
T4 Syndrome and Physiotherapy Management
What is a T4 Syndrome?
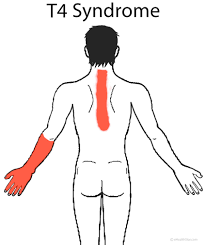
T4 Syndrome is a condition that affects Thoracic vertebrae level T4, in which you feel pain, Paresthesias, and numbness, in the upper extremity with or without associated symptoms such as headaches and upper back stiffness.
- It is a collection of symptoms resulting from autonomic dysfunction in the upper thoracic spine.
- A typical thoracic vertebra has a total of six joints with neighboring vertebrae: four synovial joints and two symphyses.
- Although the movement between any two vertebrae is limited, the summation of movement among all vertebrae results in a large range of movement by the vertebral column.
There are two major types of joints between the vertebrae :
- Symphyses between vertebral bodies
- Synovial joints between articular processes
- The synovial joint between superior and inferior articular processes on the neighboring vertebrae is the zygapophysial joints. A Thin articular capsule attached to the margins of the articular facets covers each joint. In thoracic regions, the joints are oriented vertically and limit flexion and extension, but facilitate rotation
- Vasomotor nerve fibers descend in the spinal cord and emerge in the ventral horns and roots. These fibers pass the dorsal root ganglia as it sits in the intervertebral foramen. Next, they emerge as part of a spinal segmental nerve.
- Sympathetic fibers leave the segmental nerve and join the sympathetic chain. Then it travels down the neck of the ribs with variable areas of the ganglia.
- Branches from the sympathetic chain pass over the costovertebral joints to supply the heart, esophagus, and abdominal viscera. It is not uncommon for these branches to become stretched or affected by neighboring osteophytes.
- The sympathetic chain fibers ascend or descend a variable number of segments synapse in a ganglion, and leave the chain to join a peripheral nerve.
Examination
- There is no evidence about examinations that include T4 syndrome. Unfortunately, a great deal of literature exists on shoulder pain, yet little exists in the area of periscapular or rib pain But it is almost certain that the intervertebral joint around T4 is hypermobile in patients with T4 syndrome.
- We can test this by testing the active range of motion (AROM) of the cervical, shoulder, and trunk regions to determine pain-provoking movements.
- Furthermore, we can examine the differential diagnosis to exclude. Also, postural observation from the posterior, lateral, and anterior aspects can be useful, but the reliability of visual observation has not been reported. Deviations from an ideal posture were noted.
- Manual muscle testing (MMT) and a gross sensory examination (to determine whether nerve root or peripheral nerve lesions were present) can also be helpful, but neither of them has been validated. Also, palpation of the cervical, shoulder, and upper trunk regions was assessed
Clinical Presentation
- Symptom onset may coincide with a new job or hobby, especially those that require frequent stooping or bending (electricians, surgeons, and assembly-line workers).
- Frequent posturing in front of the computer has also been implicated. Symptoms are often diffuse and located in the neck, head, and upper extremities (unilateral or bilateral)
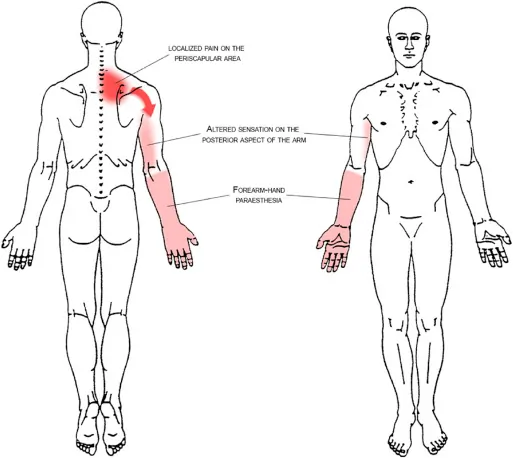
- Typical signs and symptoms include headaches, neck, and arm pain, and paresthesia. These signs and symptoms could be the result of thoracic dysfunction and its influence on the sympathetic nervous system.
Other symptoms that can occur:
- paraesthesias to the upper limbs and hands -> all five digits
- hand and forearm numbness
- upper extremity coldness
- Hands feel hot or cold
- hand clumsiness
- heaviness in the upper extremities
- hands feel and may objectively be swollen
- upper extremity pains associated with or without headaches and upper back stiffness
- intermittent posterior pain or pain around the scapula
- refer pain (Radiating nerve pain)
- pain often described as crushing or like a tight band
- sometimes these symptoms are present:
- pain and stiffness ->around the chest wall with pain anterior and posterior
- interscapular pain or stiffness
- worse pain at night
- The pain can become sharp and stabbing and increase with quick trunk or upper-extremity movements, deep breathing, coughing or sneezing, and changing positions in bed Sympathetic fibers can pass distally leaving the peripheral nerve to join an artery in the neurovascular bundle.
- Here they assist with the control of blood pressure via vasoconstriction.
- It is thought that the head and neck are provided with the sympathetic outflow from T1 to T4. The upper trunk and extremities are thought to be supplied by T2 to T5. Symptoms in the neck, head, and upper extremities are common.
