Hyoid Bone
Introduction
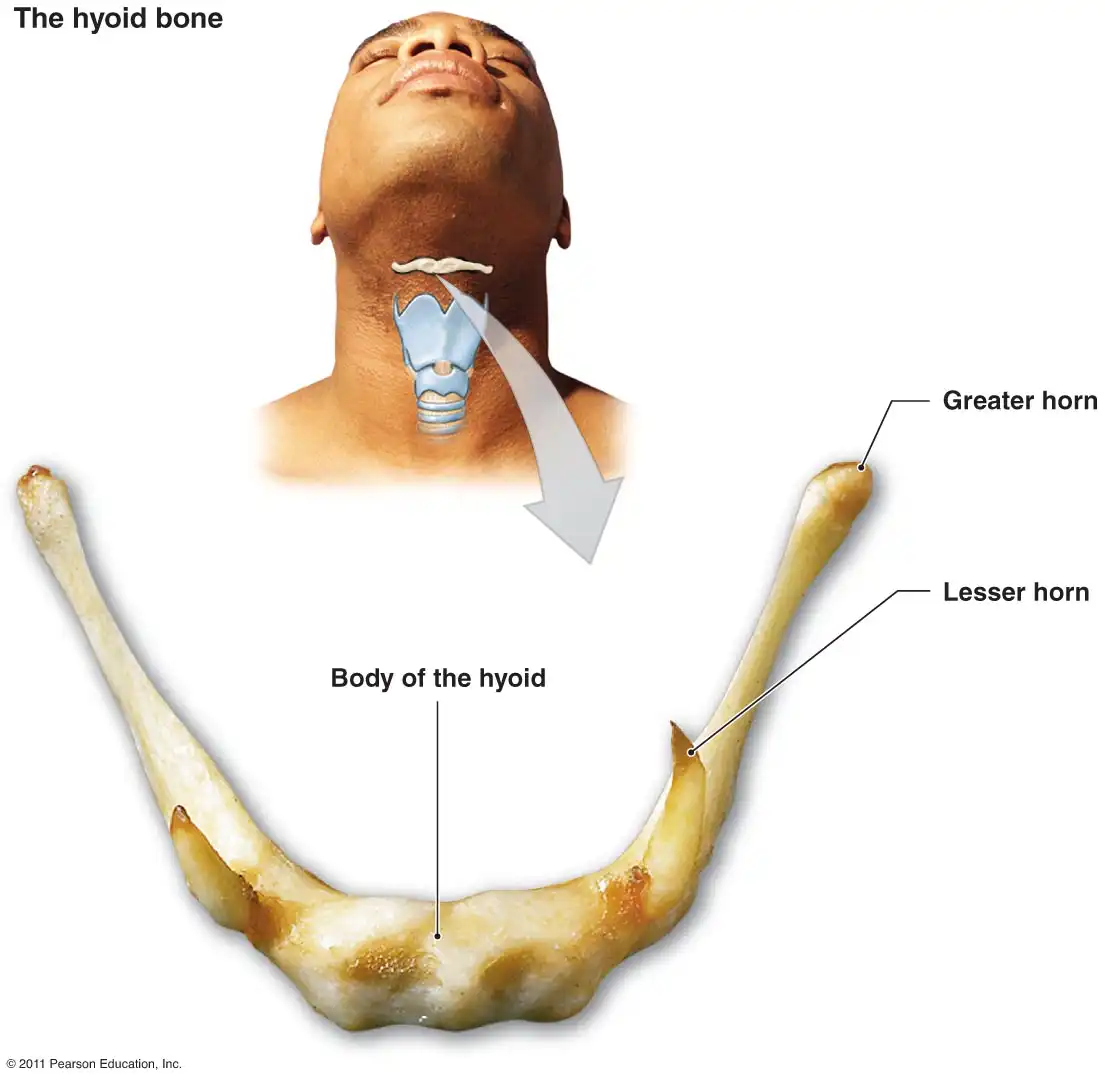
The hyoid bone is a small, U-shaped bone located in the upper neck of humans and other mammals. Despite its diminutive size, the hyoid plays an integral role in swallowing and speech. This unique bone has mystified anatomists and evolutionary biologists due to its distinctive shape and placement within the body.
