
REFLEXES : Types and Testing
Introduction
A reflex is an involuntary and relatively stereotyped response to a specific sensory stimulus. There are many types of reflexes and every healthy person has them. In fact, we’re born with most of them.
eg. When a person accidentally touches a hot object, they automatically jerk their hand away without thinking. Reflex arcs act on an impulse before that impulse reaches the brain.
Two features of the sensory stimulus are particularly important in shaping the reflex response. Second the strength of the stimulus determines the amplitude of the response. Reflex therefore are graded behaviors.
Definition
A reflex is an involuntary and nearly reactionary movement in response to a stimulus. The reflex is an automatic response to a stimulus that does not receive or need conscious thought as it occurs through a reflex arc. Reflex arcs act on an impulse before that impulse reaches the brain.
Reflex arc can be :
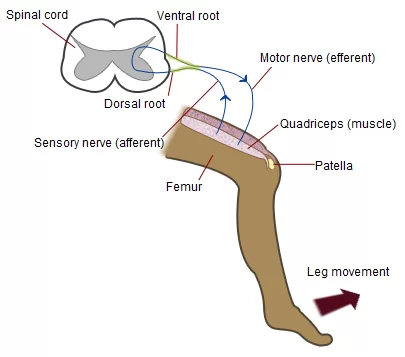
- Monosynaptic eg. contain only two neurons, a sensory and a motor neuron. Examples of monosynaptic reflex arcs in humans include the patellar reflex and the Achilles reflex.
- Polysynaptic eg. multiple inter-neurons (also called relay neurons) that interface between the sensory and motor neurons in the reflex pathway.
Video Presentation :
Types of Reflexes
Reflexes are divided into Superficial and Deep reflexes.
- Superficial reflexes: Plantar response, abdominal reflex, cremastic reflex, corneal reflex.
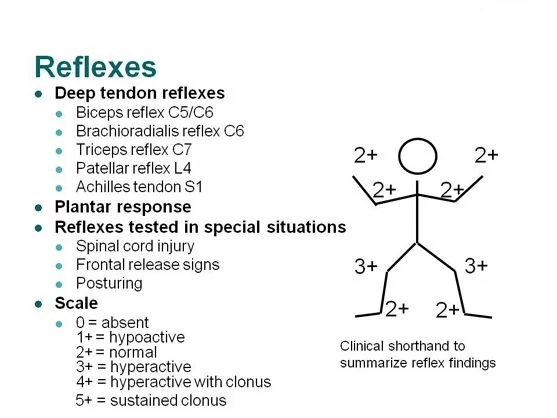
- Deep reflexes: Biceps, Brachioradialis, Triceps, Knee jerk, and ankle jerk.
Reflexes tested include the following:-
- Biceps (innervated by C5 and C6)
- Radial brachialis (by C6)
- Triceps (by C7)
- Distal finger flexors (by C8)
- Quadriceps knee jerk (by L4)
- Ankle jerk (by S1)
- Jaw jerk (by the 5th cranial nerve)
Technique for testing reflexes
- The muscle group to be tested must be in a neutral position (i.e. neither stretched nor contracted).
- The tendon attached to the muscles which is/are to be tested must be clearly identified. Place the extremity in a position that allows the tendon to be easily struck with the reflex hammer.
- To easily locate the tendon, ask the patient to contract the muscle to which it is attached. When the muscle shortens, you should be able to both see and feel the cord-like tendon, confirming its precise location.
- Strike the tendon with a single, brisk, stroke. You should not elicit pain.
Grades of Reflexes
- 0 — No evidence of contraction
- 1+ — Decreased, but still present (hypo-reflexic). Hyporeflexia is generally associated with a lower motor neuron deficit (at the alpha motor neurons from the spinal cord to muscle) eg Guillain–Barré syndrome
- 2+ — Normal
- 3+ — Super-normal (hyper-reflexic) Hyperreflexia is often attributed to upper motor neuron lesions eg Multiple sclerosis
- 4+ — Clonus: Repetitive shortening of the muscle after a single stimulation.
Abnormal Reflexes (Pathologic Reflexes)
- Pathologic reflexes (eg. Babinski, rooting, grasp) are reversions to primitive responses and indicate loss of cortical inhibition.
Other Reflexes :
- Clonus (rhythmic, rapid alternation of muscle contraction and relaxation caused by sudden, passive tendon stretching) testing is done by rapid dorsiflexion of the foot at the ankle. Sustained clonus indicates an upper motor neuron disorder.
Significance of Superficial Reflexes in Physiotherapy
- Abdominal reflex is stimulated by stroking around the abdomen which helps in determining the level of CNS lesion.
- Cremastic reflex: It is elicited when the inner part of the thigh is stroked in males (Geigel reflex is the counterpart in females). This reflex helps in the evaluation of acute scrotal pain and assessing for testicular torsion(associated with loss of reflex).