Differential Diagnosis
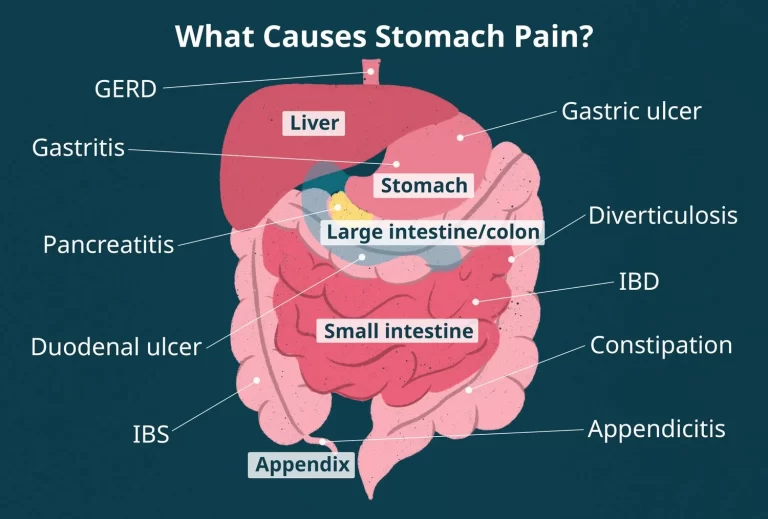
For proper diagnosis, Doctor should be asked you to rule out any related condition mainly cardiac, respiratory, or visceral conditions.
Thoracic pain is also most common with cancer metastases so prior to starting manual therapy treatment, be sure to rule out cancer as a cause of pain.
After that it is also important to rule out other related different conditions especially in potential T4 syndrome as this is a rarely seen condition therefore other related conditions are:
- Thoracic Outlet Syndrome
- Carpal tunnel syndrome
- Ulnar nerve entrapment
- Cervical disc disease or degeneration
- Visceral disease
- Neurological disease
- Fibromyalgia
- Myelopathy
- Complex Regional Pain Syndrome
- Cardiac disease
Medical Treatment:
Symptomatic pain-relieving drugs mainly NSAIDs help to relieve pain. if neurological symptoms are present Doctors prescribe gabapentinoids
If pain is not relieved Doctor also prescribes intramuscular injections of 1 to 2 mL of 0.5% bupivacaine at the 4th thoracic paraspinal level.
Physiotherapy and Medical treatment are the initial main treatment options.
Physiotherapy Management :
- Thoracic joint mobilisation techniques are the basics of a treatment plan in patients with T4 syndrome.
- Furthermore it’s beneficial to incorporate soft tissue mobilisation and stress/anxiety management techniques into the treatment seeing the positive effect at the sympathetic level.
- As with many chronic patients, exercise therapy needs to be included in the rehabilitation process.
- Soft tissue mobilisations result in improved tolerance to pressure and help with reducing stress.
- In the spinal region where the myofascial restrictions can be found during the examination, the gentle skin rolling technique can be used to restore normal fascial mobility These myofascial techniques seem to have positive effects on physical function, fascial mobility, postural stability, and anxiety level
- Thoracic posterior-anterior mobilisation seems to be effective on patients with T4 syndrome, this because mobilisations have an analgesic mechanism by exciting the sympathetic system.
- In a recent randomised control trial of Pete Jowsey et al. 36 healthy subjects (18–35 years) were randomly assigned to two groups (validated placebo intervention on skin conductance or treatment intervention) and provided evidence that a grade III postero-anterior rotatory joint mobilisation technique (treatment intervention) applied to the T4 vertebra at a frequency of 0.5 Hz can produce sympathoexcitatory effects in the hands of the subjects.
- In addition to the previous treatments, education about postural correction and home exercises should be given. The combination of patient education and mobilisations can be interesting to consider for dealing with patients with long-lasting symptoms.
- The study of Defranca et al. investigated the effect of joint manipulation, stretching, and strengthening exercises directed at the upper thoracic dysfunctional segments as a treatment for the T4 syndrome.
- Also Stacie J Fruth mentioned this sort of home exercises as a part of the treatment in her case report on T4 syndrome
- Passive stretch for middle trapezius muscle and rhomboideus muscles
- Alternate stretch for middle trapezius and rhomboideus muscles
- Trunk rotation stretch in sitting position
- Exercise for strengthening postural muscles. The patient presses arms into wall (arrows) while retracting scapulae.
- Passive stretch for middle trapezius and rhomboideus muscles.

Conclusion:
Glove-like pain, Paresthesias, and numbness, in the upper extremity with or without associated symptoms such as headaches and upper back stiffness, indicate T4 Syndrome. Manipulation and Symptomatic pain-relieving drugs and exercise of the dysfunctional upper thoracic spine help to these symptoms.
FAQ
What should you do if you have T4 syndrome?
Medical treatment with Physiotherapy treatment and exercise is a very good option and therefore it is important to consult your Doctor as well as a physiotherapist when you feel any of the above-mentioned symptoms.
You should also avoid painful activity and movement that increase your other neurological symptoms. Use of an Ice pack at Home on the affected area may help to relieve pain and swelling. Pain-relieving medicines may be helpful during the early days so that you can continue with your normal day-to-day activity.
What shouldn’t you do if you have T4 syndrome?
If you are diagnosed with T4 syndrome, you should avoid painful activities such as twisting, bending, and heavy lifting as this will increase your condition. Resting from the painful activity will help for the faster recovery of the affected area.
Long Driving and long sitting position should be reduced as much as possible to relieve stress on the affected T4 spine. If you have to drive or sit for a longer period, a good posture with breaks at regular intervals is highly useful and this can be done by sitting in a straight back chair with a fully supported pillow in your back that supports your spine.

One Comment