As the only bone in the body not connected to other bones, the “floating” hyoid exhibits an evolutionary and developmental pathway, unlike any other skeletal element.
Anatomical Structure of the Hyoid Bone
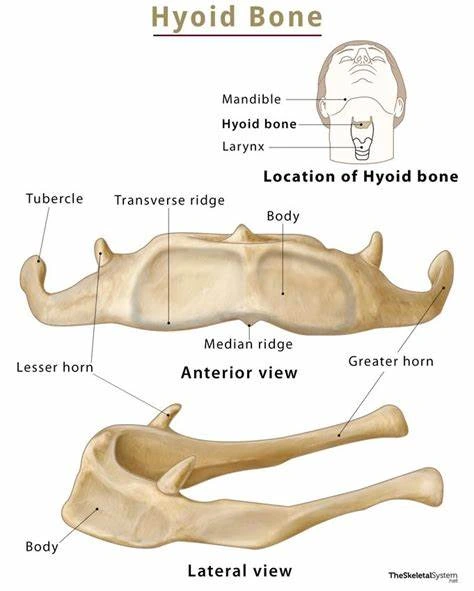
The hyoid bone has a unique shape and positioning, unlike any other bone. Located in the anterior midline of the neck, it has a central body with two pairs of horns or cornua projecting upward and backward. The larger cornua articulate with the styloid processes of the temporal bones bilaterally using tympanohyal ligaments.
The smaller lesser cornua connect to the thyroid cartilage through thyrohyoid membranes. Overall, the hyoid appears U-shaped or horseshoe-shaped.
Despite having no bony articulations, the hyoid interfaces with several structures. Ligaments and muscles suspend it from the styloid processes of the skull and the thyroid cartilage. The middle pharyngeal constrictor muscle attaches to the greater cornu, enabling the hyoid’s role in swallowing. Fascia connects the hyoid’s upper border to the base of the tongue, aiding tongue mobility. Multiple neck muscles are also inserted into the hyoid.
While the basic shape of the hyoid is consistent, natural variations exist. Differences occur in the length of the greater and lesser cornua, the width of the central body, and the angle between the body and greater cornua. Sexual dimorphism is also present, as the male hyoid is larger and more angular.
However, the biomechanical function remains identical between sexes. Understanding the anatomy and connections of the hyoid provides greater insight into its critical mechanical capabilities.
Muscular attachments of the hyoid bone
- Digastric Muscle: Attaches to the lesser cornu and depresses the hyoid bone during swallowing.
- Mylohyoid Muscle: Forms the floor of the oral cavity and elevates the hyoid bone.
- Geniohyoid Muscle: Originates on the mandible and elevates and pulls the hyoid bone anteriorly.
- Sternohyoid Muscle: Attaches the hyoid bone to the sternum and depresses the hyoid.
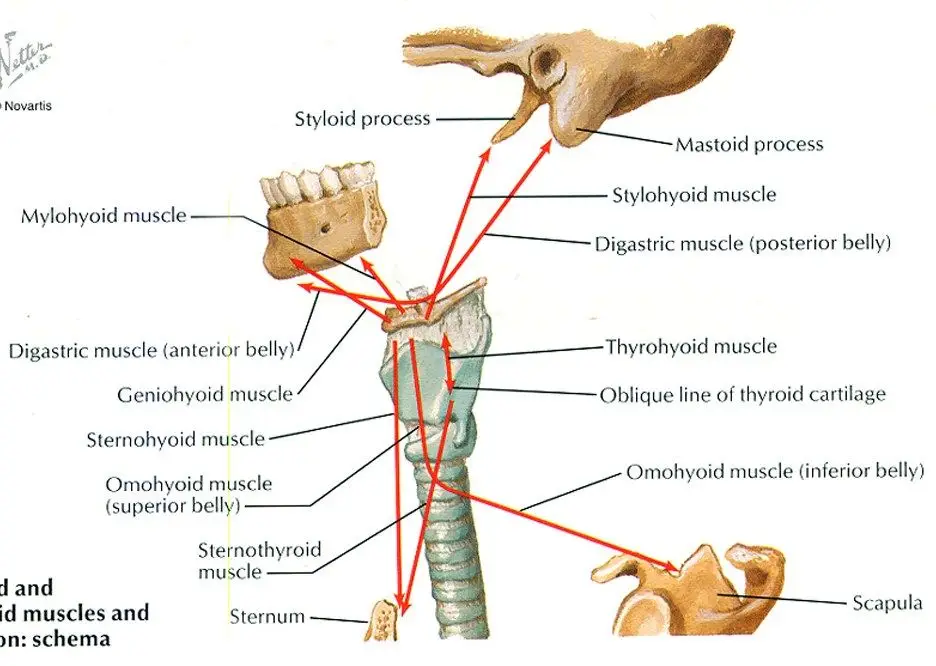
- Genioglossus Muscle: Fan-shaped tongue muscle originating from the upper hyoid body to move the tongue.
