–start with the lightest free weight that the athlete can lift; three sets of 10 repeats up to three times per day Terminal knee extensions created at 20-degree increments as comfort and knee flexion authorize Once terminal knee extensions are done correctly without extensor lag, free weights are added to the SLRs, and terminal knee extensions Increase weight by no more than 2-3 pounds at any provided time and grow no shortly than every two consecutive workdays As the athlete approaches maximum weight, somewhere almost 15-20pounds, isokinetic exercises are tried Conditioning through upper body workouts, swimming, treadmill walking Biking when knee ROM more significant than 100 degrees of flexion |
Phase 3 ( week 12+)
| Goals | Symptom-free during all movements Normal concentric and eccentric strength via full ROM and speed Enhance neuromuscular control of the trunk and pelvis Incorporate postural control into sport-specific motions |
| Precaution | Train within the symptoms-free intensity |
| Rehab | Ice – Post-exercise – as needed Treadmill intermediate to high intensity as accepted Isokinetic eccentric exercise at end ROM (in hyperflexion) STM/IASTM Plyometric jump exercise 5-10 yard accelerations/decelerations Single-limb balance windmill connects with weight on an unstable surface Sport-specific drills that incorporate postural control and advanced speed |
Eccentric protocol
Contain higher velocity eccentric Ex that contains plyometric and sports-specific movements
Examples: contain squat jumps, split hops, bounding and depth hops, single leg bounding, backward skips, lateral hops, lateral bounding, zigzag jumps, bounding, plyometric box hops, eccentric backward steps, eccentric lunge drops, eccentric forward pulls, single and double leg deadlifts, and split stance deadlift
Return to Sports Criteria
- Full power without pain in the lengthened state testing position
- Full Range of motion without pain
- Image of sport-specific activities at competition speed without symptoms.
- Isokinetic muscle testing should be conducted under both concentric and eccentric movement conditions.
- Gain 120° of knee flexion with hip extended
Clinical Bottom Line
Acute strain injuries of the quadriceps commonly appear in athletic competitions such as soccer, rugby, and football. Do these sports regularly require impulsive forceful eccentric contraction of the quadriceps during restriction of the knee? exion and hip extension. Higher points across the muscle–tendon branches with eccentric contraction can lead to strain injury. Excessive passive stretching or activation of a maximally pulled muscle can also cause strains. Of the quadriceps muscles, the rectus femoris is frequently strained. Several factors predispose this muscle and others to more regular strain injury. These contain muscles crossing two joints, those with a high percentage of Type II? Muscles with complex musculotendinous architecture. Muscle exhaustion has also been shown to play a part in acute muscle damage.
Therapy is grounded on 3 principles:
- POLICE or RICE
- Knee mobilization
- Training of the quadriceps action
Prevent quadriceps strains
You’re more possible to strain your quadriceps also after an initial injury. Cold muscles are more likely to maintain damage. Therefore, the best way to control damage is to perform a full warmup before any exercise or stretching. Consistently allow for a longer warmup when exercising in cold weather.
Lastly, if you feel tightness in your quadriceps while exercising, ever stop what you’re doing and rest. Don’t improve the power, frequency, or duration of your activity too rapidly, and be sure to build in rest because overuse injuries are more likely to occur. This will help stop another injury.
FAQ
How long accomplishes it take for a quadriceps strain to heal?
Minor to moderate quad strains will usually heal on their own, given sufficient time. Recovery for minor to medium quad strains is usually one to three weeks with limited movement. If the strained quad is extreme, it may require four to eight weeks to gain full recovery.
Can you walk with a quad strain?
During this acute stage, gently move the leg as you can tolerate. Don’t be forceful with the movement. Walking is usually the best way to support the area moving. Be sure to keep your steps shorter if you are undergoing pain.
How serious is a quad strain?
Your thigh may be swollen and bruised. If you have a bad strain, you may not be able to move your leg usually. A minor strain often recovers well with rest and other treatments. But an intense strain may need medical treatment.
Is the heating pad good for the strained quad?
A pulled muscle should first be treated using the R.I.C.E. method. During the first 72 hours, heat should be avoided to control increased swelling and inflammation. After about 72 hours, heat can be integrated into treatment to increase blood flow and aid the overall recovery process.
Should you massage a quad strain?
Exercising on an injured quad muscle can irritate the injury and prevent healing, or even cause the injury to become worse. No Massage. Massages can be useful for sore muscles but they will not help if the muscle is weakened. Massaging a quadriceps strain may aggravate the muscle more and lead to swelling.




2 Comments