- Corneal reflex: It is elicited by gentle stroking on the cornea with a cotton swab. This reflex mainly helps in knowing the damage peripherally to either the trigeminal nerve (V) or facial nerve (VII) nerve will disrupt the corneal blink circuit.
- Plantar reflex: abnormal reflex indicates metabolic or structural abnormality in the corticospinal system upstream from the segmental reflex.
Deep reflex :
Jaw Jerk :
Place the tip of your index finger on a relaxed jaw, one that is about one-third open. Tap briskly on your index finger and note the speed as the mandible is flexed (see Chapter 61 on the trigeminal nerve).
Biceps Reflex :
The forearm should be supported, either resting on the patient’s thighs or resting on the forearm of the examiner. The arm is midway between flexion and extension. Place your thumb firmly over the biceps tendon, with your fingers curling around the elbow, and tap briskly. The forearm will flex at the elbow.
Triceps Reflex :
Support the patient’s forearm by cradling it with yours or by placing it on the thigh, with the arm midway between flexion and extension. Identify the triceps tendon at its insertion on the olecranon, and tap just above the insertion. There is extension of the forearm.
Brachioradialis Reflex :
The patient’s arm should be supported. Identify the brachioradialis tendon at the wrist. It inserts at the base of the styloid process of the radius, usually about 1 cm lateral to the radial artery. If in doubt, ask the patient to hold the arm as if in a sling—flexed at the elbow and halfway between pronation and supination—and then flex the forearm at the elbow against resistance from you. The brachioradialis and its tendon will then stand out.
Place the thumb of the hand supporting the patient’s elbow on the biceps tendon while tapping the brachioradialis tendon with the other hand. Observe three potential reflexes as you tap.
Brachioradialis reflex :
flexion and supination of the forearm.
Biceps reflex :
flexion of the forearm. You will feel the biceps tendon contract if the biceps reflex is stimulated by the tap on the brachioradialis tendon.
Finger jerk :
flexion of the fingers.
The usual pattern is for only the brachioradialis reflex to be stimulated. But in the presence of a hyperactive biceps or finger jerk reflex, these reflexes may be stimulated also.
Finger Jerk:
Have the patient gently curl his fingers over your index finger, much as a bird curls its claws around the branch of a tree. Then raise your hand, with the patient’s hand now being supported by the curled fingers. Tap briskly on your fingers so that the force will transmit to the patient’s curled fingers. The response is a flexion of the patient’s fingers.
Knee Jerk :
Let the knees swing free by the side of the bed, and place one hand on the quadriceps so you can feel its contraction. If the patient is in bed, slightly flex the knee by placing your forearm under both knees by contraction of the quadriceps with extension of the lower leg. If the reflex is hyperactive there is sometimes concomitant adduction of the ipsilateral thigh. Adduction of the opposite thigh and extension of the opposite lower leg also can occur simultaneously if those reflexes are hyperactive. Note that this so-called crossed thigh adduction or leg extension tells you that the reflexes in the opposite leg are hyperactive. They tell you nothing about the state of the reflex in the leg being tested. Use the Jendrassik maneuver if there is no response.
Ankle Jerk :
With the patient sitting, place one hand underneath the sole and dorsiflex the foot slightly. Then tap on the Achilles tendon just above its insertion on the calcaneus. If the patient is in bed, flex the knee and invert or evert the foot somewhat, cradling the foot and lower leg in your arm. Then tap on the tendon.
If no response is obtained, have the patient face a chair and kneel on it with the knees resting against the back of the chair, the elbows on the top of the back, and the feet projecting over the seat.
First, dorsiflex the foot slightly and tap on the tendon. Use the Jendrassik maneuver if this doesn”t work. This position is well suited to observing the relaxation phase of the reflex in patients with suspected thyroid disease.
Infant Reflexes :
Infant Reflexes are seen with birth, Many infant reflexes disappear as the child grows older, although some remain through adulthood. A reflex that is still present after the age when it would normally disappear can be a sign of brain or nervous system damage.
Infant reflexes are responses that are normal in infants, but abnormal in other age groups. Physiotherapists check reflexes to determine if the brain and nervous system are working well. Some reflexes occur only in specific periods of development. The following are some of the normal reflexes seen in newborn babies
- Moro reflex
- Sucking reflex (sucks when the area around the mouth is touched)
- Grasp reflex (Stroking the palm of a baby’s hand causes the baby to close his or her fingers in a grasp)
- Tonic neck reflex (When a baby’s head is turned to one side, the arm on that side stretches out and the opposite arm bends up at the elbow)
- Startle reflex (pulling arms and legs in after hearing loud noise)
- Stepping reflex (stepping motions when the sole of the foot touches a hard surface)
Other Related Article :




One Comment