- Hyoglossus Muscle: Arises from the greater cornu and body of the hyoid and retracts the tongue.
- Omohyoid Muscle: Has superior and inferior bellies connected by an intermediate tendon attached to the hyoid body. Depresses the hyoid bone.
- Sternothyroid Muscle: Extends from the hyoid bone to the thyroid cartilage and depresses the larynx.
- Middle Pharyngeal Constrictor: Originates from the lesser cornu of hyoid and makes up part of the pharynx wall for swallowing.
Development and Formation of the Hyoid Bone
Embryological Development of the Hyoid Bone
Origins of the Hyoid Bone during Fetal Development
The hyoid bone begins developing during the fourth and fifth weeks of embryonic growth as mesenchymal tissue migrates from the branchial arches to the future hyoid site. Chondrification centers form from this tissue, laying down a cartilaginous model for each part of the future bone.
The body of the hyoid forms from the second pharyngeal or hyoid arch. The paired stylohyoid ligaments and lesser cornu originate from the third arch. The upper portion of the body and the greater cornu develop from dorsal sections of the fourth and fifth arches, respectively. By the end of the embryonic period, a cartilaginous hyoid exists in several segments with distinct developmental contributions.
Formation and Ossification Process of the Hyoid Bone
Intramembranous ossification converts the midline hyoid cartilage into bone starting in the third to fifth fetal months. This forms the body and fuses the segments into one structure. Endochondral ossification proceeds along the bilaterally paired greater and lesser cornua, replacing cartilage with bony tissue.
Ossification initiation occurs earlier in males, contributing to sexual dimorphism in hyoid size and shape. The timing of complete ossification is variable, ranging from early childhood to early adulthood. Although anatomical variations exist, the basic corrugated shape remains consistent.
Developmental Disorders and Abnormalities of the Hyoid Bone
Congenital anomalies of the hyoid are uncommon. Partial aplasia, duplication deformities, fusion of segments, and midline clefts can occur. Multiple ossification centers or persistent separation of segments are also reported. Such disorders may impair hyoid mobility or respiratory and swallowing functions.
Aging and Changes in the Hyoid Bone
Structural Changes in the Hyoid Bone with Age
After maturation, the hyoid bone undergoes age-related anatomical changes. Ossification expands at sites of muscle and ligament insertion. Density loss and occasional calcification or cavitation also occur over time. The synovial joints of the greater cornua exhibit degenerative alterations as well.
Degenerative Effects and Impacts on Functionality
Despite architectural changes with aging, the hyoid’s biomechanical performance typically remains intact. However, some correlation exists between hyoid modifications and increased prevalence of dysphagia, aspiration, and voice issues in the elderly. The reasons are likely multifactorial, but research is needed on whether age-specific hyoid changes directly contribute to such problems.
Functions of the Hyoid Bone
The hyoid bone facilitates several critical physiological processes, most notably swallowing and speech. Its muscular and ligamentous connections also influence respiration. Breakdown in hyoid mechanisms can therefore impair multiple systems.
Swallowing and Speech: The Key Role of the Hyoid Bone
Hyoid Bone and its Role in Swallowing Mechanisms
The hyoid provides an anchor for muscles that elevate the larynx during swallowing. This pulls the larynx under the tongue base and closes air passages to prevent aspiration. Hyoid mobility also assists tongue root retraction and pharyngeal contractions that propel the food bolus. Age or trauma-related stiffness reduces these actions, increasing dysphagia and aspiration risks.
Vocalization and Articulation: Hyoid Bone’s Involvement
Muscles attached to the hyoid modify the vocal fold tension required for pitch control. The hyoid also anchors tongue muscles needed for consonant and vowel production. Hyoid disorders may thus contribute to voice and speech deficits through several mechanisms.
The Impact of Hyoid Bone Disorders on Speech
Abnormalities in hyoid development or fracture call impair vocal and swallowing performance. Potential effects include hoarseness, articulation errors, reduced vocal stamina, tongue weakness, and aspiration. However, outcomes rely heavily on the nature and severity of structural damage.
Role in Breathing and Respiration
Hyoid Bone and Its Connection to the Upper Airways
Hyoid positioning impacts the dimensions of the oro- and laryngopharynx. Anterior hyoid displacement is correlated with increased collapsibility of pharyngeal air spaces. This places older individuals at higher risk for obstructive sleep apnea.
Influence on Airway Stability and Patency
Muscles inserted into the hyoid dilate the upper airways. During inspiration, the hyoid retracts via the geniohyoid muscles to widen the pharynx. Loss of this pharyngeal dilation through muscular dysfunction or hyoid fracture may potentiate airway obstructions.
Disorders and Breathing Difficulties Related to the Hyoid Bone
Hyoid bone anomalies can precipitate or exacerbate sleep-disordered breathing. While multifactorial, hyoid-related changes in airway caliber raise risks for sleep apnea across age groups. The impacts highlight the significance of the delicate hyoid bone in maintaining airway patency.
Hyoid Bone’s Role in Head and Neck Movement
Muscle Attachments and Actions
The hyoid serves as an attachment point for several infrahyoid muscles that act on the larynx, pharynx, and cervical spine. Key muscle groups include the sternohyoid, omohyoids, sternothyroid, and thyrohyoids. These muscles coordinate swallowing but also facilitate neck flexion and rotation.
Coordination in Eating, Turning the Head, and Yawning
Forward head flexion relying on the infrahyoid muscles assists in bringing food to the mouth. Contraction of the omohyoids and sternohyoids enables head turning by flexing the cervical spine. Yawning requires elevation of the hyoid bone by the digastric muscles as the jaw opens widely.
Dysfunctions and Its Impact on Basic Movements
Injuries restricting hyoid motion can limit neck mobility for eating or head orientation. Fibrosis acquiring muscle attachments hinders flexion required in yawning or changing head position. Such dysfunctions may manifest insidiously but can degrade the quality of life over time. Assessing hyoid involvement reveals an overlooked contributor to difficulties performing routine movements.
Clinical Implications and Disorders
Hyoid Bone Abnormalities and Pathologies
Congenital Anomalies and Developmental Malformations
Congenital hyoid disorders are uncommon outcomes of aberrant ossification, fusion, or cleavage. Documented anomalies include aplasia of segments, accessory ossicles, duplication deformities, midline clefts, and persistent unfused hypnoid elements.
Such malformations can profoundly impact the biomechanics of swallowing, speech, and respiration. If asymptomatic, anomalies may go undiagnosed unless incidental imaging findings.
Symptomatic cases often present with feeding difficulties, reflux, aspiration, or stridor in infancy or childhood. Surgical procedures to release tethered hyoid segments or stabilize unfused elements may be employed to minimize long-term morbidities and mortalities.
Dysphagia and Dysphonia: Hyoid Bone Disorders
Acquired disorders of the hyoid bone later in life increase the risks of dysphagia due to inadequate laryngeal elevation, tongue base retraction, and pharyngeal peristalsis needed for effective swallowing. Vocal fold adduction and tongue strength for vowel production and consonant articulation may also decline.
Complaints of swallowing difficulties, choking spells, hoarse voice, reduced vocal stamina, and impaired communication are common. These hyoid-related deficits severely reduce the quality of life.
When conservative therapies like diet modification or swallowing exercises fail, more invasive injections, implants, or surgical interventions could be trialed. However, multi-disciplinary approaches are ideal to target the various facets of disease progression.
Surgical Interventions and Remedial Procedures
In cases of severe hyoid impairment, surgical release of fused segments, fracture stabilization, reconstruction, or hyoid suspension may be recommended. However, operative candidacy depends on the patient’s symptoms, overall health status, integrity of surrounding structures, and likelihood of functional improvement.
Post-operative management focuses on protecting healing tissues while working to strengthen hyoid musculature and range of motion. Conservative rehabilitative approaches utilize swallowing therapies, voice exercises, oral appliances, and dietary strategies to circumvent structural deficits when possible.
Determining the optimal procedures for hyoid disorders requires individualized consideration of the relative risks versus the potential functional rewards.
Sleep Apnea and Hyoid Bone Position
Understanding Sleep Apnea and Its Relationship with the Hyoid Bone
Sleep apnea syndrome is characterized by repetitive collapse of the upper airway during sleep, causing temporary hypoxia and frequent arousals. While multifactorial, anterior displacement of the hyoid bone is correlated with increased pharyngeal collapsibility that can precipitate apneic events. This relationship is strongest for obstructive sleep apnea (OSA) but may also contribute to central apnea mechanisms via the hypopharynx.
Impact of Hyoid Bone Displacement on Sleep Apnea Symptoms
Anterior shifting of the hyoid bone predicts several markers of OSA severity, including oxygen desaturation indices, hypertension, and metrics of sleep fragmentation. The association stems from the hyoid’s role in maintaining pharyngeal patency.
Anterior movement narrows retropalatal and retroglossal spaces, promoting airway occlusion. Patients may then suffer fatigue, snoring, witnessed apneas, and other sequelae of sleep disruption.
Treatment Approaches Targeting Hyoid Bone Position
As the hyoid bone proves integral for airway stability, therapies moving it posteriorly demonstrate promise for OSA patients. Oral appliances like mandibular advancement devices indirectly shift the hyoid backward via musculature. Custom appliances also directly contact and retain the hyoid.
Early research shows such interventions may shrink airway cross-sectional areas and reduce apnea events. Future approaches could apply transcutaneous electrical stimulation to consciously retract and elevate the hyoid during sleep. Targeting the position of this singular bone may significantly improve breathing in sleep apnea patients.
Trauma and Fractures of the Hyoid Bone
Recognizing and Assessing Hyoid Bone Fractures
Hyoid bone fractures result from extensive neck hyperextension or compression injuries and occur in motor vehicle collisions, sports impacts, strangulation attempts, and other assault cases. Due to its protected location, significant force is required to break the hyoid. Clinical features prompting evaluation include neck pain, dysphagia, odynophagia, dysphonia, implied trauma, and visible ecchymosis above the hyoid.
Imaging confirms the diagnosis, but X-rays miss up to 30% of fractures while CT scans and MRIs have greater accuracy. Complete assessments denote fracture location, displacement degree, and tissue integrity.
Associated Injuries and Forensic Implications
Given the posterior ligamentous attachments and anterior musculature connections, hyoid fractures signal high-velocity impacts transmitted to the neck. Their presence warrants expanded trauma imaging to identify possible concomitant spine, vascular, thoracic, and traumatic brain injuries.
Hyoid fractures also have immense forensic importance as markers of strangulation violence. Documentation is mandatory for the investigation of possible assault and homicide cases.
Management and Healing Process of Hyoid Bone Fractures
The hyoid healing process varies by patient age, fracture displacement, site integrity, and comorbidities. Minimally displaced fractures carry a good prognosis with conservative treatment emphasizing analgesia, dietary modifications, and activity limitations. However, displaced medial fragments often necessitate open reduction and internal fixation to prevent nonunion and chronic pain or dysphagia.
Precise realignment promotes mucosal healing and restoration of the critical functions relying on hyoid mobility. Despite sensitivity, most hyoid fractures heal well if given proper acute management.
Imaging Tests
- X-ray – Can visualize hyoid fractures but misses 30% of fractures
- CT scan – More accurate for fracture and better shows soft tissues
- MRI – Provides clear images of anatomical relations without radiation
- Videofluoroscopic swallow study – Documents biomechanics of swallowing
- Laryngoscopy – Visualizes laryngeal structure and movement
- Cephalometry – Defines hyoid bone position relative to airway spaces
These imaging exams are used to confirm and characterize hyoid bone fractures, congenital anomalies, acquired degenerative changes, positional disorders relative to the airway, and impaired mobility contributing to swallowing pathologies or speech deficits. The tests complement a full history and clinical examination to guide appropriate treatment.
Common Symptoms
- Dysphagia (difficulty swallowing)
- Odynophagia (painful swallowing)
- Aspiration or choking spells
- Hoarse, weak voice or vocal fatigue
- Impaired speech articulation
- Neck or throat pain
- Stiffness or limited range of motion
Summary
The hyoid bone is a unique U-shaped bone of the neck with an important role in swallowing and speech. Its suspended position and distinctive connections set it apart from the rest of the skeleton.
During embryonic development, the hyoid forms from cartilage precursors derived from multiple pharyngeal arches. Intramembranous and endochondral ossification establish the bony structure early in fetal growth. Anatomical variations occur but typically do not obstruct the hyoid’s critical functions.
The hyoid provides attachments for the tongue and pharyngeal muscles, permitting intricate movements in swallowing bolus transfer, and vocalization. Dysphagia and dysphonia can result from architectural anomalies or traumatic fractures of the hyoid system. Forward displacement of the hyoid bone also narrows retropharyngeal airways, increasing the risks of obstructive sleep apnea.
Diagnosis of hyoid-related dysfunctions often necessitates imaging for precise assessments. Treatment approaches are tailored to the specific deficit and available interventions for that region. Protecting the delicate hyoid mechanisms supports nutritional intake, communication, and respiration—all functions vital to well-being.
FAQs
What is the hyoid bone’s location in the human body?
The hyoid bone is located in the anterior midline of the upper neck, just below the mandible and above the thyroid cartilage. It is the only bone in the body not articulating with other bony structures.
How does the hyoid bone contribute to swallowing and speech?
The hyoid anchors muscles of the tongue and pharynx needed for bolus propulsion and airway protection when swallowing. It also assists in vocal fold adduction for pitch and volume adjustments used in speech.
What are the most common disorders related to the hyoid bone?
Congenital malformations, secondary dysfunctions causing dysphagia/dysphonia, traumatic fractures, and anterior positional shifts contributing to obstructive sleep apnea are among the most frequently occurring hyoid disorders.
How are swallowing disorders diagnosed and treated?
Videofluoroscopy, endoscopy, and functional endoscopic evaluation of swallowing assess biomechanics. Management options include diet modification, posture strategies, muscle-strengthening exercises, stimulator devices, and surgery.
Can the hyoid bone’s position influence sleep apnea symptoms?
Yes, anterior movement of the hyoid bone limits airway caliber and is associated with more severe presentations of obstructive sleep apnea. Appliances that reposition the hyoid may help reduce respiratory events.
What is the management approach for hyoid bone fractures?
Most hyoid fractures heal well with conservative measures like a soft diet and activity limitation. However, significantly displaced fragments might require open reduction and internal fixation to realign the ends and prevent nonunion.
References
- Britannica, T. Editors of Encyclopaedia (2024, January 11). hyoid bone. Encyclopedia Britannica. https://www.britannica.com/science/hyoid-bone
- Hyoid bone. (2023, July 5). Kenhub. https://www.kenhub.com/en/library/anatomy/hyoid-bone
- Professional, C. C. M. (n.d.). Hyoid Bone. Cleveland Clinic. https://my.clevelandclinic.org/health/body/hyoid-bone
- Cpt, A. A. (2022, June 1). The Anatomy of the Hyoid Bone. Verywell Health. https://www.verywellhealth.com/hyoid-bone-anatomy-296913